
Abstract
Objective:
To evaluate the efficacy and safety of ultrasound-guided acupotomy (UgA) for the treatment of thoracodorsal myofascial pain syndrome (TDMPS) and monitor its mid-term efficacy at 3 months after treatment.
Methods:
A 3-week, evaluator-blinded randomized clinical trial was conducted among 100 patients with TDMPS (visual analogue scale [VAS] score > 3) in the outpatient clinic of the Department of Orthopaedics of the Second Affiliated Hospital of Anhui University of Traditional Chinese Medicine, with a 3-month follow-up starting after completion of treatment. These patients were randomly assigned to receive UgA (n = 50) or oral celecoxib (n = 50). Recruitment was conducted between January 2021 and July 2022. The primary outcome was the VAS score, and the secondary outcomes included the Oswestry Disability Index (ODI), Pain Anxiety Symptoms Scale (PASS), and TNF-α and IL-1β levels. Outcome data were collected at baseline, week 3 (post-treatment) and week 15 (follow-up).
Results:
Compared with that in the celecoxib group, the pain in the UgA group was alleviated more strongly, with an adjusted mean group difference of −0.69 (95% CI,−1.07 to −0.31 after multiple imputation) at week 3 and −1.96 (95% CI,−2.33 to −1.59 after multiple imputation) at week 15 (p < 0.001 for overall group × time interaction). Both groups exhibited improvements in the ODI and PASS scores at weeks 3 and 15, but these improvements were significantly greater in the UgA group (p < 0.05). At week 3, the TNF-α and IL-1 levels were significantly lower in both groups, but celecoxib was more effective (p < 0.05). Results from analyses with multilevel multiple imputation for missingness were similar.
Conclusion:
UgA led to greater and safer alleviation of pain, dysfunction, and pain anxiety in patients treated with TDMPS than did celecoxib and had a durable 3-month efficacy but was inferior to celecoxib in reducing the level of inflammatory factors. These findings may prompt clinicians to recommend UgA as an alternative and supplementary therapy for pain management in patients with TDMPS.
Introduction
Thoracodorsal myofascial pain syndrome (TDMPS), which is a form of chronic musculoskeletal pain that can cause localized or widespread pain characterized by painful myofascial trigger points (MTrPs) of compression pain in the taut bands of muscle fibers, is a highly prevalent and burdensome condition. 1,2 Back pain alone costs £1.6 billion in direct costs and £10 billion in indirect costs each year in the UK. 3 With a lifetime incidence of up to 85%, TDMPS accounts for approximately 15–20% of patients in general outpatient clinics, is very common in people aged 20–50 years, is more prevalent in females than in males, and is not strongly age related. 4,5 Upper back pain has received far less attention than lower back and neck pain, although it appears to have comparable features and can be problematic in work and everyday activities. 6
Several studies have proposed a variety of interventions to manage or prevent myofascial pain syndrome (MPS), including medications, 7,8 manipulation and physical therapy, 9 dry needling, 10,11 MTrP injections, 10 and botulinum toxin injections. 12 Noninvasive treatments do not provide long-term pain relief, and pharmaceutical injections or oral administrations are limited by adverse effects. 13,14 The myofascia are connective tissues that surround and adhere to bony prominences. Repeated and protracted myofascial stressors can produce myofascial tightness and hypertrophy, resulting in the production of tense and spastic nodules, tensioned strips, or MTrPs, which pull and irritate the neurovascular system that runs through them, resulting in the onset of symptoms. According to Simons and Travell, the keys to treating MPS are to inactivate MTrPs, release contracture bundles in the muscle, correct homeostasis, and eliminate potential triggers. 15,16 Acupotomy serves as both an “acupuncture” and a “scalpel” in traditional Chinese medicine. By directly cutting and loosening the MTrPs, the tension on the fascial surface can be lowered, and the pressure in the fascial cavity can be reduced, thus eliminating irritation and compression on the sensory nerve endings and relieving pain. And acupotomy has been successfully used to treat chronic pain and various muscular diseases. 17,18 However, it is worth noting that our patient’s discomfort was in the chest and back, and a “back as thin as article” was observed during acupuncture. Owing to the relatively thin muscle tissue in the back and the position of the chest wall in relation to the intercostal space, there is a higher risk of pneumothorax following back acupotomy, according to multiple findings in the literature. 19,20 Moreover, considering the high variability of manual identification and treatment of MTrPs in daily practice by different operators under blinded conditions, 21 some authors have suggested that ultrasound imaging can be optimized for the diagnosis and management of myofascial pain and that the classical sonographic feature of MTrPs is a hypoechoic nodule with well-defined borders and a heterogeneous internal echotexture. 22 –24 Several studies have examined the possibility of ultrasound-guided acupotomy treatment for knee osteoarthritis, 25 entrapment of the inferior patellar branch of the saphenous nerve 26 and cervical spondylotic radiculopathy. 27 But there are fewer studies on ultrasound-guided acupotomy (UgA) therapy for TDMPS. To determine whether UgA can be used as an alternative therapy for secure and efficient pain relief, as well as to provide useful references for the application of this therapy and clinical studies of the disease, we conducted a 3-week single-blind randomized clinical trial of UgA versus celecoxib for the treatment of patients with TDMPS with a 3-month follow-up.
