
Abstract
Background and purpose:
Little is known about the applicability, utilization, and effectiveness of mind–body interventions (MBIs) for conditions that are not predominantly pain, neoplastic, or psychiatric, particularly in pediatric patients. This scoping review describes research pertaining to such interventions in youth with nonpain, noncancer, and nonpsychiatric predominant chronic medical conditions.
Methods:
Searches of EBSCO CINAHL, Elsevier Scopus, Ovid for MEDLINE, and Ovid PsycInfo were conducted to investigate MBIs in youth under 18 years of age with nonpain, noncancer, and nonpsychiatric predominant chronic medical conditions. Articles published between 2010 and 2020 were included. Abstracts were screened by three authors for inclusion, and disagreements were resolved by a designated author. Selected full-text articles were divided among all authors for review of study quality, intervention feasibility and acceptability, and effectiveness.
Results:
The search yielded 1010 titles with 15 meeting the final inclusion criteria, studying a total of 641 youth. Participants ranged in age from 6 to 19 years (included studies had data on participants <18 years reported separately); 61.5% were female (n = 394) and 38.5% were male (n = 247). The two most common conditions studied were asthma and irritable bowel syndrome, with yoga being the most popular intervention. Overall, MBIs showed promising preliminary evidence for improving symptoms and quality of life in youth with chronic medical conditions.
Conclusion:
MBIs have been successfully delivered and show promise in symptom palliation and quality of life improvement for youth with a variety of chronic medical conditions. More data from high-quality randomized controlled trials are needed to further characterize the effectiveness of specific modalities for specific conditions.
Introduction
Nearly one in four children in the United States are affected by chronic and often lifelong medical conditions. 1,2 Children with chronic conditions often require repeated hospitalizations, home health care, and rehabilitation. 3,4 The most common chronic conditions in children include asthma, epilepsy, and diabetes, leading to estimated additional medical expenses of $1,378 to $9,059 per child annually. 5 This translates to ∼$25 to $167 billion in additional health care costs for these conditions alone. 6
Children often feel and are out of control of their circumstances, which may thereby worsen their burden of stress and lead to behavioral problems and emotional dysregulation. 7,8 Care for children with chronic conditions has generally focused upon treating the presenting medical concern, with limited resources available to address the additional allostatic load imposed by these chronic medical conditions on other parts of their lives. 9
Mind–body interventions (MBIs) present an innovative, accessible, and effective means to improve coping in chronic health conditions. 10 In the 2007–2012 National Health Interview Survey, MBIs were ranked among the top 10 complementary and integrative health (CIH) practices utilized by both adults and children. 11 MBIs demonstrate compelling benefit for psychiatric conditions, such as post-traumatic stress disorder, 12 and are increasingly being utilized for pain conditions as well as quality of life improvement in various cancers. 13,14 Innovations in delivering MBIs remotely, through telehealth or electronic smartphone-based applications, or in group settings are also promising. 15 Many seekers of CIH turned to virtual care during the coronavirus disease 2019 pandemic. 16
While the impact of MBIs is extensively described in the literature for all ages—predominantly adults—in the management of pain, cancer, and psychiatric conditions, less is known about their applicability, utilization, and effectiveness for other chronic medical conditions, particularly in pediatric patients. 17 –20 Thus, the objective of this scoping review was to describe the literature addressing MBIs delivered to pediatric patients with chronic, nonpain, and nonpsychiatric predominant medical conditions with regard to feasibility, acceptability, and effectiveness.
Methods
Ethics approval was not required for this scoping review, and a review protocol does not exist for this study.
Eligibility criteria and information source
This review was conducted in accordance with the Preferred Reported Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines extension for scoping reviews. 21 The inclusion criteria for this review were as follows: (1) articles were published between September 1, 2010 and September 30, 2020, and were designed as prospective cohort trials, randomized controlled trials (RCTs), mixed-methods studies, waitlist-control trials, case series, or clinical replication series; (2) included data for youth under 18 years of age with chronic, nonpain, noncancer, and nonpsychiatric predominant medical conditions, broadly defined as any medical diagnosis affecting children and requiring long-term management with a health care provider; and (3) utilized MBIs including, but not limited to, biofeedback, guided imagery, hypnosis, meditation, Tai Chi, and yoga.
Owing to the extensive variation in definitions of “chronic conditions” across professional societies and medical bodies, 22 the term was left intentionally broad to include how it was defined in each article obtained during literature search. Concussion was included as a chronic condition because, although acute in onset, subsequent symptoms often require prolonged management; exact search terms for chronic conditions are enumerated in Appendix A1.
