
Abstract
Introduction:
Patients with acute coronary syndrome (ACS) often experience high levels of anxiety, which can significantly impact their prognosis. However, evidence regarding anxiety reduction by aromatherapy in patients with ACS is lacking. This study aimed to investigate the effects of aromatherapy on anxiety in patients with ACS.
Methods:
The literature search was conducted using PubMed, CINAHL, Embase, Web of Science, Cochrane Library, and PsycINFO from their inception until February 21, 2024. Based on inclusion criteria, randomized controlled trials (RCTs) on aromatherapy in patients with ACS aged ≥ 18 years were included. The risk of bias in the included studies was assessed using the revised Cochrane risk-of-bias tool for RCTs.
Results:
A total of 14 studies were included in the final analysis. Aromatherapy significantly reduced anxiety among patients with ACS, with a large effect size (standardized mean difference [SMD] = −1.66, 95% confidence interval [CI]: −2.47 to −0.85). The effect on systolic blood pressure (SBP) was −0.65 (95% CI: −1.15 to −0.15), indicating a moderate effect size, whereas there was no significant effect on diastolic blood pressure. Inhalation therapy demonstrated a large effect size (SMD = −1.70, 95% CI: −2.33 to −1.08), whereas massage therapy did not show a significant effect on reducing anxiety.
Discussion/Conclusions:
The findings show that aromatherapy can effectively reduce anxiety and SBP in patients with ACS. In particular, inhalation therapy showed a significant effect on reducing anxiety levels. Applying aromatherapy in clinical settings to reduce anxiety among patients with ACS should be considered. However, the limited number of studies analyzed hinders a comprehensive evaluation of the effectiveness of massage therapy. Hence, further research is necessary to elucidate its potential role in reducing anxiety among patients with ACS.
Introduction
Acute coronary syndrome (ACS) encompasses all the acute clinical symptoms resulting from an imbalance in the blood supply to the myocardium. It is a type of ischemic heart disease characterized by the rupture of vulnerable plaques in the coronary arteries or the formation of a thrombus, leading to acute chest pain and myocardial ischemia. 1,2 According to statistical data from the American Heart Association, approximately 790,000 Americans die each year from myocardial infarction, a form of ACS. 3 Generally, patients with ACS experience limitations in daily activities and occupational functioning. Despite advancements in medical therapy and interventions, ACS remains associated with a high incidence of myocardial infarction and mortality rates. 4
Once ACS occurs, patients typically experience chest pain, a known clinical symptom, and are closely observed and treated in the coronary care unit (CCU). During this time, patients with ACS may experience anxiety because of the numerous medical professionals, unfamiliar medical devices, and unfamiliar environment. 5 Moreover, anxiety has been reported to be associated with an increased risk of mortality and adverse cardiovascular events in patients with ACS. 6 In addition, anxiety activates lipid deposition within the blood vessels, thereby increasing the incidence of atherosclerosis. Anxiety is also correlated with the risk of ventricular arrhythmias and a 36% increase in the risk of adverse cardiac effects in patients, 7 confirming that anxiety has a significant impact on the prognosis of patients with ACS. Therefore, reducing anxiety in patients hospitalized for cardiovascular diseases because of ACS is considered crucial for their treatment and prognosis.
Generally, pharmacological and nonpharmacological methods can be applied to reduce anxiety. 8 Pharmacological methods offer several advantages, including immediate relief and widespread applicability. Anxiolytic drugs not only offer rapid relief from acute anxiety symptoms but also are frequently simpler to administer. However, caution is needed when using these medications in patients with cardiovascular diseases. When administering selective serotonin reuptake inhibitors, which are commonly used as anxiolytics, to patients with cardiovascular diseases, side effects such as increased anxiety, insomnia, or agitation may occur during the first few days. 9 In addition, benzodiazepines such as lorazepam, commonly used to reduce anxiety symptoms, may exhibit side effects such as central nervous system depression, bradycardia, hypotension, and syncope, especially when used concurrently with sedatives, opioids, or muscle relaxants. 10 Especially considering that opioids such as morphine are commonly used to manage chest pain commonly seen in patients with ACS, 11 particular caution is warranted when administering these drugs to patients with ACS.
