
Abstract
Objective:
This systematic review aims to assess the impact of music therapy and musical interventions on neuropsychiatric outcomes among patients with moderate and severe mental disorders, in comparison with conventional treatment in isolation.
Methods:
The review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A comprehensive search was conducted on November 16, 2021, using the following databases and search interfaces: Cumulative Index to Nursing and Allied Health Literature, Embase, SCOPUS, Web of Science; PubMed, PsycINFO, Literatura Latino-Americana e do Caribe em Ciências da Saúde, and Scientific Electronic Library Online. Two authors independently assessed the studies for inclusion criteria, extracted the data, and evaluated the quality of the included studies using critical appraisal tools.
Results:
In total, 17 studies were included, 9 of which were randomized controlled trials. The experimental studies involved 5,082 adult and elderly patients. The most prevalent symptoms assessed in the studies were anxiety, depression, and positive and negative symptoms of psychotic disorders. Music interventions were predominantly conducted by music therapists and nurses, providing passive interventions with the selection of musical repertoire by therapists and patients. The frequency with which musical interventions occurred varied greatly in terms of session duration, number of times per week, and number of times during the day. The identified study designs included clinical and quasi-experimental studies. In terms of methodological quality, clinical studies showed weaknesses regarding deviations from intended interventions.
Conclusion:
The effectiveness of music therapy and musical interventions for neuropsychiatric symptoms in patients with moderate and severe mental disorders was evident in quasi-experimental and clinical studies with satisfactory methodological quality. Musical interventions, in various forms of application, represent an interdisciplinary therapeutic tool that complements and enhances conventional treatment. Unlike conventional treatments, the immersive and integrative nature of music interventions allows access to both intrapersonal and interpersonal dimensions during periods of psychic suffering. These findings highlight the importance of researchers addressing methodological limitations, such as deviations from intended interventions, and advocate for the expansion the use of music in community treatment settings.
Introduction
The treatment of individuals with mental disorders has witnessed substantial transformations throughout history, reflecting the prevailing historical and cultural dynamics of each era. These shifts in approach have been characterized by the predominant paradigms of medicalization and institutionalization, primarily focused on correction and therapeutic intervention. 1,2 It has become imperative to dismantle the notion that the etiology of mental illness must be confronted. Instead, it should be comprehended as a unique manifestation and expression of an individual’s suffering. 2
In the context of expanding mental health care practices, various tools can be employed. Music, for example, has been utilized in psychiatric hospitals for some time to alleviate stress, reestablish interpersonal relationships, and promote self-esteem. Music creates an intimate bridge between the realms of philosophy and psychology, offering the opportunity to harmonize art and science. It possesses the potential to facilitate expression and communication between individuals and is often considered to predate language itself. 3
The utilization of music can take two primary forms: music therapy and musical intervention. Music therapy is conducted by a certified music therapist who works one-on-one with individuals to enhance their well-being through structured musical experiences. This aims to foster an improved quality of life, prevent health issues, and support rehabilitation. 3,4 Music therapy employs specific methodologies and principles to achieve therapeutic objectives that encompass both biomedical and socio-community approaches. 5 On the contrary, musical intervention involves the application of music as a therapeutic resource for individuals with various medical conditions. This is typically carried out by health care professionals who are not certified music therapists. The primary goal of musical intervention is to facilitate the patient–professional relationship and enhance the overall approach to patient care. 6
There is a growing commitment to conducting scientific research on the use of music as a complementary approach in mental health care. 3 It’s worth noting that moderate and severe mental disorders exhibit varying prevalence rates worldwide, ranging from 10.9% in Africa to 15.6% in the Americas. Notably, conditions like schizophrenia affect approximately 1 in every 200 adults. 7 Dementia-related conditions, including Alzheimer’s disease, account for 60%–80% of cases, with vascular dementia representing the remaining 20%. 8
In this context, the utilization of music assumes a pivotal role in promoting well-being. It accomplishes this by eliciting positive emotions, enhancing self-awareness, and allowing individuals to express their feelings and thoughts. Music also helps in reducing the sense of alienation, making self-identification more attainable for individuals who might have previously felt like outsiders. 4,5 In contrast to conventional treatment, which predominantly relies on psychotropic medications, music therapy offers a comprehensive and holistic approach to care. It facilitates the patient’s integration into the realm of mental health, addressing not only individual aspects encompassing physical, mental, and spiritual well-being but also broader social factors, including family dynamics, cultural influences, work-related issues, and historical context. 4
Hence, the primary objective of this study is to assess the impact of music therapy and musical interventions on neuropsychiatric outcomes among patients with moderate and severe mental disorders, in comparison with conventional treatment in isolation. By doing so, our aim is to furnish empirical evidence that advocates for the incorporation of music within a more comprehensive and holistic approach to care.
