
Abstract
Background:
Patients in intensive care units experience high symptom burden during mechanical ventilation (MV). Pharmacologic symptom management is associated with side effects and increased morbidity. Music-based interventions (MBIs) have been associated with reductions in both anxiety in MV adults and pain for critically ill adults, yet their use for the management of other burdensome symptoms has not been evaluated. The purpose of this scoping review is to map the state of evidence for the use of prerecorded music listening MBIs for symptom management in MV adults.
Methods:
A systematic search of the literature was conducted across four electronic databases (PubMed, EMBASE, CINAHL, and Web of Science) for experimental designed studies that measured the efficacy of MBIs for the management of physical and psychological symptoms including anxiety, sedation/agitation, dyspnea, distress, delirium, sleep, stress, fear, loneliness, or depression in critically ill, MV adults between January 1, 1998, and April 18, 2023.
Results:
A total of 643 abstracts and 29 clinical trials were included. Overall, the risk of bias, assessed using the Evidence Project tool, was moderate. MBIs were mostly delivered with headphones using music selected either by investigators or from a limited selection. MBIs were associated with reduced pain, agitation, dyspnea, distress and anxiety, and improved tolerance of MV and sedative weaning. Outcomes of delirium were mixed. No studies explored sleep disturbances, fear, or loneliness.
Conclusions:
Use of MBIs improved symptom experience for critically ill adults during MV. Future studies employing unrestricted patient-preferred music selections and exploring outcomes of sleep quality, psychological distress, and delirium are needed in this highly symptomatic patient population.
Introduction
More than 5.7 million adults are admitted annually to U.S. intensive care units (ICUs), where 20–40% receive advanced respiratory support with mechanical ventilation (MV). 1 Critically ill patients experience significant symptom burden, including high rates of pain, anxiety, delirium, restlessness, dyspnea, confusion, disordered sleep, loneliness, sadness, and fear. 2 –5 MV is associated with more frequent and more intense experience(s) of most symptoms. 6 Symptom palliation is a challenge in the ICU because common pharmacologic treatments for pain, anxiety, and agitation confer increased risk of side effects and are often ineffective. Moreover, deeper levels of sedation used to promote tolerance of MV are also associated with the development of delirium and increased length of stay. 7 However, conversely, undermanaged symptoms of pain, anxiety, and disordered sleep may precipitate delirium and increase the risk of post-traumatic stress disorder. 8 In an effort to balance excessive and inadequate medication use, new guidelines for critically ill adults include recommendations to minimize psychoactive medications and to employ nonpharmacological interventions, such as music listening, to reduce distressing symptoms associated with critical illness and MV. 9
Music based interventions (MBIs) are defined as the use of music to achieve health-related goals. 10 Two major categories of MBI are recognized: music therapy and music medicine. 11,12 Music therapy is delivered by credentialed music therapists in the context of a therapeutic relationship. Music medicine can involve playing prerecorded or live music for patients and may be delivered by nurses or other clinicians without specialized training. 12 Music listening is one of the most requested nonpharmacological modalities for symptom management in the ICU. 13 –15 The use of music listening is included in recommendations as an easy-to-use, low-risk intervention to promote safe and effective symptom management in critical care. 10,16 –18 As such, music listening represents a promising nonpharmacological intervention for MV adults.
The imperative to deliver evidence-based care has led to a rise in the quantity and quality of research examining the health benefits of MBIs in health care settings. A recent systematic review showed that MBIs of 20–30 min in length are beneficial for the reduction of self-reported pain in critically ill adults, but the benefit for people unable to self-report is unclear. 19 In other reviews, MBIs have been associated with reduction in anxiety among critically ill and MV adults. 20,21 However, the effect of MBIs on observed measures of psychological distress, such as agitation, or on other important symptoms, such as sleep, confusion, delirium, and dyspnea, has not been established. Furthermore, the efficacy of MBIs using prerecorded music listening has not been evaluated as prior systematic reviews do not distinguish between the type of MBI, combining music therapy with music medicine, and live music with prerecorded music.
As a result, the efficacy of MBIs employing prerecorded music listening for critical care symptom management during MV ventilation remains unclear. Therefore, the purpose of this scoping review in critically ill, MV adults is to: (1) catalog the symptoms for which MBIs using prerecorded music have been studied; (2) describe the approaches to using prerecorded music to manage symptoms; (3) evaluate the state of the evidence of MBI clinical trials employing prerecorded music; and (4) identify knowledge gaps.