Materials and Methods
Study design
A 3-week evaluator-blinded randomized clinical trial with a follow-up period of 3 months at the end of the treatment was conducted on 100 TDMPS patients from the outpatient clinic of the Department of Orthopaedics I of the Second Affiliated Hospital of Anhui University of Traditional Chinese Medicine to validate the effects of UgA on pain, function, anxiety, and inflammatory factors in the TDMPS. All participants provided oral and written informed consent before study inclusion. This study was conducted according to the CONSORT statement, and all subjects signed a written informed consent before inclusion in the study. This study was approved by the Ethical Review Committee of the Second Affiliated Hospital of Anhui University of Traditional Chinese Medicine (2023-zj-08) and registered at Research Registry (www.researchregistry.com Researchregistry10031).
Participants
Participants were patients with TDMPS in the outpatient clinic of the Department of Orthopaedics I at the Second Affiliated Hospital of Anhui University of Traditional Chinese Medicine. Recruitment took place from January 2021 to July 2022. The inclusion criteria were as follows: patients who (1) met the diagnostic criteria for MPS; 28 (2) had a chief complaint of upper back pain (visual analogue scale [VAS] score >3); (3) were between 23 and 65 years of age; and (4) were not treated with other methods of treatment or oral medication within 2 weeks of onset. The exclusion criteria were as follows: patients who (1) were allergic to celecoxib or were unable to complete the acupotomy treatment; (2) had severe coagulation disorders; (3) were pregnant or considered pregnant within the study period or had cognitive dysfunction; (4) had localized skin breakdown or erythema; (5) had comorbid discogenic cervical and lumbar spondylosis, ankylosing spondylitis, or rheumatism; and (6) had comorbid cardiovascular, cerebrovascular, hepatic, renal, or other serious visceral diseases or psychiatric disorders. All study treatments were provided free of cost.
Randomization and blinding
After recruitment and baseline measurements, a trial coordinator independent of the intervention team used SPSS 26.0 software to generate randomized numbers in sealed envelopes. Therapists opened the envelopes sequentially in front of the patients and randomly assigned them in a 1 per 1 ratio to the UgA group or the Western medicine group for treatment. A single-blind design was used with blinded allocation for the participants and assessors but not the therapists or statisticians. All eligible participants were treated by the same physician.
Interventions

Procedure of ultrasound-guided acupotomy. The red arrow marks the myofascial trigger point, and the white circle highlights changes in its thickness before and after treatment. With the patient prone, the physician locates the approximate position of the myofascial trigger point through palpation, then locates the thickened trigger point using ultrasound
Outcome and follow-up
Participants completed questionnaires and tests of their inflammation levels at baseline, week 3 and week 15 (3 months after treatment). The primary outcome was a valid and reliable self-reported level of upper back pain. 30 The VAS uses a traveler’s scale of approximately 10 cm in length with 10 large scales and 100 small scales with 0 points (for no pain) and 10 points (for intolerable worst pain) to allow the patient to indicate a value representing the level of pain based on self-perception to evaluate immediate subjective pain. The VAS has demonstrated reliability, validity, and sensitivity to change. 31 The secondary outcome indicators included functional impairment, pain anxiety symptoms, and inflammatory factor levels. The Oswestry Disability Index (ODI) consists of nine components, with the Cronbach’s alpha for internal consistency reaching 0.93. 32 For this study, the ODI was slightly modified by replacing “leg pain” with “chest and back pain.” The Pain Anxiety Symptoms Scale (PASS), which consists of 20 items, was used to assess patients’ pain-related anxiety and fear. The scale has good reliability, validity, and internal consistency (Cronbach’s αs = 0.72–0.92) in the Chinese population. 33 Tumor necrosis factor alpha (TNF-α) and interleukin-1beta (IL-1β): TNF-α and IL-1β were measured in patient serum by enzyme-linked immunosorbent assay (ELISA) with strict reference to the instructions of the kit.