In addition, various nonpharmacological interventions such as aromatherapy, 12 cognitive behavioral therapy, 13 respiration therapy, 14 and mindfulness 15 are utilized to reduce anxiety. Recently, there has been a growing trend toward utilizing complementary and alternative therapies as a nonpharmacological approach to manage anxiety, as they have fewer complications. 16 Particularly, aromatherapy is widely utilized as one of the various complementary and alternative therapies for alleviating anxiety. Aromatherapy involves applying essential oils extracted from various parts of plants to the skin through massage and inhalation methods. This trend is increasing because of its low cost and minimal side effects, making it effective for managing various conditions such as depression, anxiety, pain, vomiting, and sleep disorders. 17 Aromatherapy stimulates the olfactory receptors, which transmit information to the limbic system in the brain, ultimately leading to the release of endorphins, serotonin, and enkephalins, which can help alleviate anxiety. 18,19 Anxiety-reducing effects of essential oils have been reported in several studies, especially lavender oils 20,21 and Melissa officinalis L. 22 Lavender is known as one of the most effective oils in reducing anxiety and belongs to the Lamiaceae family, with various species. The most commonly used lavender species is Lavandula angustifolia, and its key components, linalool and linalyl acetate, are known for their calming and sedative effects. 23 Melissa officinalis L. is a plant known as lemon balm. Among the main components of lemon balm essential oil, rosmarinic acid, ursolic acid, and oleanolic acid are known to increase the levels of gamma-aminobutyric acid, a neurotransmitter in the brain, reducing anxiety. 24
Upon reviewing existing meta-analyses, the authors discovered studies investigating the effects of inhalation therapy on anxiety in patients undergoing cardiac surgery, 25 as well as the effects of aromatherapy on anxiety in patients with various cardiovascular diseases, such as hypertension, coronary heart disease, and ACS. 12 However, no studies have focused on patients with ACS. Furthermore, these studies included nonrandomized controlled trials (nonRCTs), 12 indicating a lack of high-level evidence. In addition, owing to the lack of various types of essential oils and diverse application methods, 12,25 there is insufficient evidence to establish intervention strategies for reducing the anxiety of patients with ACS in clinical settings. Therefore, this study aimed to verify high-level evidence regarding the anxiety-reducing effects of aromatherapy, specifically in patients with ACS, by including only RCTs. In addition, it sought to provide objective evidence for effectively developing strategies to reduce anxiety in patients with ACS in clinical settings.
Methods
This review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses 2020 guidelines. 26 The study protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO protocol number: CRD42024511381).
Information sources and search strategies
To search for relevant articles, comprehensive searches were conducted using six databases: PubMed, CINAHL, Embase, Web of Science, Cochrane Library, and PsycINFO. The search strategy incorporated the Medical Subject Headings database, Emtree, free terms, and synonyms, using the Boolean logical operators “AND” and “OR” to complete the search equation for participants, interventions, and outcomes. The search strategy is provided in the Supplementary Table S1. Manual searches were conducted based on the reference lists of relevant previous studies, and a Google Scholar web search was performed, including gray literature. The search period was not restricted, and all articles published until February 21, 2024, were included.
Eligibility criteria
The specific inclusion criteria for this study were as follows: 1) participants: adults aged 18 years and older admitted to the hospital for the treatment of ACS; 2) interventions: studies that performed aromatherapy using aromatic essential oils; 3) comparisons: placebo, no intervention, and routine care; 4) outcome: anxiety (primary outcome) and blood pressure (secondary outcome); and 5) study design: RCTs.
The exclusion criteria were studies: 1) evaluating the effects of aromatherapy on transient anxiety before surgery or procedures such as coronary artery bypass graft (CABG), coronary angiography, intravenous catheterization, or chest tube removal; 2) without a control group; 3) combining aromatherapy with other interventions; and 4) lacking essential data required for meta-analysis.