Methods
Study design
This systematic review was conducted following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (the checklist is present in Supplementary Material). The review is registered on the PROSPERO platform and can be identified by the ID CRD42022307603. 9
To conduct the review, the PICOS strategy will be followed according to the following points: Population (P): individuals with moderate and severe mental disorders; Intervention or exposure (I): music therapy; Comparison or control (C): treatment with psychopharmacology; Outcomes or outcome measures (O): anxiety, depression, aggressive behavior, hallucinations, and delusions; Study design (S): intervention (quasi-experimental and experimental). The research question for this review (PICOS) is: What is the effectiveness of music therapy for outcomes of anxiety, depression, aggressive behavior, sleep, hallucinations, and delusions in individuals with moderate and severe mental disorders compared with the treatment with psychopharmacology?
Search strategy
Searches were conducted on November 16, 2021, in the information resources Cumulative Index to Nursing and Allied Health Literature, Embase, SCOPUS, Web of Science; PubMed, PsycINFO, Scientific Health Information from Latin America and the Caribbean countries, and Scientific Electronic Library Online.
Based on the research question, descriptors (based on Health Sciences Descriptors), Mesh terms (based on the National Center for Biomedical Information), Emtree terms (Embase thesaurus), keywords, and free terms that could compose the search strategies for the respective information sources were identified. The search strategies employed were developed with the assistance of a librarian who is part of the research team and are presented in Supplementary Appendix.
Studies selection
The inclusion criteria for the retrieved documents from the information resources were considered as follows: (1) experimental studies (quasi-experimental or randomized control trial [RCT]), (2) published between 2011 and 2021, (3) in English, Spanish, or Portuguese languages, (4) addressing psychological outcomes. As exclusion criteria, the following were considered: (1) review articles, (2) articles that do not address the research question, and (3) articles that do not cover the selected topic.
The search results were organized using the reference manager EndNote, and duplicate articles were excluded. The Rayyan software was used for study selection. Two independent researchers participated in this stage (blinded), and in case of disagreement, a third researcher was consulted for the decision to include or exclude the article. 10
The selection of studies initially involved reading titles and abstracts, applying the eligibility criteria to refine the sample by including those who meet the review’s objective. Subsequently, the studies were read in full to verify compliance with the selection criteria.
Data extraction and sensitivity analysis
After the selection of retrieved articles was completed, we conducted an in-depth review to underpin our understanding of the studied phenomenon. To systematically organize and synthesize the gathered data, an Excel spreadsheet was employed. This spreadsheet included bibliographic details, methodological specifics (study type, location, care context, study population, outcome measurement instruments, and recorded results), as well as the study findings. 11
Furthermore, we assessed the quality, functionality, and structure of musical interventions in accordance with the Reporting Guidelines for Music-Based Interventions. These guidelines encompass seven components that delineate how music-based interventions function: Intervention Theory, Intervention Content, Intervention Delivery Schedule, Interventionist, Treatment Fidelity, Setting, and Unit of Delivery. These recommendations aim to support the Consolidated Standards for Reporting Trials and Transparent Reporting of Evaluations with Non-randomized Designs statements for transparent reporting of interventions, addressing the variety, complexity, and uniqueness of the interventions. 12 The delineation of the components followed the framework that is presented in Table 1.