Sample size calculation
After reviewing the literature, 34,35 α = 0.05, β = 0.10, P1 = 93%, and P2 = 70% were set for this study (P1 and P2 are the predicted clinical effectiveness rates of the two treatment regimens, respectively, as determined by the previous literature and our clinical experience). Calculations using the PASS software yielded n = 90, and the final sample size was determined to be 100 patients according to the 10% loss-to-follow-up ratio.
Adverse events
Patient-reported adverse effects and adverse events, such as gastrointestinal reactions, hematomas, neurological injuries, and severe pain, were registered and discussed after weekly treatments.
Statistical analysis
All the statistical analyses were performed using IBM SPSS Statistics 26.0. The significance level was set at p < 0.05. Measurements are expressed herein as the mean ± standard deviation (
Results
Baseline characteristics
Between January 2021 and July 2022, 100 patients were randomly assigned to the UgA group (n = 50; males = 21, females = 29) or the celecoxib group (n = 50; males = 19, females = 31), with the last participant completing follow-up in October 2022. Ninety-five (95%) patients finished their therapy, and 87 (87%) patients finished their follow-up. The dropout rate was 8% (4/50) in the UgA group and 14% (7/50) in the celecoxib group at 15 weeks. Figure 2 depicts the flow chart for the investigation. Table 1 displays the demographic and clinical baseline data.

Patient enrollment flowchart. Visual Analogue Scale score indicates visual analog scale.
Baseline Characteristics of the Study Participants
BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); SD, Standard deviation; UgA, ultrasound-guided acupotomy.
Primary outcomes
Table 2 shows the VAS scores of the two study groups. Patients in the UgA group had additional improvements in VAS scores of -0.69 (95% CI, −1.07 to −0.31; p < 0.001) at week 3 and −1.96 (95% CI, −2.33 to −1.59; p < 0.001) at week 15 compared with those in the celecoxib group. The UgA treatment was more effective at improving pain (p < 0.001 for overall group × time interaction).
Primary Outcomes at Baseline, 3 and 15 Weeks
Mean differences between groups were adjusted for sex, age, body mass index, pain area, and disease duration.
NA, not applicable; UgA, ultrasound-guided acupotomy; VAS, Visual Analog Scal.
Secondary outcomes
Compared with those in the celecoxib group, participants in the UgA group had additional improvements of −5.92 (95% CI,−8.49 to -3.35) in the ODI and −4.10 (95% CI, −6.79to-1.41) in the PASS at week 3; −9.36 (95% CI, −11.80to-6.92) in the ODI; and −4.18 (95% CI, −6.61to-1.75) in the PASS at week 15. Compared with participants in the celecoxib group, participants in the UgA group had more significant efficacy in terms of the ODI (p < 0.001 for overall group × time interaction) and PASS (p < 0.001 for overall group × time interaction) (Table 3). The changes in the VAS score, ODI score, and PASS score between the two groups are shown in Figure 3.
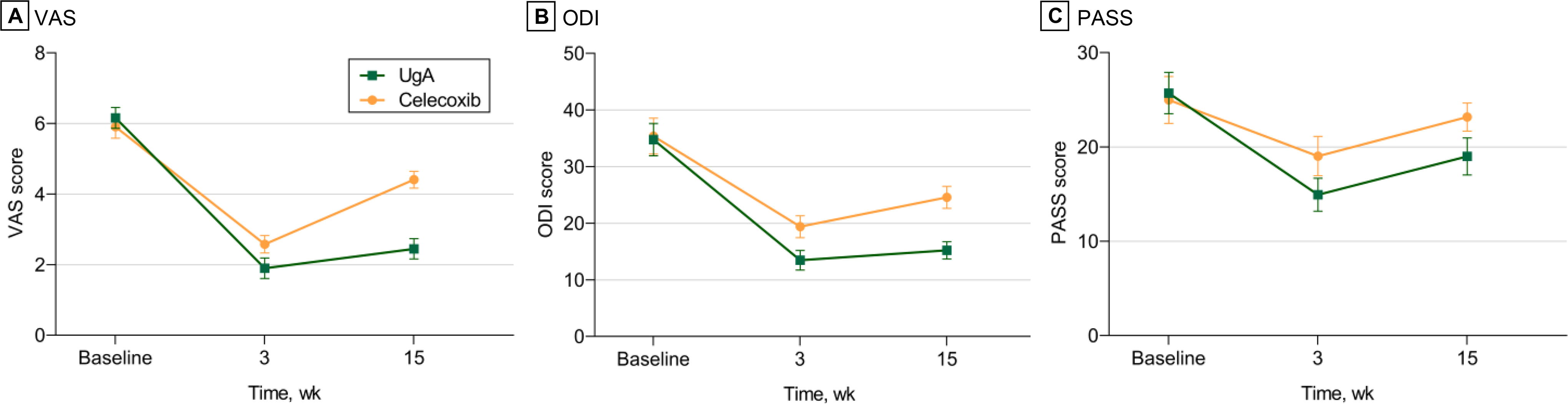
The change in Visual Analogue Scale (VAS) score, the Oswestry disability index (ODI) and Pain Anxiety Symptoms Scale (PASS) scores at baseline, week 3 and week 15 of treatment for ultrasound-guided acupotomy (UgA) and Celecoxib. The green line indicates UgA and the orange line indicates Celecoxib; diamonds indicate the mean scores of the outcome measures observed at each assessment; and the vertical line through each diamond indicates the 95% CI of the mean scores.