The criteria for exclusion from this review included studies that (1) included children older than or equal to 18 years of age or did not report data for those under the age of 18 years separately; (2) investigated nutrition, exercise, or psychotherapy-based interventions; (3) MBIs that consisted of acupuncture interventions (as the body of literature exploring acupuncture is large and already established); (4) included pain as the primary outcome measure; and/or (5) were review articles or editorials.
A search strategy was generated for the concepts of MBIs in pediatric patients with chronic illnesses. Both controlled vocabulary and title and abstract fields were used for the search terminology. Searches of EBSCO CINAHL, Elsevier Scopus, Ovid for MEDLINE, and Ovid PsycInfo were conducted, and search results were articles limited to the English language and published between the dates of September 1, 2010 and September 30, 2020. Reviews, editorials, and commentary were removed before exporting results to a Covidence database for review.
Covidence is a web-based collaboration software platform that streamlines the production of systematic and other literature reviews. 23 The search was conducted by a single author (M.N.). Three authors (M.M., D.W.M., and M.E.C.) screened and reviewed the title, abstract, and full text of each retrieved article. Any disagreements were resolved by one author (M.M.). Appendix A1 provides a detailed description of the search strategy. While the initial search strategy included acupuncture, articles with acupuncture interventions were excluded during screening by authors.
Data extraction and analysis
The Covidence database was utilized for data collection from generating the search strategy, initial abstract and full-text review, and initial data collection. The following components were used to adequately extract data from the included studies: study type; number, age, and demographics of participants; chronic medical condition studied; intervention type and setting; measures of MBI feasibility and acceptability; outcome measurement instruments; and outcomes following MBI. Data were extracted and further analyzed by two authors (R.S. and D.W.M.) using an Excel spreadsheet.
Study quality assessment
Study quality was assessed using a modified Newcastle-Ottawa Quality Assessment Scale 24 for all included articles. Scale Four categories were included: (1) representativeness of the sample; (2) comparability of intervention and control groups; (3) assessment of outcomes; and (4) statistical tests used.
Results
Article selection
A total of 1010 articles were screened after 264 duplicate studies were removed. Of these, 112 articles were selected for full-text review, and 898 articles were excluded (Fig. 1). Studies were excluded on the basis of the aforementioned exclusion criteria. Fifteen publications met the final inclusion criteria. 25 –39 All 15 included studies were published between 2010 and 2019.