Methods
Protocol and eligibility criteria
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Metanalyses guidelines 22,23 and the protocol was registered on PROSPERO (CRD42020153026). For the purposes of this review, an MBI was defined as a period of listening to prerecorded music. Peer-reviewed, experimental, or quasiexperimental trials that evaluated the effect of an MBI on commonly reported symptoms of pain, anxiety, agitation, delirium, confusion, dyspnea, sleep disturbances, fear, depression, and loneliness in critically ill MV adults were included (Table 1). This review was limited to clinical trials in English or French that assessed the use of MBIs specifically; studies in which music was coadministered as part of a larger protocol of other interventions were excluded as were studies that included live music or nonmusic auditory stimulus (e.g., nature sounds). Studies were excluded if they had a qualitative design, were review articles, published protocols, cost-effectiveness trials, commentaries, or editorials. Participants were limited to adults aged 18 and older, admitted to critical care areas, including medical or surgical ICUs, and who were receiving MV. Patients who were treated for burns were also excluded as this patient population experiences a uniquely high symptom burden, which may influence the outcome of an MBI and the reliability of findings. Studies that examined primary outcome measures of sedation, agitation, relaxation, observed pain, ventilator tolerance, sleep indices, delirium, or sedative/analgesic medication burden and studies that measured subjective reports of dyspnea, pain, anxiety, sleep disturbances, confusion, loneliness, fear, and patient satisfaction were included.
Inclusion and Exclusion Criteria
Information sources and search strategy
An initial exploratory search was conducted in consultation with a university librarian. Once the search terms were refined, studies were identified using search strategies within the PubMed, Embase, CINAHL, and Web of Science databases. Dates were restricted to January 1, 1998—present for all four searches. The first full search was run on March 20, 2022, and was repeated on April 23, 2023. Medical subject heading search terms and free-text words were systematically combined to identify relevant studies (Supplementary Appendix S1). A gray literature search was conducted (RM) using reference lists from identified studies of interest.
Study selection
Relevant results were scanned for duplicates. Next, eligible studies were exported into Covidence software where the title and abstracts were screened by two independent reviewers (R.M. and T.B.) using the eligibility criteria. Studies that did not meet the inclusion criteria were removed. The remaining articles that met the inclusion criteria were screened by full-text assessment. Studies that did not specifically measure distressing symptoms or related outcomes of an MBI in MV adults in critical care settings were removed. A third reviewer (J.H.E.) adjudicated any disagreements.
Data collection
Data were extracted from included studies through full-text review by one investigator (RM). Extracted study characteristics included the following: author; setting; study design; sample size; social and demographic variables; and clinical characteristics at enrollment. Characteristics of MBIs were identified according to CONSORT guidelines for reporting MBIs 24 and extracted. Extracted outcomes included the following: observed measures of pain, anxiety, delirium sedation, agitation, or ventilator tolerance; subjective reports of anxiety, pain, dyspnea, and distress; differences in sedative or analgesic medication requirement; and physiological measurements of heart rate (HR), respiratory rate (RR), systolic blood pressure, mean arterial blood pressure, and diastolic blood pressure (SBP, MAP, and DBP), oxygen saturation, bispectral index of sedation (BIS), and change in electroencephalogram (EEG). Due to the heterogeneity of symptoms and outcomes measured, a meta-analysis of findings was not performed. A narrative synthesis of the findings was conducted and is presented in text and tables. (Supplementary Appendix S2).
Risk of bias
Risk of bias was determined by two reviewers (R.M. and T.B.) using the Evidence Project risk of bias tool. 25 The tool consists of eight criteria designed to assess risk of bias across a wide variety of study designs, including quasiexperimental and observational studies, and has a high inter-rater reliability. Each article was assessed for its adherence to the criteria outlined in the tool. Because clinical characteristics may influence the results of MBIs in critical care, the authors expanded assessment of baseline sociodemographic equivalence between groups to include important clinical characteristics such as length of stay, length of MV, arousal level, and diagnoses.
Results
Study selection
The literature search revealed 900 citations for review. After removing duplicates, 634 studies remained. After a review of the title and abstract, 573 did not meet the screening criteria and were eliminated. The full text of the remaining 61 articles was then assessed. Of these, 32 more were excluded because they did not meet the inclusion criteria. A total of 29 studies were identified for the final analysis (Fig. 1). Two citations 26,27 were identified from the same research study and are reported together.