Secondary Outcomes of ODI and PASS at Baseline, 3 and 15 Weeks
Mean differences between groups were adjusted for sex, age, body mass index, pain area, and disease duration.
NA, not applicable; ODI, Oswestry disability index; PASS, Pain Anxiety Symptoms Scale; UgA, ultrasound-guided acupotomy.
At week 3, TNF-α and IL-1β levels were significantly lower in both groups (p < 0.05) and were lower in the celecoxib group than in the UgA group (TNF-α: 36.81 ± 7.71 [UgA group] versus 28.31 ± 6.56 [celecoxib group], p < 0.001; IL-1β: 67.61 ± 9.52 [UgA group] versus 57.65 ± 6.89 [celecoxib group], p < 0.001) (Table 4).
Secondary Outcomes of TNF-α and IL-1β at Baseline and 3 Weeks
There is a statistically significant difference before and after treatment in the same group (p < 0.05).
NA, not applicable; UgA, ultrasound-guided acupotomy.
Adverse events
No serious adverse reactions were observed in the UgA group, and some patients developed bruises caused by subcutaneous bleeding; these lesions subsided on their own, and the patients continued treatment after an explanation. In the celecoxib group, there were five cases of gastrointestinal reactions, including diarrhea, nausea, loss of appetite, fatigue, vomiting, and gastric discomfort; 2 patients continued treatment after the symptoms disappeared with an oral gastric mucosal protector, and 3 patients withdrew to seek other treatments because they did not want to take oral medications.
Discussion
Our results showed that UgA significantly improved upper back pain, functional disability, pain anxiety, and serum inflammatory factor levels in patients with TDMPS during the observation period and was particularly superior to celecoxib in improving upper back pain, function, and pain anxiety. However, celecoxib was superior to UgA in lowering TNF-α and IL-1β levels. In addition, there were few significant adverse effects throughout the course of treatment and follow-up.
To our knowledge, there are few studies on the treatment of upper back pain, and there are no comparable randomized controlled trials evaluating the clinical effectiveness of UgA therapy for treating patients with TDMPS. These findings may provide new perspectives for the treatment of TDMPS. Myofascial pain is prone to recurrence in clinical practice, and the repeated use of Western medications is obviously unwise. UgA can be used as an alternative and complementary therapy to analgesics to help patients with TDMPS experience more significant and long-lasting pain relief while also successfully reducing the side effects of medication, which is desirable for clinical promotion and application.
Acupotomy combines the “needle” approach of traditional Chinese medicine acupuncture with the “knife” approach of modern surgery. 37 In addition to the usual effects of acupuncture, acupotomy can also directly cut, peel, and loosen adhesions, which lowers internal fascia stress while boosting local blood flow and enhancing tissue metabolism. Moreover, acupotomy has certain effectiveness, a short treatment course, and a long-term impact and is frequently employed in the therapeutic treatment of chronic soft tissue injuries. We discovered a study 38 that used acupotomy, acupuncture, and fascial release to treat 83 MTrPs of 43 MPS patients. The findings revealed that acupotomy was more effective at reducing patients’ discomfort and restoring their mobility. Our study used musculoskeletal ultrasound based on traditional acupotomy to determine the hierarchical anatomical structure of the MTrP points in patients with TDMPS more clearly as well as to clarify the position, angle, depth, and range of acupotomy entry and acupotomy loosening during acupotomy treatment to prevent accidental stabbing into the thoracic cavity and thereby avoid causing pneumothorax. Our findings demonstrated that patients’ pain, dysfunction, and pain anxiety status significantly improved following acupotomy treatment compared to baseline; even though symptoms recurred at follow-up, they were still significantly improved compared with baseline, and there were no significant adverse reactions throughout the entire treatment period. These findings suggest that UgA can not only effectively treat TDMPS but also compensate for the differences in judging the depth of MTrPs and the operation level of different operators to improve safety.
