
Abstract
Objectives:
To investigate whether Hispanic immigrants with sleep disturbance showed improvements with auriculo-acupuncture mediated by emotional stress.
Design:
Single-blind randomized clinical trial.
Settings/Location:
Community.
Subjects:
Sixteen Hispanic male (N = 4) and female (N = 12) volunteers.
Interventions:
Bi-weekly intervention for eight total treatments of National Acupuncture Detoxification Association (NADA) auriculo-acupuncture or sham.
Outcome Measures:
Emotional distress and sleep measures were completed Baseline, Mid- (four treatments), and Follow-up (eight treatments). Comparisons between Groups and within sessions using Mixed-Model ANOVA; linear regression assessed emotional stress and sleep association.
Results:
Significant within-subjects effect of Session (p's <.05) with significant differences Baseline/Mid-Way and Baseline/Final (p's <.05). Linear Regression showed significant positive associations at Baseline.
Conclusions:
Community auriculo-acupuncture may improve sleep and emotional stress in Hispanic immigrants.
Introduction
Hispanics immigrants are a racial/ethnic minority facing sociocultural stressors associated with their marginalized status in the United States. 1 The prevalence of reported ethnic discrimination among U.S. Hispanics is as high as 78%. 2 Sleep disturbances such as trouble falling asleep, disrupted sleep, and early morning awakenings are prevalent and may be related to stress and challenging environmental conditions. 3 Emotional stress may be an important underlying factor contributing to their sleep disturbance. 1,4,5 Auriculo-acupuncture is a potential treatment for reducing emotional stress and thus improving sleep in Hispanic immigrants.
Systematic reviews support the use of acupuncture for anxiety and depression. 6 Studies suggest that auriculo-acupuncture 7 is an effective intervention in reducing stress and and significantly improves depression, anxiety, and anger. 8 Community acupuncture is more socioeconomically diverse than private acupuncture and potentially more accessible. 9 This study serves as a preliminary investigation into the efficacy of acupuncture for decreasing sleep disturbance through mitigating emotional stress to inform future larger scale intervention and comparison studies.
Research objectives were to investigate whether (1) Hispanic immigrant men and women with self-reported sleep disturbance show improvements in sleep and emotional stress with auriculo-acupuncture and (2) levels of emotional stress mediated changes in sleep outcomes associated with acupuncture.
Materials and Methods
Study recruitment and participants
All participants provided written informed consent before study enrollment. All procedures were in accordance with the ethical standards of the Helsinki Declaration of 1975 and met IRB approval [Solutions IRB (approval no. #2019/01/16)]. Participants were recruited from the larger Talbot County, MD, area through flyers and community outreach. Adult men and women of ages 18–64 years self-identifying as Hispanic/Latino immigrants and reporting sleep problems participated.
Participants were randomly assigned to National Acupuncture Detoxification Association (NADA) auriculo-acupuncture protocol or sham acupuncture control in a single blind procedure. Groups were coded by a colleague uninvolved with the study that was kept in a locked file drawer and used for assignment. Subjects were paid $24.00 for the first session, $12.00 for all subsequent sessions.
Intervention
The auriculo-acupuncture treatment followed a well-established and commonly used protocol developed by the NADA. 10 Acupuncture was performed by a licensed acupuncturist. Acupuncture needles were sterile, single use, stainless steel shafts of 0.20 mm diameter and 7.0 mm length provided in sterile packages. For the NADA auriculo-acupuncture group, five fine-gauge, sterilized, one-time-use auriculo-acupuncture needles (Fig. 1) were inserted at the five points of the NADA protocol (Shen men, sympathetic autonomic, lung, liver, and kidney points) bilaterally.