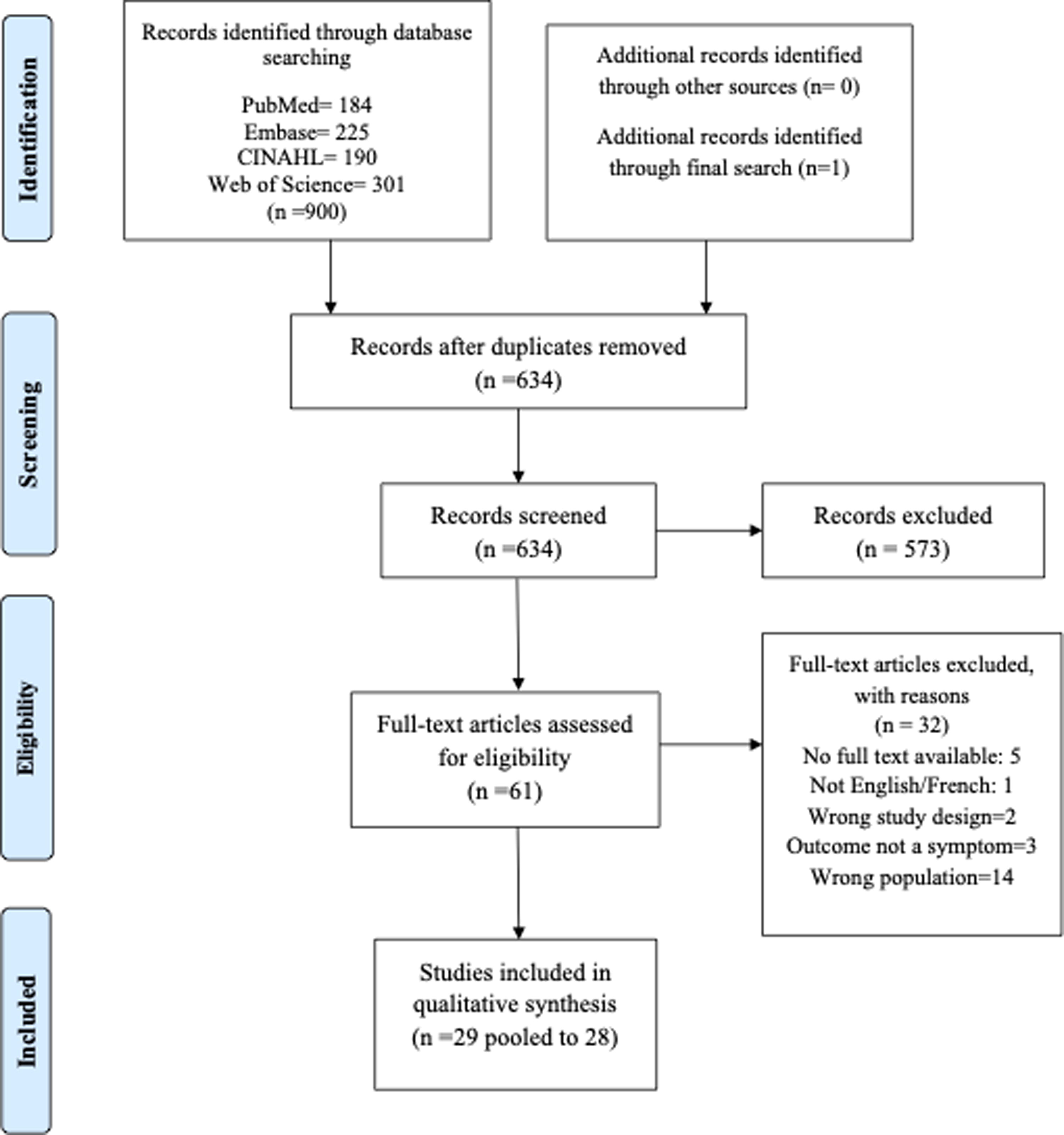
PRISMA flow diagram.