In addition, we found that the clinical efficacy of UgA in TDMPS was more durable compared with celecoxib over a 3-month observation period. Research 39,40 has shown that NSAIDs prolong contraction-induced mechanical nociceptive hypersensitivity of muscles while having analgesic effects on MPS and that short-term usage temporarily reduces pain in individuals with persistent back pain. Oral celecoxib treatment is effective at relieving upper back pain in patients during the administration period, but the effect does not improve significantly as the blood concentration in the body decreases after administration, and the efficacy is not as good as that of the UgA group during the treatment period or at the follow-up.
The local environment of MTrPs contains increased concentrations of inflammatory mediators, neuropeptides, catecholamines, and cytokines. 41 TNF- and IL-1, key members of inflammation-related diseases, are important factors in the production of pain and induce the release of a variety of pro-inflammatory mediators. 42 During the course of MPS, TNF-α reduces the propagation of inhibitory synapses through the spinal cord, stimulates the release of additional proinflammatory cytokines, and induces immune and glial cell proliferation, increasing neuroinflammation and pain propagation, whereas IL-1β induces primary neurofibrillary hypersensitivity, leading to pain hypersensitivity. 43 Consistent with the findings of previous research, 44 the current study showed that acupotomy significantly reduced the serum TNF-α and IL-1 levels in TDMPS patients, suggesting that acupotomy inhibited the expression of inflammatory factors such as IL-1 and TNF-α, improved local soft tissue adhesions and inflammatory infiltrates, and relieved muscle pain. This study also revealed that celecoxib reduced these parameters more significantly than acupotomy did, possibly because of the ability of celecoxib to inhibit prostaglandin production by inhibiting cyclooxygenase-2 (COX-2), which in turn inhibits the expression of various inflammatory factors, an advantage of NSAIDs. However, because of the high pressure within myofascial trigger points, acupotomy not only releases the pressure on the interfascial compartments through the loosening of soft tissue adhesions with chronic aseptic inflammation but also reduces inflammatory factor levels through the stimulation of local pressure points to cause tissue proteolysis. This makes UgA more effective at releasing myofascial trigger points because it stops the stimulation and compression of sensory nerve ends and alleviates pain.
Strengths and limitations
Our trial had several limitations. First, we were unable to complete the testing and analysis of serological indicators at 3 months of treatment, and the timeline of the evaluation indicators was not complete enough; a more systematic and complete recording of the indicators is needed in further studies. Second, shedding data in this study exceeded expectations for various reasons, and we used the multiple imputation method to fill in missing data, which may increase the risk of committing a Type II error, but the results of our study still showed a significant difference between the two groups. Our study provides preliminary evidence about the effectiveness of this treatment, and future studies of ours will expand the sample size and strictly control the dropout rate and group assignment to enhance the reliability of the results. Our study has several advantages. To the best of our knowledge, this is the first study to investigate UgA therapy for TDMPS, providing new ideas and methods for clinical treatment. In addition, this study had a 3-month follow-up period and a large experimental sample, which ensured sufficient statistical power to detect clinical efficacy.
Conclusions
In this randomized clinical trial, UgA led to greater alleviation of pain, dysfunction, and pain anxiety in TDMPS patients than did celecoxib and had a durable 3-month safe efficacy but was inferior to celecoxib in reducing the level of inflammatory factors. These findings may prompt clinicians to recommend UgA as an alternative and supplementary therapy for pain management in TDMPS patients and reduce the need for medication in patients with chronic pain.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Footnotes
Acknowledgments
The author thank the patients and staff of the Department of Orthopaedics I of the Second Affiliated Hospital of Anhui University of Traditional Chinese Medicine for their valuable contributions to the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author (J.Z.), upon reasonable request.
Authors’ Contributions
Z.Y.:conceptualization (equal) and writing—original draft. J.Z.: conceptualization and (equal) and funding acquisition. C.W.: supervision and writing—review and editing. L.H.: software, data curation, and formal analysis. Y.N.: methodology. Y.X.: investigation. Z.Z.: resources. All the authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Traditional Chinese Medicine Inheritance and Innovation Research Project of Anhui Province in 2022 (Project No.: 2022CCZC02).