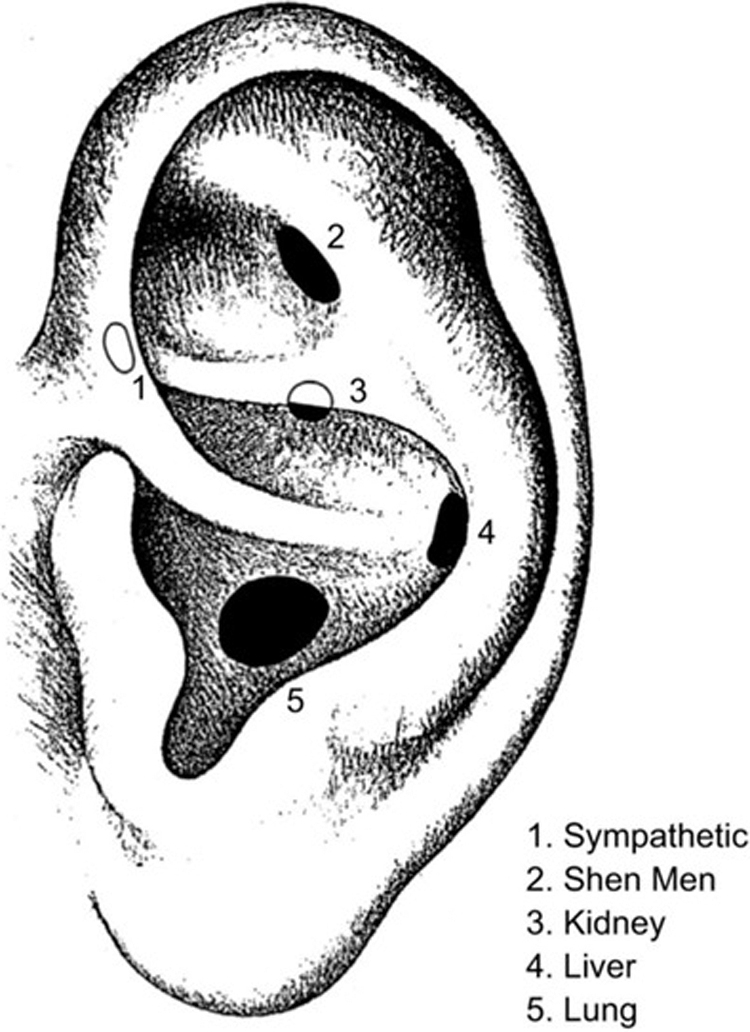
NADA protocol points: 1. Sympathetic; 2. Shen Men; 3. Kidney; 4. Liver; and 5. Lung. NADA, National Acupuncture Detoxification Association.
Sham control auriculo-acupuncture group participants had five auriculo-acupuncture needles inserted around the helix of the ear. Participants in each group received bilateral sham control or NADA auriculo-acupuncture biweekly while seated together in a large quiet room of up to six participants. Once all participants' needles were inserted, participants remained seated with the needles in for 30 min and were instructed to focus on their breathing and relax with dim lights and music. Needles were removed at the end of the 30 min.
Study design
See Table 1 for study timeline and procedures. Self-reported emotional stress and sleep were assessed before, midway, and after the 4-week intervention. The consenting process occurred immediately before study initiation, the acupuncturist was introduced, the procedure explained, and participants were encouraged to ask questions. A Spanish language translator was present. Participants completed the demographics form including age, gender, racial/ethnic origin, and marital status. The following forms were completed at baseline, midway (week 3), and at follow-up (week 5) to characterize sleep, sleep disturbance, emotional stress, and psychological stress; forms have been evaluated for use in Spanish-translated forms.
Study Timeline and Procedures
AIS, Athens Insomnia Scale; ESS, Epworth Sleepiness Scale; NADA, National Acupuncture Detoxification Association; PSQI, Pittsburgh Sleep Quality Index; PSS, Perceived Stress Scale.
Epworth Sleepiness Scale (ESS) 11 : 8-item questionnaire measuring daytime sleepiness with ratings of likelihood of falling asleep in eight different contexts on a 4-point scale (0–3); scores range from 0 to 24. Excessive daytime sleepiness is defined as an ESS score >10.
Athens Insomnia Scale (AIS) 12 : Assesses sleep difficulty with eight items: five for sleep disturbance and three for daytime consequences.
Pittsburgh Sleep Quality Index (PSQI) 13 : Assesses sleep quality over the past month. Global score and seven subscale scores: sleep quality, latency, duration, efficiency, disturbances, sleep medication, and daytime dysfunction.
Emotional Distress Scale (EDS) 14 : Measures mood distress with brief item sets of mood descriptors indicating the extent experienced a particular feeling during the past week, including today, selecting from response choices that range from “not at all” (1) to “extremely” (5). A distress composite score is computed on the average of anxiety, depression, and anger.
European Spanish Version of the Perceived Stress Scale (PSS) 15 : 14 items assessing perceived stress during the past month with a 5-point response scale (0 = never, 1 = almost never, 2 = once in a while, 3 = often, 4 = very often). Higher scores indicate higher stress. The study STROBE checklist and Study Flow Chart are included as Supplementary Data S1 and S2.
Data analysis
Aim 1: Self-reported sleep scales (ESS, AIS, and PSQI) and emotional distress scales (EDS and PSS) were compared between groups pre-, mid-, and post-treatment using Mixed-Model ANOVA with Between factor Treatment Group (sham control or NADA) and within group factor session (baseline, midway, and follow-up).