Risk of bias
None of the reviewed studies met all eight rigor criteria outlined in the Evidence Project risk of bias tool, resulting in an overall medium risk of bias (Table 2). Several studies had high rates of attrition, common in critical care studies. Notably, studies that examined a single application of music listening had high completion rates. Study participants were well matched overall across treatment arms for reported sociodemographic measures. Critically, comparison groups were equivalent across important, potentially confounding clinical features such as length of stay, length of mechanical ventilation, and diagnoses.
Quality of Evidence Using the Evidence Project Risk of Bias Tool
Y = met, N = not met.
Control group more sedatives.
Baseline cortisol differed between groups.
Combined Lee et al articles for reporting (single cohort).
Higher baseline carbon dioxide level in music group.
NR, not reported; NA, not applicable.
Parity of baseline outcome measures between comparison groups was largely balanced, adding to study validity. Sample size, effect size, and power analysis do not feature in the Evidence Project risk of bias tool and would likely add significant risk of bias to several included studies. Many were exploratory, pilot, or feasibility studies with small sample sizes and were not designed to measure symptom outcomes. On their own, these smaller studies are at high risk of bias, but this is mitigated by the consistency of results they shared with other more rigorous studies in the group.
Study and sample characteristics
All reviewed studies had convenience samples, including 1753 participants (Table 3). Twenty-five used randomized designs and six were crossover trials. 31,41,47,48,53,50 Sample size ranged from 6 to 373 participants. Studies were conducted in 11 countries, including in Western Europe, 28 –30,37,38,40 –42,44,48,49 the Middle East, 36,45,54 Asia, 26,27,39,46,53,50 and North America. 31 –35,43,47,51,52 The participant age ranged from 34 to 85 years (mean 65.92) and 47.3% (n = 829) were female sex. Race and ethnicity were reported in only five studies, 32 –34,43,47 all of which were conducted in the United States where most participants were white (84.6%). Participants were described as clinically “stable” and were enrolled 1 to 16 days after admission to the ICU. The majority of patients were described as “awake,” “co-operative,” or able to “respond”; many studies stipulated the exclusion of any patients receiving continuous sedation. Only one study included agitated patients, 50 and seven included patients with decreased level of consciousness or who were sedated. 31,34,35,42,48,51,52,54 Ventilator settings were reported in 14 studies; of these only seven included spontaneous breathing modes. Any qualitative observations and adverse events were extracted (Supplementary Data S1 and S2). 38,42,44,46,47,49,50
Study and Sample Characteristics
AC, assist control; APACHE, acute physiology and chronic health evaluation; BIS, bispectral index of sedation; CAM, confusion assessment method; CVICU, cardiovascular ICU; ETT, endotracheal tube; FiO2, fractional inspired oxygen; GCS, Glasgow coma score; ICU, intensive care unit; LoS, length of stay; MV, mechanical ventilation; NR, not reported; PCV, pressure control ventilation; PEEP, positive end expiratory pressure; PSV, pressure support ventilation; RASS, Richmond Agitation Sedation Scale; SAS, Sedation Agitation Scale; Trach, tracheostomy tube.
Theoretical framework
Few investigators described formal theoretical models to support their hypotheses; four suggested theories of the Environment (including Nightingale’s) as a framework for exploring the mechanism by which MBI may affect patients in critical care, 30,48,52,50 and three proposed a cognitive neuroscience theory of meaningful stimulation (Table 4). “Distraction” 27,39,44 and entrainment 32,46 were suggested by five study authors as a means to support the mechanism of music-induced symptom relief, and one group discussed a theory of Holism. 36 The majority of studies discussed psychophysical or psychoneurological models, in which music stimulates the hypothalamic–pituitary axis and limbic system to affect symptom state, but these mechanistic explanations were mooted as hypothetical models, not as tested theories. 28,30,31,33,35,40,42,47,53
Music Interventions
Specific music selections when reported are listed in Supplementary Appendix S3.
Recorded music listening intervention
Participants (or their surrogates) in 10 studies were offered a choice of music styles from a limited selection list of Western or Chinese classical, country, jazz, “oldies,” Chinese traditional, new age, religious music, or movie scores
26,27,32
–34,38,39,45,46,52,53
(Table 4). Two study investigators offered patient-preferred music with restrictions on tempo and mood (described as relaxing); the process for identifying patient-preferred music was not described.
41,47
Three study designs used unrestricted choice of music.
43,49,50
The remaining 12 studies used music selected by investigators: Western classical music
30,31,35,40,42,44,51
; Sufi compositions
28,29
; “New Age” music
48
; or instrumental music.