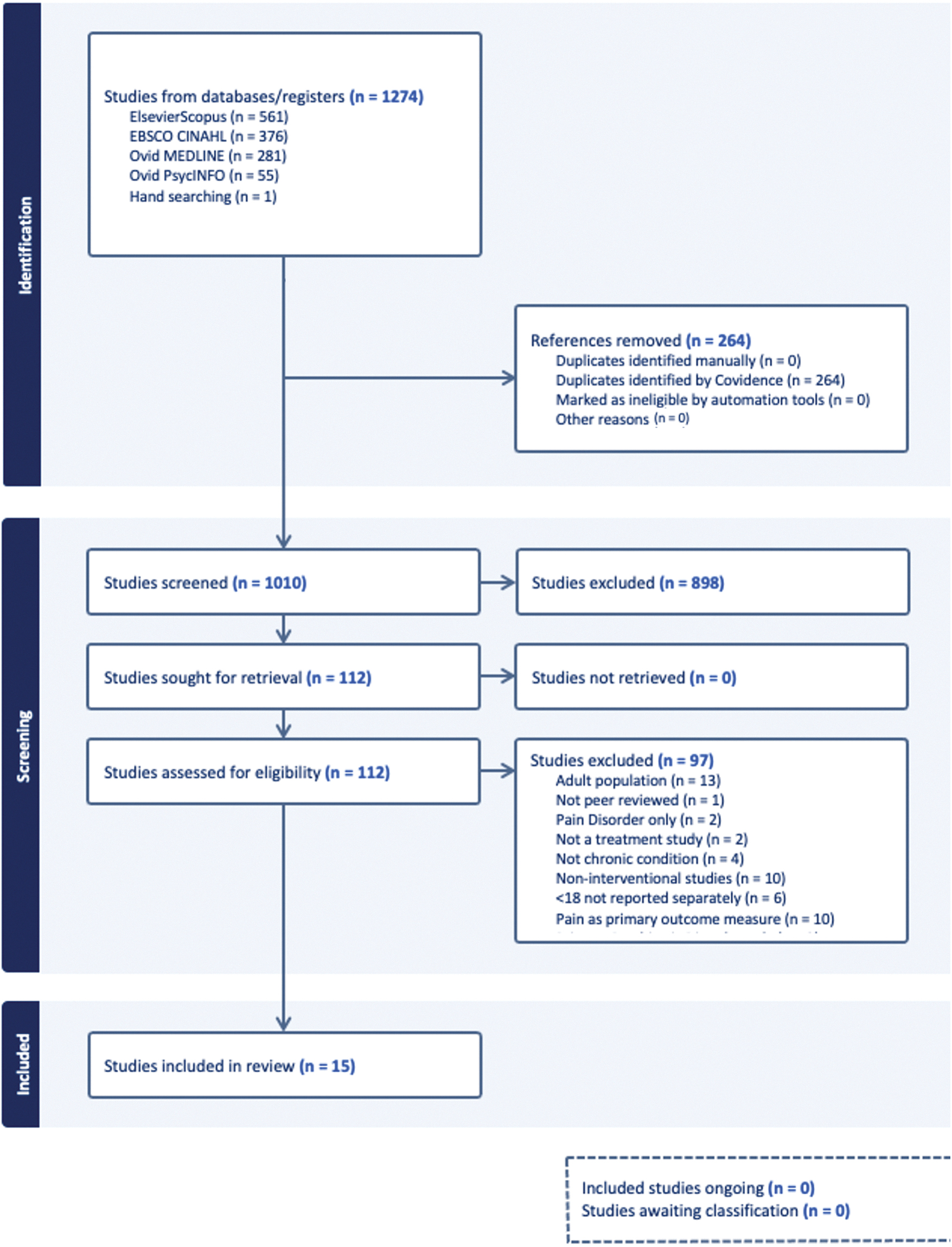
Preferred Reported Items for Systematic Reviews and Meta-Analyses flow diagram.
Study types
Studies' target conditions, population, intervention details, setting, measures, design, presence/absence of a control group, and presence/absence of a home practice component are presented in Table 1. Most of the included studies were prospective cohort trials (n = 6, 40%), followed by RCTs (n = 3, 20%), mixed-methods studies (n = 2, 13%), and one each of waitlist-control, multiple baselines, case series, and clinical replication series. Pilot studies constituted 40% (n = 6) of the included studies, and 47% of the included studies had a control group (n = 7).
Study Characteristics
Results analyzed separately for adolescents; subgroup mean age not provided
BAM, breathing and awareness meditation; BP, blood pressure; DS, digital storytelling; FAP, functional abdominal pain; GI, guided imagery; HE, health education; HEC, health education control; HRVB, heart rate variability biofeedback; HTN, hypertension, IBS, irritable bowel syndrome; LST, life skills training; MBI, mind-body intervention; MBY, mindfulness-based yoga; N/A, not applicable.
Population
Demographic details of participants and studies, including study location, number of participants, mean ages, gender, and race, are presented in Table 2. There were a total of 641 participants (394 female and 247 male) across the 15 included studies, with an overall mean sample size of 43 participants, ranging from a case series with 3 participants 39 to as many as 162 participants 27 ; the latter was an RCT. Ages of study participants ranged from 7.5 to 19 years; however, in included studies with participants above 18 years of age, data for individuals under 18 years of age were reported separately and examined in this review. Notably, female participants predominated in all studies, constituting an average of 61.5%.
Participant Demographics Within Included Studies
Study locations—country of origin, study setting
Most studies took place in various cities throughout the United States (n = 10, 67%); of the remaining five studies, one each (6.7%) was conducted in Canada, China, Iran, Taiwan, and Turkey, respectively. A map indicating the locations of the 15 included studies is shown in Figure 2.

Geographic location of included studies.
Chronic medical conditions
Asthma was studied in three articles (20%), which utilized MBIs including yoga, Tai Chi, and guided imagery; irritable bowel syndrome (IBS) or other gastrointestinal disorders were also studied in three articles (20%). Hypertension or elevated blood pressure was explored in two studies (13%), as was cystic fibrosis (13%). The full array of chronic medical conditions studied in this scoping review is illustrated in Figure 3.