Reporting Guidelines for Music-Based Interventions 12
The risk of bias for each study was assessed by two independent examiners using the Cochrane Collaboration tool. This scale categorizes studies as having a low risk, an uncertain risk, or a high risk of bias, with assessments based on six specific criteria: random sequence generation, allocation concealment, blinding (patients, personnel, and outcome assessors), incomplete outcome data, selective reporting, and other sources of bias. 13
Results
After screening, 31 full text articles were reviewed to analyze if they met the inclusion criteria. Of these, 14 articles were excluded; thus, a total of 17 studies met the inclusion criteria for the review. Figure 1 provides a detailed outline of the article selection process.
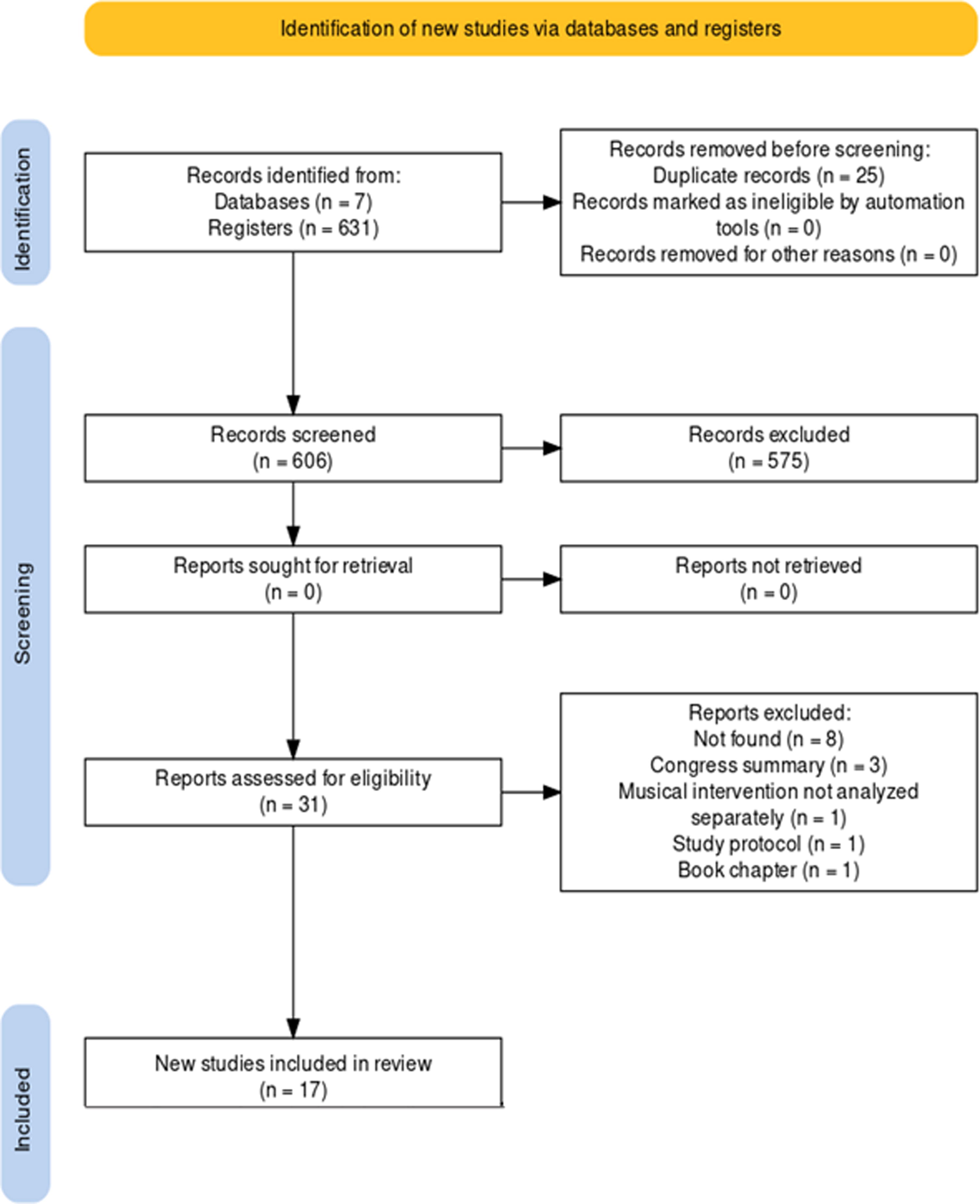
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram for the systematic review. BVS, Virtual Health Library (Biblioteca Virtual em Saúde); CINAHL, Cumulative Index to Nursing and Allied Health Literature; WOS, Web of Science.