37,54
Most music selections were described as “relaxing,” of a “slow rhythm” often limited to 60–80 beats/min, however, one group included faster tempo pop songs.
50
All but two of the studies used headphones for music delivery. Participants listened to music for a fixed length of time ranging from 20 min to 240 min in all but one study where MBIs were patient-initiated and the mean listening time was 79.8 min/day.
34
MBIs were delivered once,
27
–30,32,33,35,40,41,44
–46,48,52,53,50
twice in one day,
31,36,37,43
three times in 12-h intervals,
38
or daily over the length of the study period.
36,42,47
–49
Time of day of MBI varied with many protocols using morning (9:00 or 10:00
Control or comparator conditions
In 10 studies, the control condition was a period of resting quietly with noise cancellation headphones 27,31,34,35,39,40,45,46,48 or with noise reduction earplugs. 37 One group used stereo headphones without noise cancellation 51 and five included a third condition of resting quietly without headphones. 34,37,39,40,49 Two studies compared patient-selected music (obtained from streaming services) with investigator-selected music. 43,50 Of these, one study described patient-selected music as preferred music constructed of an unrestricted playlist of favorite songs. 50 In the other, patient-selected playlists were described only as personalized and developed by investigators based on information about music preferences (genres, instruments, artists) from patient surrogates. 56 Two studies did not describe the type of control condition used. 44,47 The remaining studies compared an MBI to a period of controlled rest, or usual care without noise cancellation.
Symptoms measured
The most common measured symptom was anxiety 27,32,34,37 –39,43,46,47,52,53,50 (Table 5). The effects of music listening on sedation-agitation were also explored in 12 studies. 30 –32,34,36,37,41,43,48,51,53,50 Procedural pain outcomes were measured in four studies 28,29,42,44 and five explored pain outcomes more generally. 37,41,45,48,54 Stress was measured in six studies 27,31,33,35,39,40 and delirium in three. 36,37,43 Four studies considered outcomes of dyspnea or ventilator tolerance. 47 –49,52 One study measured distress 49 ; no studies measured outcomes of sleep disturbances, loneliness, or fear.
Outcomes of Music Based Interventions
BIS, bispectral index of sedation; BPS, behavioral pain scale; CAM, confusion assessment method; CPOT, critical care pain observation tool; EEG, electroencephalogram (changes); FAS, Facial Anxiety Scale; HR, heart rate; MAP, mean arterial blood pressure; NRS, Numbers Rated Scale (Pain); O2 Sat, oxygen saturation; PDI, psychological distress index; RASS, Richmond Agitation Sedation Scale; RR, respiratory rate; SBP, systolic blood pressure; STAI, State-trait Anxiety Index; VAS-A, Visual Analogue Scale-Anxiety; VAS-D, Visual Analogue Scale-Dyspnea.
Measurements of symptom experience
MBIs were associated with deeper states of sedation when measured with the Ramsay and Richmond Agitation Sedation Scores (RASS) in six of the nine studies that used these instruments. 28,35,37,38,41,50 Subjective reports of anxiety, as measured by VAS and STAI, were lower after an MBI in 7 of 10 studies. 27,32,34,39,52,53,50 MBIs were also associated with lower CPOT and Behavioral Pain Scores (BPS) in six of eight studies that included observed measures of pain. 28,29,37,42,45,54 Self-reported pain was also significantly lower in the music condition in the only study that compared results of the NRS. 41 Of the two groups that measured the symptom of dyspnea, only one noted a significant reduction in VAS of this symptom following an MBI. 47 Participants in the music arm also reported significantly reduced distress using the peritraumatic distress inventory (PDI) in the only study to measure this symptom. 48 Incidence and duration of delirium were not different between the music and control groups 36,43 ; however, both severity and duration of delirium were improved with MBI in the only study that recruited delirious patients. 37 Eight studies reported qualitative findings, including appearances of calm, restful behaviors, falling asleep during MBIs, reductions in agitated behaviors, and subjective reports of feeling “normal” and “calm.” 27,34,35,41,43,48,50 Of the seven studies that addressed adverse events, one study reported a worsening of symptom experience associated with MBIs, 40 and three studies reported early withdrawal from the protocols related to dislike of equipment or music selection. 34,37,41