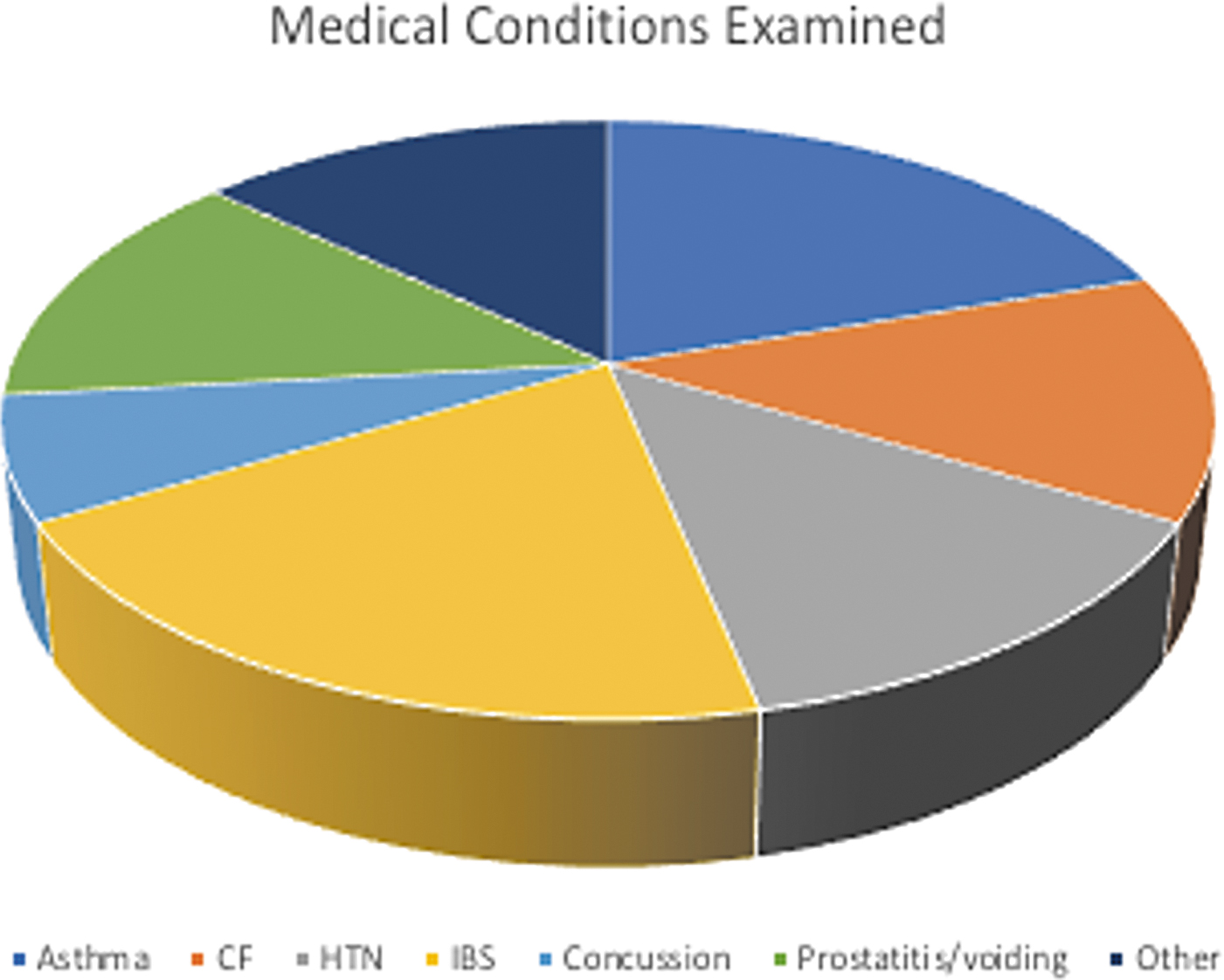
Chronic medical conditions.
Interventions
Types of MBIs
The included studies assayed many different types of therapeutic interventions. Of the 15 included studies, five utilized some form of yoga as the primary intervention, four employed biofeedback, three employed breathing and awareness meditation (BAM), two used guided imagery (including “relaxation and guided imagery”), and one focused on Tai Chi.
MBIs were investigated for the following conditions: yoga for asthma, concussion, cystic fibrosis, and IBS (two studies). Biofeedback was utilized for children with cystic fibrosis, DES, IBS, and chronic prostatitis (CP). Guided imagery was used in cohorts of participants diagnosed with obesity, as well as asthma with associated anxiety disorders. BAM was delivered to a group of youth at risk of hypertension (HTN), and Tai Chi was used in youth with asthma.