Table 2 provides a summary of the sample size, clinical conditions, mental health assessment scales, primary findings, and the level of evidence for the 17 studies.
Summary of the Characteristics and Results of the Included Studies (n = 17)
The findings of this study demonstrate that music therapy and musical interventions are valuable complements to the existing mental health care practices. 14 –30 They serve as potent interdisciplinary care technologies, leveraging the language and capabilities of music to transcend psychological barriers and fostering the restoration and enhancement of mental health through collaborative engagement between professionals and service users. 15
The study identified a more pronounced clinical improvement, particularly in symptoms such as anxiety, 15,20,27,30 agitation, 18,26,27 and depression. 14,19,26,27,30 There was a substantial reduction in the use of psychotropic medications, as indicated by several studies, 18,27,28 including a decrease in the utilization of benzodiazepines. 28
The application of various forms of musical interventions was observed to be feasible and straightforward for the engagement of participants. This approach was also well received by professionals and staff in nursing homes, 16,17,20,27,28,30 psychiatric inpatient units, 14,15,18,21 detoxification units, 22 –24 and other health care facilities. 19,25 –29
The studies did not identify challenges regarding the application of musical interventions and music therapy. Conversely, caregivers and health care professionals found that the intervention was easy to implement. 18 It not only improved caregiver burden 17,20 but also reduced the average length of stay and the number of hospitalizations events. 18
The results of research studies specifically utilizing music therapy have demonstrated that it allows for the expression of emotions; 19 reduction of symptoms of anxiety, 20,30 depression, 30 and delirium; 30 improvement in readiness and motivation for treatment; 23,24 and being the most effective nonpharmacologic intervention. 20 Musical interventions have achieved convergent results by reducing negative symptoms, 14,21 anxiety, 15 agitation, 26 and depressive 14,26 and manic symptoms 14 and promoting better patient engagement in care practices. 16
Research specifically focused on music therapy revealed that it enables the expression of emotions; 19 reduces symptoms of anxiety, 20,30 depression, 30 and delirium; 30 enhances readiness and motivation for treatment; 23,24 and stands out as the most effective nonpharmacologic intervention. 20 Musical interventions also consistently produced positive outcomes, including the reduction of negative symptoms, 14,21 anxiety, 15 agitation, 26 and depressive 14,26 and manic symptoms, 14 and an improved level of patient engagement in care practices. 16
Out of the 17 articles included in the study, 6 of them did not cover all the categories outlined in the Reporting Guidelines for Music-Based Interventions. These omitted categories were Intervention Content, particularly the elements related to Intervention Materials, 20,22,25,29 Person Selecting the Music, 25,29 Music, 25,28 Music Delivery Method (live or recorded); 28 Intervenor, 20 and Intervention Delivery Schedule. 27 Table 3 provides a descriptive overview of the components of the musical interventions identified in the studies.