Physiological parameters
Hemodynamic parameters, including HR, BP, RR, and other measures of breathing, were reported in all but 10 studies (Table 5). Mean HR was decreased after listening to music in seven studies, 27,32,39,41,46,47 but did not vary compared with a control condition in 13 other studies. 28,30,33,35,36,38,40,42 –44,48,49,51 Results were varied for BP assessed as: systolic (SBP), diastolic (DBP), and mean (MAP). Fourteen investigators measured SBP, but only six found a mean decrease in SBP associated with an MBI. 27,30,35,39,41,44 Of the 12 studies that included DBP measurements, only three 30,39,44 showed a reduction after MBIs, and MAP was reduced in the MBI group of only one study 27 out of four, which included this outcome. Six studies measured oxygen saturation 28,30,39,40,44,49 but none observed any significant change after the MBI. Mean RR was reduced in 6 of 16 studies after MBIs. 32,39,41,44,46,47 Paired with this finding, data from one study demonstrated an increase in tidal volume and minute ventilation after an MBI, compared with no change in the control arm. 41 MBIs were associated with a reduction in MV length in three trials 36,37,52 and an increase in tolerance (time) of ventilator weaning trials in a third study. 47 EEG recordings were not different after an MBI in a single study 35 and the BIS was lower after an MBI in one study 41 but was unchanged in a second. 48 Serum biomarkers commonly associated with stress states were measured in four studies with mixed results.
Medication use
MBIs were not associated with reductions in opioid, 31,34,36,40,43 anxiolytic, sedative, or hypnotic use. 31,40 One group of investigators combined all hypnotic, opiate, and anxiolytic medications into a “frequency of use” and a “concentration of dose” measure and reported a reduction of each in the music listening arm compared with the usual care arm. 34 Two groups found improved tolerance of sedation weaning with MBIs compared with without. 35,51
Discussion
To the authors’ knowledge, this is the first scoping review to summarize the current types, uses, and effects of MBIs on commonly experienced symptoms in MV adults. New study findings include the use of MBIs for a wide range of symptoms, such as the relief of dyspnea, delirium, and distress, and support prior research that shows the benefit of music listening for self-reported anxiety in MV adults. Methodological weakness and heterogeneity of outcome measures limit the ability to draw firm conclusions, but, together, these results provide preliminary evidence to support the use of MBIs for symptom management in MV adults. Important physical and psychological symptoms remain understudied and the paucity of studies that include patient choice for music selection represents important areas for future research of MBIs in MV adults.
Symptom outcomes
MBIs were generally associated with improved symptom experience when measured with validated scales or psychometric instruments such as the VAS, RASS, and CPOT. Studies that relied on physiological variables failed to demonstrate an effect. One explanation for these negative findings is that common physiological measurements lack specificity for symptoms experienced in critical care. 57 In fact, none of the validated, reliable tools used to measure pain, sedation-agitation, or delirium in critical care utilizes HR, BP, or RR in their construct; rather they are based on clinical judgment of level of arousal, restlessness, facial expressions, body movements, executive function and responsiveness. 58,59 Some have suggested entrainment as a theoretical model for the mechanism of action of music as a sedative, which has informed the selection of relaxing music with a slower rhythm (60–80 beats/min). 60 However, this theoretical mechanism has not been demonstrated in critical care; noted reductions in mean HR after MBIs are likely coincidental. 61 Slower breaths have been associated with relaxation in healthy adults, 62 however, during MV, variance of RR is limited by predetermined ventilator settings. Similarly, listening to music has been associated with reductions in expression of stress hormones in healthy controls, 63 but cortisol has poor specificity and adrenal responsiveness may be altered in critical care. 64,65 Critically, physiological variables may sometimes demonstrate statistical significance, but, on their own, may not represent a meaningful clinical outcome. As such, the use of these measurements does not advance the understanding of the effectiveness of MBIs for symptom management.