Interventions also varied by the settings in which they were delivered. Four studies were conducted in the school setting, where they were integrated into the school day; 10 took place in community or clinical research settings, and one, Chadi et al., had partial virtual delivery. 38 Only one study, Bingham et al., was delivered exclusively in an inpatient setting. 31
Group versus solo
Most MBIs (60%) were delivered in a group setting. Six studies described MBIs that were delivered one-on-one to participants: all four biofeedback studies were delivered one-on-one, as was a case series of guided imagery for asthma and anxiety, and a trial of yoga for cystic fibrosis.
Home practice
Home practice was a required element of the intervention in six (40%) of the included studies; home practice was encouraged, but not required, in four (27%) of the included studies. The remaining five studies (33%) did not include a home practice element.
Outcomes
Studies' main outcomes are presented in Table 3. Participants generally demonstrated improvements in self-reported medical symptoms and objective measurements after MBIs. The heterogeneous nature of the data from these 15 studies meant that calculations such as meta-analysis would yield results of limited practical utility and are outside the scope of this scoping review. 40 Therefore, this section summarizes studies by condition and intervention type as one means of collating results for better conceptualization and comparison.
Outcome Measures and Key Results of Included Studies
ABP, ambulatory blood pressure; ACMI, adolescent version of the Cook-Medley Hostility Inventory; APSA, Additional Pain Symptoms Assessment; BSI-18, Brief Symptom Inventory-18; CSI, Children's Somatization Inventory; DVSS, Dysfunctional Voiding Symptom Score; EMG, electromyography; ET-1 SNP, endothelin-1 single nucleotide polymorphism; FACIT-Fatigue, Functional Assessment of Chronic Illness Therapy Fatigue Subscale; FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; HRV, heart rate variability; MSAS, Memorial Symptom Assessment Scale; NIH-CPSI, National Institute of Health Chronic Pain Symptom Index; NRS, abdominal pain numeric rating scale; PAQLQ, Pediatric Asthma Quality of Life Questionnaire; PEFR, peak expiratory flow rate; STAIC, State-Trait Anxiety Inventory for Children; UTI, urinary tract infection.
Asthma
A case series of youth with asthma and anxiety suggested that engaging in a relaxation/guided imagery intervention yielded improvements in lung function and anxiety. 39 In youth with asthma alone, a Tai Chi intervention was associated with improvements in lung function and quality of life as compared with nonasthmatics 30 ; yoga training yielded improvements in lung function in youth with exercise-induced asthma. Interestingly, after the yoga intervention, youth with exercise-induced asthma subsequently became exercise-tolerant. 29
Other chronic health conditions
A single mixed-methods study assessed the impact of an adapted 8-week MBI delivered either virtually or in person in a group of youth with various chronic health conditions. 38 No untreated control group was used for comparison. Results showed a statistically significant decrease in depressive symptoms and positive impacts on well-being, stress, pain, and sleep in both groups, whereas no significant differences were observed in salivary cortisol levels in either group.
Concussion
A small pilot study of mindfulness-based yoga training for youth with concussive symptoms (n = 6) demonstrated increased heart rate variability (a measure of healthy neurophysiological function), decreased concussive symptomatology, and ability to engage in strenuous exercise both immediately and 3 months postintervention compared with baseline. 25 No control group was included.
Cystic fibrosis
For hospitalized youth with cystic fibrosis (n = 12), a video-based biofeedback intervention yielded improvements in eye-breath coordination (i.e., eye tracking of a moving target that represented the breath) as compared with baseline. 31 In another study, youth who engaged in a 10-week yoga intervention demonstrated significant improvements in anxiety, depression, and joint pain immediately postintervention. 33 These changes were not sustained at follow-up. Neither study included a control group for comparison.
Dysfunction elimination syndrome
Among youth with dysfunction elimination syndrome (n = 80), those who received an intervention consisting of animated biofeedback therapy alongside behavioral modification and pelvic floor exercises demonstrated significant improvements in subjective and objective voiding problems (including daytime wetting, fecal soiling, staccato voiding, and urinary tract infection) compared with those who received behavioral modification and pelvic floor exercise education alone. 32
Hypertension
Two studies employed BAM versus life skills training (LST) interventions for Black youth at risk of hypertension. 27,37 Gregoski et al. categorized participants using endothelin genotyping and quantified allostatic stress by measuring discrimination-based stress exposure. Both BAM and LST interventions were effective in reducing ambulatory blood pressure, although the BAM group displayed effects faster; however, in Gregoski et al., only BAM reduced blood pressure in gene noncarriers with high stress exposure.