Detailed Characterization of Music Therapy Interventions (n = 17)
When considering these categories, it becomes evident how each item significantly impacts the quality and the potential for replication of the musical interventions detailed in each study. This is illustrated in Table 4, which emphasizes the categories that are covered in the articles. 12
Components of Interventions Reported Between Studies (n = 17)
Subtitle: A, Intervention Theory; B, Intervention Content; C, Delivery Schedule; D, Interventionist; E, Treatment Fidelity; F, Setting; G, Unit of Delivery.
After an analysis of the methodological procedures in the articles, two primary study designs were identified: RCTs (level of evidence 1b) 14,15,17,19,20,23 –26,30 and pre-post studies conducted without a control group (2c). 16,18,21,22,28,29 Among the nine RCTs, 14,15,17,19,20,23 –26,30 seven were categorized as having a low risk of bias. The second domain, which pertains to the potential bias arising from deviations in the intended interventions, raised some concerns across the studies, particularly related to the blinding of those responsible for delivering the musical interventions. The details of the quality assessment for the articles included in this systematic review are provided in Figure 2.

Cochrane risk of bias assessment for randomized controlled trials. Domain 1 (D1), Bias arising from the randomization process; Domain 2 (D2), Bias due to deviations from intended intervention; Domain 3 (D3), Bias due to missing outcome data; Domain 4 (D4), Bias in measurement of the outcome; Domain 5 (D5), Bias in selection of the reported result.
In the six before-and-after studies without a control group, 16,18,21,22,28,29 there is a risk of selection bias, which occurs when participants, follow-up time, or developmental events are not controlled or randomized. Among these, two studies 16,21 did not employ randomization since the group assignments were determined by the institution’s organization where the participants were placed. In another study, 18 randomization was not utilized because music intervention was only provided to patients who voluntarily requested to participate. Two other studies 22,28 also lacked randomization and control groups. The two remaining studies 27,29 did not include a control group in their design. 31
Discussion
The various positive results identified in this review support the inherent therapeutic potential of utilizing music therapy and musical interventions for dealing with and processing psychological distress. Music provides access to various human dimensions, spanning from somatic processes to psychic experiences, and it creates an integrative and holistic impact. As a therapeutic tool, it has the capacity to activate internal and subjective content, facilitating the (re)interpretation of experiences and enhancing self-confidence, self-image, expression, and creative processes. 32
Indeed, when considering specific scenarios such as patients with negative symptoms of schizophrenia, verbal communication of their emotions and thoughts can be challenging. 33 Nonetheless, music therapy or a musical intervention holds the potential to surmount this obstacle, given that music directly engages with emotional centers, stimulating areas of the brain associated with emotions, resulting in pleasurable sensations. 33,34 It allows the activation of cognitive resources, memory, thinking, and emotion, thereby contributing to the preservation of the individual’s identity. 34
Music therapy and musical interventions are regarded as highly effective tools for enhancing social interaction by nurturing personal and interpersonal communication skills. 16,30 They contribute to improved cognition, 17 quality of life, 17 and overall well-being encompassing physical, psychological, and social aspects. 16,17,30 Moreover, these approaches aid in preserving expressive abilities, 16,29,30 promoting sociability, 16,29,30 and reducing symptoms related to depression, 14,19,26,27,30 anxiety, 15,20,27,30 and stress. 22
The observation revealed that music therapy and musical interventions were predominantly implemented within institutional settings. 14 –18,20 –22,24,25,27 –30 This outcome can likely be attributed to the characteristics of the population under analysis, individuals with moderate-to-severe mental disorders, as hospital services have been the most common platform for this therapeutic approach. 14,15,18,21 –24 In contrast, the utilization of music in community-based contexts leads to shorter hospital stays, 14 implying that the benefits of care are attainable, irrespective of the service type.