Aim 2: Linear regression was used to assess associations with (1) emotional stress (EDS and PSS) and sleep scores that showed significant changes in the ANOVA (AIS, PSQI, or ESS) at baseline, midway, or follow-up. Linear regression was performed with the sleep scores (AIS, PSQI, or ESS) as the y-input and the emotional stress measures (EDS and PSS) as the x-input.
Results
Participants
Sixteen Hispanic/Latino male (N = 4) and female (N = 12) volunteers participated in the study [NADA, N = 8, mean (SD) age = 41 years (16); sham control, n = 8; mean (SD) age = 42 years (17)]. Ten volunteers completed all 9 sessions: 5 volunteers' participation ended after 6 sessions due to COVID-19; 1 volunteer completed 3 sessions and withdrew due to work. Preliminary analyses on the first 10 subjects who completed all 9 sessions showed no significant changes after the fifth session for either group on any measure: a similar pattern is expected to have emerged for the last six for whom only baseline and midway point assessments were collected. Intent to Treat was used for all analyses for missing data for the final session.
Aim 1
Mixed-Model ANOVAs for sleep measures ASI and PSQI and emotional stress measures EDS and PSS showed significant within-subjects effect of session (p's < 0.05) (Fig. 2). Post hoc t-tests for main effects of session showed significant differences between baseline/midway and baseline/final for ASI, PSQI, EDS, and PSS measures (p's < 0.05); there was not a significant difference between midway and final sessions (p > 0.05) for any measure.
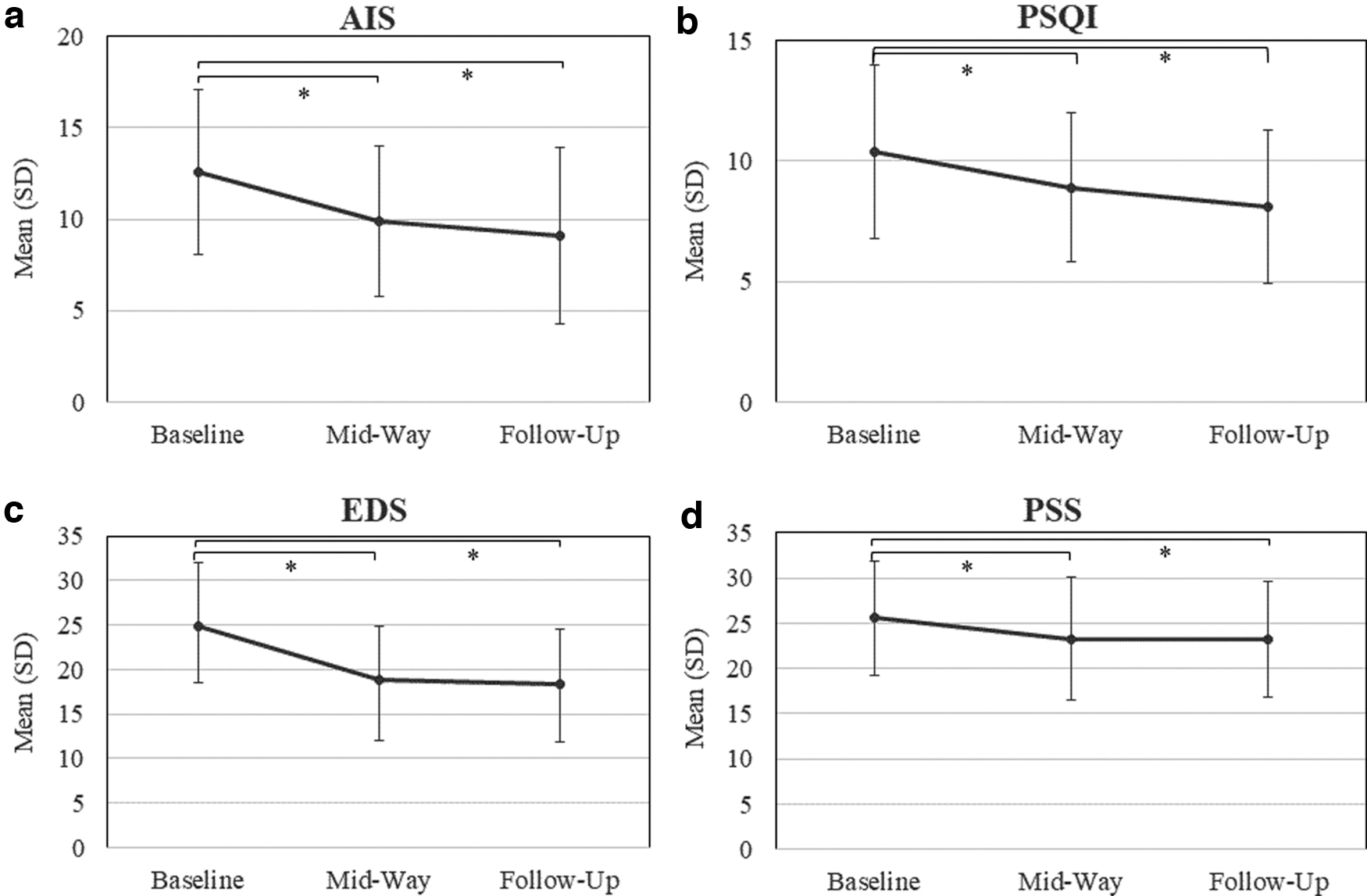
Aim 1. Significant main effects of session: mean (±SD) for sleep measures:
Mean (SD) of scores were as follows: AIS: baseline = 12.6 (4.5), midway = 9.9 (4.1), follow-up = 9.1 (4.8); PSQI: baseline = 10.4 (3.6), midway = 8.9 (3.1), follow-up = 8.1 (3.2); EDS: baseline = 24.8 (7.2), midway = 18.8 (6.0), follow-up = 18.3 (6.3); PSS: baseline = 25.6 (6.3), midway = 23.2 (6.8), follow-up = 23.2 (6.4). The ESS did not show any significant effects. Main effects of group and group by session interactions were not significant for any measure (p's > 0.05).
Aim 2
Linear regression showed significant associations between sleep and emotional stress at baseline for the AIS and the EDS (R 2 = 0.28; p = 0.03) and PSQI and EDS (R 2 = 0.45; p = 0.005) with higher scores on the EDS associated with higher scores on the AIS and PSQI. There was a trend for an association between PSQI and EDS scores at midway (R 2 = 0.24; p = 0.05). No significant associations were found for the PSS with the AIS and PSQI.
Limitations
The limitation of the study is the small sample size: data collection and subject recruitment were suspended with the onset of COVID-19. Thus, there is not enough power to meaningfully address differences between the NADA and sham groups and their interactions with treatment sessions. Thus, it is unclear whether the improvements were due to the NADA auriculo-acupuncture points specifically, placebo effect to inserting needles on any point in the ear, or the body's healing response to needle insertion.