In addition, Wright et al. found significant decreases in systolic blood pressure and hostility after BAM intervention, as measured by the Cook–Medley Hostility Inventory. Notably, there were significant increases in hostility post-LST.
IBS
For youth with IBS, the results of two Iyengar yoga interventions were correlated with significant improvements in symptoms, sleep, and pain as compared with controls 35,36 ; one study also reported significantly improved psychological distress and fatigue as compared with control. 35 HRVB led to significant improvements in IBS per patient self-report 34 ; 69.2% of participants achieved full remission, that is, 2 weeks symptom-free, while 30.4% of participants achieved partial remission. Similar improvements were observed in the same study for children with functional abdominal pain (FAP); controls were not included in this study.
Metabolic syndrome
One study assessed the impact of education on leading a heart-healthy lifestyle plus either guided imagery or digital storytelling in a cohort of Latino youth with obesity Latino children. 26 Both interventions were deemed acceptable to the study population. Guided imagery yielded increased physical activity alongside improvements in intuitive eating (described as a nondieting philosophy emphasizing permission to eat, relying on internal satiety cues, and engaging in physical activity for well-being) and salivary cortisol; these changes were not observed in the digital storytelling group.
Chronic prostatitis
Among pubertal patients with CP, those who received biofeedback training for 24 or more months after a 12-week intensive training experienced significant improvements in CP symptoms. 28 In comparison, those who received follow-up biofeedback training for less than 24 months postintensive training, paradoxically, experienced significant increases in CP symptoms and pain and decreased maximum urinary flow rate.
Instruments
Outcome measurement tools examined in this review were highly heterogeneous, owing to the variety of intervention types delivered and medical conditions treated. Details of the outcome measurements used in each study can be found in Table 1.
Intervention feasibility and acceptability
Thirteen of the 15 reviewed studies reported some measurement of feasibility and acceptability, including tracking of attendance, home practice (if required or encouraged during intervention), ratings or surveys of program, and/or qualitative interview data pertaining to satisfaction with the intervention; only two studies did not report attendance data. MBIs were overall deemed feasible and acceptable by participants, although one study (Wright et al. 37 ) noted overall loss of 29% of cohort and attendance rate of <70% attributable to school attendance. Details of intervention feasibility and acceptability for each included study can be found in Table 4.
Feasibility and Acceptability Reported in Reviewed Studies
Study quality assessment
The Modified Newcastle-Ottawa Scale (NOS) criteria are described in Table 5. The NOS (Table 6) has a maximum, highest quality score of 8 points. Points were given based on sample representativeness, presence of a matched control group, subjective versus objective outcome measurement, and extent of statistical tests performed. Scores for the included studies ranged from 3 to 7, with a mean score of 4.9, such that higher scores reflected greater methodological quality.
Modified Newcastle-Ottawa Quality Assessment Scale Criteria for Studies of Mind-Body Interventions for Youth with Chronic Medical Conditions
Scoring of Modified Newcastle-Ottawa Quality Assessment Scale for Studies of Mind-Body Interventions for Youth with Chronic Medical Conditions
Discussion
Overview
Based on the search performed, this appears to be the first scoping review of studies analyzing MBIs in youth under 18 years of age with various chronic, nonpain, noncancer, and nonpsychiatric predominant medical conditions. This review highlights encouraging preliminary findings for MBI feasibility, acceptability, and effectiveness, while underscoring the need for significantly more high-quality trials in this underserved population. Specific considerations regarding intervention design (including improved controls), participant needs, strengths, limitations, and future guidance are discussed in sections “Study types” to “Future considerations.”
Study types
The most frequently observed MBIs in this review included yoga, followed by Tai Chi, guided imagery, and digital storytelling, which were most frequently utilized in populations with asthma and IBS. Study heterogeneity made meta-analysis practically impossible, and the wide range of study designs included in this review elucidates the need for further efforts toward determining optimal formats for research and care delivery. Most studies were prospective trials, and only three were RCTs, which had small sample sizes ranging from 35 to 162 participants. More high-quality large-scale RCTs are warranted to better characterize intervention effectiveness for these conditions.