This discovery is corroborated by another study that found a decrease in readmission rates for individuals who underwent music therapy intervention in comparison with those who did not. 35 Consequently, it can be affirmed that musical interventions transcend clinical advantages and embody a political mechanism by contributing to the shift away from the asylum model, thereby addressing the issue of the “revolving door” phenomenon. 35,36
The majority of studies in this review employed instruments designed to assess primary outcomes through psychological constructs. 14 –20,23 –30 However, two studies evaluated the outcomes of musical interventions using biological parameters, specifically, the measurement of cortisol levels. 21,22 It is contended that the incorporation of biologic parameters contributes to the generation of clinical evidence concerning the use of music among the population under investigation. Biomarkers, such as cortisol, serve as objective and quantifiable indicators, with cortisol, in particular, being a recognized stress marker. 37 –39
Regarding the entity responsible for selecting the music, there was a division between patients themselves, based on their expressed preferences (not necessarily involving specific song choices) 16,26,27,30 and the interventionists. 17,21,23,24 In a study that conducted a meta-analysis, it was discovered that the outcomes of musical interventions were more favorable when the musical selection was predetermined as opposed to music chosen by either the music therapist or the patient. Furthermore, relaxation music had a more beneficial effect compared with favorite music and classical music. 38 Conversely, interventions in which music was presented passively to subjects with dementia yielded more positive results than other, more interactive, or lengthier interventions. 40
This study makes a valuable contribution by highlighting the advantages of using music as an approach for patients with severe mental disorders and dementia. Beyond the clinical benefits in symptom management, it enhances the quality of life, fosters social integration, and strengthens the relationships between health care professionals and their patients. In addition, it presents an intervention that is easy to implement and cost-effective and challenges prevailing paradigms.
Limitations of the study
One of the limitations of this study pertains to the lack of clear and detailed descriptions of musical interventions in some of the articles analyzed. This limitation is substantial because detailed descriptions are crucial for improving, replicating, and translating music-based interventions into clinical practice. Moreover, the wide variety of approaches and techniques among these interventions created heterogeneity that made it challenging to generalize the conclusions. As a result of this heterogeneity, the study did not conduct a meta-analysis.
Conclusions
Through evidence of levels 1b and 2c, it was identified that music therapy and musical interventions demonstrate effectiveness in the care of individuals with severe and moderate mental disorders in various care contexts. It leads to improvements in symptoms, such as reducing depressive, dissociative, delusional, anxiety, agitation, aggression, and pain symptoms.
The application of music therapy and musical interventions enhanced the relational dimension of the investigated population, reflected in improvements in socioemotional functioning, emotional well-being, and personal development. Among the studies analyzed, there were reports of strengthened affect, quality of life, increased participation in care and activities, and enhanced social interaction and inhibition.
Music therapy and musical interventions are a complementary therapy that favors the reversal of the biomedical model, as evidenced by the reduction in the administration of medications for agitation, the use of anxiolytics, antidepressants, and psychotropic drugs, as well as a decrease in the concomitant use of specific medications, whose potential harms outweigh the clinical benefits, such as the concurrent use of antipsychotics and antidepressants. In addition, it led to a reduction in hospitalization time, promoted motivation and engagement in treatment, and consequently alleviated caregiver burden.
The interventions analyzed in this review were described in detail, which facilitates their application in real-world settings. The majority of instruments were based on psychological constructs, and variability represented a limitation. It is suggested that the use of biomarkers could enhance comparisons with other therapeutic approaches, and further studies should investigate these benefits in community-based and territorial services.
In music lies the potential to be a rehabilitative source beyond an auditory experience, unfolding as a transdisciplinary tool capable of fully encompassing the health of the individual, expressed in their body, heart, and mind.
Footnotes
Authors’ Contributions
E.G.C., L.C.D.S., M.S.D.C.O., G.C.B., M.B., and T.S.D. were responsible for conceptualization, methodology, validation, and visualization. E.G.C., L.C.D.S., M.B., and T.S.D. were responsible for formal analysis, investigation, resources, and writing—original draft. E.G.C., L.C.D.S., G.C.B., and T.S.D. were responsible for writing—reviewing and editing. M.S.D.C.O. and T.S.D. were responsible for supervision and project administration.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix
Supplementary PRISMA_2020_checklist
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.