The use of validated measures of symptoms is a strength in several reviewed studies and is consistent with current recommendations for critical care symptom management. 6 Studies that gauge the effectiveness of MBIs against reliable measurements of symptoms also allow for inclusion of less awake, more agitated, or more deeply sedated patients, a factor that will expand the potential applications for treatment with music in critical care. While not amenable to synthesis, the inclusion of other clinically meaningful outcomes, such as tolerance of sedation and ventilator weaning, also adds to the strength of this review. Clinically meaningful outcomes can inform the development of core outcome sets, thereby reducing reporting bias and also increasing the prospect of generating useful results. 66
Expansion of the symptoms of interest to include delirium, dyspnea, and ventilator tolerance is another strength in this review. However, the lack of studies examining the effects of MBIs on other important symptoms, such as sleep quality and psychological distress, is notable. Prior research has shown that the most commonly reported symptom in ICU adults is exhaustion (nearly 75%). 5 Patients also experience restlessness and shortness of breath more often than pain, and they rate sadness, fear, confusion, and exhaustion as equally or more intense than pain or anxiety. 5 Listening to music has been associated with improved sleep in healthy adults 67 and there is evidence that listening to recorded music alone or alongside other mind–body interventions is associated with improved quality and quantity of restful sleep in non-MV critically ill adults. 68,69 Given the importance of adequate sleep, both for symptom experience and prevention of delirium, studies that examine the use of MBIs to treat and prevent sleep disorders represent an important area for future research. MBIs may also address psychological symptoms not amenable to medications. Observations of patients smiling, seeming happy, tapping their feet, and reports that music made them feel normal support this hypothesis. 34,43,50
The narrow focus on a single symptom (often pain or anxiety) in several studies may also have left some improvements in symptom experience underreported. Furthermore, co-occurring symptoms may have confounded the results in several studies in this review. Distressing symptoms rarely exist in isolation in MV adults. For example, pain, fear, anxiety, and dyspnea are often co-occurring and may potentiate one another. 4,9,70 In fact, patients using self-directed music listening during MV, have endorsed a wide range of target symptoms. 71 More recent studies in this review explored multiple symptom outcomes such as dyspnea and anxiety, or delirium and pain. Comprehensive symptom assessment is consistent with current recommendations that call for routine, thorough investigation of symptoms in MV adults. 6 Studies that include holistic assessment of multiple symptoms provide a methodological template for future exploration by acknowledging the relationship between symptoms and widening the lens through which the effectiveness of MBIs are measured.
Finally, variable symptom experience between individuals may also have affected the results. Overall, this review includes a wide range of adults hospitalized in 12 countries adding to the generalizability of the findings. However, results of the reviewed studies may have been influenced by the wide range, and older mean age of the cohort age (>65). Older age is a risk factor for delirium, and few studies screened for this condition. If present, delirium may have affected the results, as hypoactive delirium can dampen a patient’s arousal, and hyperactive delirium may result in increased use of restraints, antipsychotics, or sedatives to maintain patient safety. Meanwhile, most of the studies reported clinical parity of their sample but few reported any social determinants of health when describing their participants. Social determinants of health such as income, marital and employment status, or history of stressful life experiences have been associated with varying symptom experience in patients with chronic disease. 72 In critical care, sociodemographically minoritized patients endorse extreme psychological distress and severe loneliness. 73 Future studies that expand the symptoms of interest and include robust descriptions of the social, economic, and cultural context of the participants may reveal new uses for MBIs and lead to deeper understandings of the mechanism of action of music listening for adults during MV.
Music selection
It is difficult to know what role music selection played in the symptom outcomes. Despite recommendations to tailor music selections to patient preferences, 74 –79 most of the studies in this review (n = 23) limited the choice of music to “traditional,” “instrumental,” or Western classical music. On the surface, testing the effects of a specific, investigator-selected piece of music increases the internal consistency of an intervention. However, personal preferences and degree of familiarity determine these psychobiological responses to music. 80 –83 Individual music preference was rarely reported, and thus, it is unknown how well the investigator-selected music was aligned with patient preference. It is worth noting, however, that in several studies, participants lamented the lack of choice of the music intervention, leading some to withdraw from participation altogether. When choice of music was offered, selection was usually limited to slow tempo “relaxing” music, or a choice between a group of investigator-selected playlists. Yet, studies of adults with altered consciousness suggest that compared with “relaxing classical” or investigator-chosen neutral music, use of preferred music, regardless of tempo, is associated with a stronger effect seen as a greater reduction in agitation after traumatic brain injury, 55 improved level of consciousness after coma, 84 or increased relaxation response during intraoperative anesthesia. 85 Listening to a preferred musical genre or familiar music has also been associated with increased relaxation effect and heightened pleasure arousal in healthy adults. 86,87 While it is not clear if this finding translates to the critically ill patient population, offering patient-centered and patient-selected music selection may confer the increased benefit of an MBI. In fact, the three studies that offered an unlimited personalized selection of music demonstrated a significant relaxation effect. 41,47,50 Given that the basis of these musical preferences is rooted in this sociocultural context, 88 offering access to unrestricted music listening represents a form of culturally humble care and may therefore potentiate symptom response. Prior research also suggests that preferred music for listening during MV may vary by individuals and over the course of their hospitalization. 71 Careful descriptions of the music selection in studies using unrestricted personalized or preferred music are needed, 24 including analyses of the reliability of surrogate selection.