Population
Demographics
This review also elucidates certain trends in participant demographics among YOUTH receiving MBIs for chronic conditions. All (except for the study involving prostatitis) included more females than males, with the lowest proportion of female participants being 52%. No study explicitly explained this distribution, and only one acknowledged this skewed distribution. Possible explanations for this observation may reflect a broader trend of chronic medical conditions affecting more females than males, 41 gender-based differences in symptom reporting or diagnosis, and issues related to adherence, as well as relatively greater female participation in CIH modalities, such as MBIs, overall. 42
Three studies intervened upon specific demographic groups: Gregoski et al. and Wright et al. assessed the impact of BAM upon blood pressure in Black high school students, who are at particular risk of hypertension, 27,37 while Weigensberg et al. explored the impact of guided imagery with health education upon Latino adolescents with obesity, at risk of metabolic syndrome. 26 These studies represent critically important endeavors for numerous reasons.
First, delivering MBIs to youth at high risk for specific chronic medical conditions should represent a priority within the CIH space. Concurrently, efforts to engage with demographic groups who have historically been less represented among patients receiving CIH reflects an important move toward equitable access to potentially high-value, low-cost, and preventative health care, especially in youth.
Developmental stages
Participants had a wide range of ages. This is important in studies in the pediatric population, as developmental ages/stages profoundly impact treatment adherence, comprehension, and efficacy. This feature of the review proved valuable in demonstrating feasibility for multiple ages; however, this also made it difficult to generalize findings across age groups. Effective MBI delivery considers the unique psychosocial needs of youth in each age group.
Study locations
Most studies took place at or in association with large urban medical centers in cities worldwide. Most MBIs were delivered in the outpatient or clinical research setting (n = 10; one offered a virtual option for attendance), four were delivered in schools, and one was delivered inpatient. Future efforts will ideally include MBIs delivered to rural or underserved populations, or otherwise include efforts to ameliorate issues related to distance and transportation to increase access.
Weigensberg et al. 26 described reimbursing participants for transportation as a means of improving engagement. Virtually delivered MBIs may also help to bridge this chasm of accessibility: Chadi et al. 38 demonstrated that electronic delivery of mindfulness meditation was equally as efficacious as in-person delivery for a variety of chronic medical conditions, including epilepsy and rheumatologic conditions.
Interventions
Of the six MBIs delivered one-on-one, four were biofeedback interventions. It was posited that the nature of biofeedback lends itself better to individual delivery rather than to a group setting. In addition, these studies assessed individuals with cystic fibrosis, DES, IBS/FAP, and CP—conditions for which biofeedback therapy may involve sensitive parts of the body, particularly in the latter three, and are thus perhaps ideally delivered individually.
In contrast, the nine MBIs delivered in group settings included modalities such as yoga, Tai Chi, guided imagery, and BAM, and the latter two included didactic components. These modalities likely lend themselves better to group delivery: qualitative comments from participants with concussion who received yoga revealed that youth appreciated knowing that they were not alone in managing their chronic condition and its associated challenges. 25 The multifactorial beneficial effects of group practice may come from the unstructured social element of being together in the waiting room, time immediately before/after session, and so on.
Most studies either required or encouraged a home practice element as part of the MBI. In those where home practice was encouraged (but not required), researchers noted that making this a required element would be advisable. In contrast, Paniccia et al. discouraged home practice for safety reasons in efforts to ensure that participants with concussions carefully implemented calculated increases in physical activity. 25 This suggests that home practice may be an important feature of MBI design, but only after extra consideration for participants' developmental stages and unique safety issues.
Strengths
This scoping review provides an overview of the findings of an otherwise under-discussed realm of research. There is a paucity of literature exploring MBIs in any single or group of related nonpain, noncancer, and nonpsychiatric predominant medical conditions in pediatric patients. However, despite the lack of depth in any one condition, the broad scope of this review translates to coverage of a great breadth of different conditions and interventions, allowing for a broad understanding of the types of interventions that can be delivered and a snapshot of conditions that might benefit.
Furthermore, the included studies were conducted in a variety of locations worldwide. This heterogeneity and diversity potentiate the generalizability of the findings across populations, geographic locations, and intervention locations. This review also highlights the importance of both condition-specific and biopsychosocial considerations in study design and delivery to optimize feasibility and acceptability among diverse ages and ethnicities.
Limitations
This scoping review included data from a wide variety of chronic medical conditions and means of delivering MBIs. This heterogeneity does not allow for meta-analysis or in-depth analysis of a singular condition or method of intervention. Ultimately, these observations underscore the need for further research in this specific realm; as the body of available data grows, so too would the potential to conduct systematic reviews with meta-analyses for definitive guidance regarding clinical decision-making.