Discussion
Results of the study showed significant improvements in sleep and emotional stress after four auriculo-acupuncture sessions that persisted throughout. There was some association between improvement in sleep and less emotional stress; the direction of the association cannot be determined from these analyses but supports the hypothesis that a reduction in emotional stress could be associated with better sleep.
These results are preliminary, but suggest avenues of future research on the mechanisms of action of how auriculo-acupuncture might impact sleep and emotional stress and how it might best be integrated into community care. Other integrative approaches might be examined as well. Future directions may investigate the mechanisms of the effect of auriculo-acupuncture on sleep and emotional stress (e.g., with salivary cortisol measures) or with additional control measures, specifically utilizing another control without needle insertion (e.g., sitting quietly in a room with music) to better address issues of the placebo effect.
Conclusion
Auriculo-acupuncture may be a low-cost, relatively fast-acting, nonpharmacologic treatment option for improving sleep and emotional stress in Hispanic immigrants as well as other communities. This preliminary study suggests (1) implementation of auriculo-acupuncture treatment could directly benefit sleep and emotional health and (2) it is an avenue for future research in Hispanic immigrants as well as other persons suffering from sleep disturbance associated with emotional stress.
Footnotes
Acknowledgments
The author thanks the American Academy of Sleep Medicine (AASM) for its Humanitarian Award funding to support this research. The author specially thanks the Chesapeake Multi-Cultural Resource Center (ChesMRC) in Easton, MD, for its support and help with recruitment and outreach and with much gratitude to the study volunteers.
Author's Contributions
T.L.R. contributed to all phases of the study including conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, visualization, and writing.
Disclaimer
The opinions and assertions expressed herein are those of the author and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences, the Department of Defense, or the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval Statement
This study was approved by Solutions IRB (approval no. #2019/01/16).
Patient Consent Statement
All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was made possible with thanks to the American Academy of Sleep Medicine (AASM) Humanitarian Award#: 197-FP-18.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.