Music intervention delivery
Variations in the control arms and the potential therapeutic effect of noise cancellation headphones may have reduced the strength of some findings. Critical care units are plagued by high noise levels and the World Health Organization has made recommendations to offer earplugs or headphones to reduce this. 89,90 In addition, headphones themselves have been studied for the promotion of sleep and prevention of delirium. 91,92 Maintaining headphone use across both arms attends to concerns of internal validity. Conversely, the use of headphones may add to feelings of disconnectedness and communication barriers especially during MV. Studies that explore the use of ambient music may suffer methodological criticism but may be more pragmatic and acceptable.
The heterogeneity of duration, timing, and frequency of MBIs in these studies precludes any summary conclusions about the optimal length or frequency of MBIs, however, the wide variety of symptoms included in this broad review likely requires varied management approaches. 71 Research exploring cognitive processing of music suggests that adults are affected by listening to music within minutes 93,94 and that MBIs of short duration (10–15 min) are associated with improved levels of arousal during coma recovery. 95,96 This rapid onset of effect may help explain why short MBIs were effective for the management of procedural pain in this review. Similarly, MBIs have been associated with reduced emergence delirium and increased satisfaction after general anesthesia compared with controls. 97 This could explain the improved symptom experience of patients in this review who received an MBI during or immediately after surgery with general anesthesia. While the onset of action may occur within minutes, MBIs of longer duration were well tolerated. It remains unclear how long MV patients are affected by an MBI. This highlights an important area of research for critically ill, MV patients: optimal frequency timing and duration of MBIs, which is likely to depend on the symptom of interest.
Limitations
This review was limited to published peer-reviewed journals and may be affected by publication biases. Two gray literature citations appeared to meet the inclusion criteria but were unpublished data. Other relevant citations were only available as conference abstracts, with limited data on methods and results, and were therefore excluded. A second limitation of this review is that the search was limited to publications in English and French: at least four other studies met the inclusion criteria but were published in other languages.
Conclusions
This study demonstrates improved self-reported symptoms associated with MBIs in awake, responsive MV adults. In addition, changes in observed pain, agitation, sedation level, and ventilator tolerance were appreciated in adults unable to self-report due to altered levels of consciousness. Unlike prior reviews, MBIs were not associated with changes in vital signs. Instead, the use of validated psychometric instruments provided evidence of the effect of MBIs on symptoms of pain, anxiety, agitation, dyspnea, and distress. There remain substantial opportunities for expanded MBI use, including testing varied music types and their effect on sleep quality, psychological well-being, and ventilator tolerance. Future clinical trials that seek to maximize the potential therapeutic benefit of an MBI in MV adults will benefit from research that identifies reliable, meaningful measures and that helps explain the underlying mechanism of action of a music intervention.
Footnotes
Acknowledgments
The authors acknowledge Min-Lin Fang for her work in helping to develop and refine a search strategy. This research is based upon a dissertation titled: Recorded Music Listening Interventions for Symptom Management During Mechanical Ventilation in Critical Care, written by the first author, in partial fulfillment of a PhD at the University of California, San Francisco, conferred June, 2022.
Authors’ Contributions
R.M.: Conceptualization, methodology, investigation, formal analysis, and writing—original draft. T.B.: Data curation, formal analysis, and writing—review and editing. H.L.: Conceptualization and writing—review and editing. J.T.: Conceptualization and writing—review and editing. J.J.: Methodology, writing—review and editing, and supervision. J.H.-E.: Methodology, validation, writing—review and editing, and supervision.
Author Disclosure Statement
None of the coauthors has any competing interests or anything to disclose.
Funding Information
Rebecca Menza received a Dean’s Fellowship from the Graduate Division of the University of California San Francisco to support her doctoral research including this study. The other authors received no financial support for the research, authorship, or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.