This review is further limited by the overall small participant pool: among 15 articles, there were only 641 participants, and individual studies had very small sample sizes, averaging 43 participants per study. The smallest study was conducted on only 3 individuals, whereas the largest study involved 162 participants. Thus, it was not possible to draw definitive conclusions regarding the impact of specific interventions upon specific conditions; future research in this area will ideally include larger sample sizes.
Another limitation of this review is variable study quality, as detailed in Table 6. In addition to the small sample sizes, many of the reviewed studies were not designed as RCTs and lacked a control group to comparatively analyze therapeutic impact. In addition, some studies explored objective measures of improvement alone, making it difficult to compare results with studies that specifically explored patient-reported symptomatic improvement, or vice versa.
Most studies did not report the results of long-term follow-up, presenting limitations in understanding the impact of treatment on symptomatology, adherence, and other outcomes along the course of age-related transitions and changes. Long-term follow-up with study participants would yield interesting findings as to the lifelong impact of exposure to MBIs, even beyond the specific condition targeted.
Future considerations
In addition to the essential need for more research in this field, future research should consider assessing numerous other domains particularly relevant to childhood chronic medical conditions. One such domain is quality of life, which is commonly impacted by chronic illness, and for which MBIs have previously shown promise 10 ; others include psychosocial, social, and economic determinants of health to explore barriers to MBI accessibility in this vulnerable patient population. Determining optimal controls for these studies presents challenges and will demand creativity. Interventions that are, by nature, founded on the assumption that participants be actively engaged and put forth effort, generally get better results with greater effort.
Furthermore, these interventions, when enthusiastically engaged, generally hypothesize added gains over time. Thus, there is additional complexity in generating generalizable outcomes. Within the active group alone, one would expect considerable variation in outcomes based on interest, effort, prior experience, general aptitude, and resonance with a given modality. These factors may be even more pronounced when working with children and teens than in an adult population.
Studies comparing outcomes of yoga versus Tai Chi, for example, would need to account for, first, “type of yoga” and “type of tai chi,” as well as consider that some participants may enjoy seated yoga and dislike movement-based Tai Chi, and vice versa. It may be that yoga is very powerful for some people, while Tai Chi is the preferred choice for others. This would dictate, then, that yoga may not be an inherently effective or ineffective intervention, but rather be inherently effective for some and inherently ineffective for others. Given this, research looking at for whom yoga is likely to be most valuable would be compelling, rather than only if yoga can affect a disease state in an undifferentiated population.
Rather than analyzing data collectively from the group (e.g., mean change in outcome measures for the whole active cohort), it may also be revealing to seek subsets of the active cohort for whom the intervention is particularly powerful, and then work to amplify their engagement and study changes in their specific disease and quality of life measures. Studies of MBIs must consider that the work is being done “with” participants rather than “to” participants and must recognize subject individuality in a more pronounced manner than may be needed for a study of a surgical procedural technique or drug trial.
Conclusions
MBIs have been successfully and feasibly delivered in the service of many chronic medical conditions in youth across diverse populations and age groups. These interventions, which address the critical need to support coping in children with chronic conditions, show promise in benefiting symptoms and psychosocial outcomes. Tailoring interventions to condition-specific needs and developmental stages of patients, as well as addressing unique socioeconomic factors faced by each population, contributes to better treatment adherence and satisfaction.
Greater consideration of individual effort, aptitude, and interest by participants is also needed to best determine how to optimize intervention-subject pairing. The high degree of heterogeneity across studies limits collated analysis, at present. However, the existing literature supports the feasibility and acceptability of MBI delivery for several modalities, delivery structures, and health conditions. More high-quality research and potentially innovative research designs are needed to explore the impact of MBIs on nonpain, noncancer, and nonpsychiatric predominant chronic medical conditions in pediatric populations.
Data Availability Statement
Data available within the article or its Supplementary Data.
Footnotes
Authors' Contributions
Study conception and design by D.W.M., J.A.D., M.K.D., and M.M.; background research and data organization by A.W., D.W.M., M.K.D., and R.S.; article procurement and search method director by M.N.; article screening by D.W.M., M.E.C., and M.M.; analysis and interpretation of results and draft article preparation by D.W.M. and R.S.; article review and editing by M.E.C., M.M., J.A.D., and R.S. All authors have accepted responsibility for the entire content of this article and approved its submission.
Author Disclosure Statement
The authors do not have any conflicts of interest to disclose.
Funding Information
This scoping review was generously supported by the Elisabeth Severance Prentiss Foundation. Sources of funding for included research can be found in their original articles as cited.
Supplementary Material
Supplementary Data S1
Appendix A1.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.