Study selection and data extraction
Two reviewers independently conducted the database searches according to a predefined search strategy. The data were organized using the EndNote 20 reference software package (Clarivate Analytics, Philadelphia, PA, USA), and duplicate publications were excluded using the software’s functionality. Two reviewers (RWK and MK) initially screened titles and abstracts to select studies that met the inclusion criteria. For subsequent secondary screening, the full texts of the selected studies were reviewed and those that met the inclusion criteria were included in the final analysis. Disagreements between the reviewers were resolved by reviewing the full text and engaging in discussions until a consensus was reached.
After analyzing the characteristics of the included studies, a data extraction form was developed. Two researchers (RWK and MK) randomly selected three studies and independently extracted the data, which were discussed to refine the data extraction form. Each author extracted data according to the data extraction form, which included the following information: 1) author, publication year, country, study design, and characteristics of the included studies (setting, participants, sample size, mean age, and percentage of female participants); 2) intervention characteristics (route of administration, type of essential oil, total sessions, length, and duration); 3) instruments; and 4) control group. In cases of discrepancies during data extraction, a consensus was reached through discussion.
Risk of bias assessment
Cochrane’s Risk of Bias tool 2.0 (RoB2) for RCTs 27 was used to assess the risk of bias in the included studies. Two reviewers (RWK and MK) independently conducted the assessments. The following domains were evaluated and rated as “low,” “some concerns,” or “high” for their risk of bias: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result.
Synthesis and statistical analysis
The R package Meta version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria) was used for statistical analysis. As different tools were used to measure the effect size in each study, the standardized mean difference (SMD) was calculated to verify the mean difference between the two groups. Hedges’ g was calculated as the SMD to account for the tendency to overestimate the effect size in studies with small sample sizes. The statistical significance of the estimated effect size was presented with a 95% confidence interval (CI). Effect sizes were categorized as follows: small, 0.2 ≤ SMD < 0.5; moderate, 0.5 ≤ SMD < 0.8; and large, SMD ≥ 0.8. 28 Furthermore, considering the heterogeneity in sample sizes and intervention methods among the included studies, the analysis was conducted using the restricted maximum-likelihood estimator, along with the Hartung–Knapp correction. 29
The I 2 statistic, which represents the proportion of the total variance attributable to the real variance, was used to assess the heterogeneity of the effect sizes across studies. The interpretation of heterogeneity was as follows: 1) 0%–40%, might not be important; 2) 30%–60%, may represent moderate heterogeneity; 3) 50%–90%, may represent substantial heterogeneity; and 4) 75%–100%, considerable heterogeneity. 30 In the case of considerable heterogeneity, it is important to identify potential sources of heterogeneity to obtain more reliable results. Therefore, a moderator analysis was planned. The moderator analysis included categorical variables, such as route of administration, type of essential oil, length of intervention, and mean age, which were analyzed through subgroup analysis and meta-analysis of variance. Furthermore, continuous variables, such as intervention sessions and duration, were included and analyzed using meta-regression.
A funnel plot was used to evaluate publication bias by examining the presence of asymmetry. To complement this analysis, Egger’s regression test was used to verify the presence of small-study effects. Publication bias was detected, and the regression-adjustment method was used to perform an adjustment. Considering the potential for heterogeneity to distort the meta-analysis results, a sensitivity analysis was conducted to examine the consistency of the derived effect sizes. Initially, a Baujat plot was used to identify studies with substantial heterogeneity that could have influenced the overall effect size. The authors observed changes in the overall effect size after excluding studies with high heterogeneity.
Results
Study selection
A total of 440 articles were initially identified from six databases. After excluding the duplicates (115 articles), 325 articles remained. In the first screening phase, 308 articles were excluded based on the title and abstract, leaving 17 articles. During the second screening phase, a full-text assessment was conducted, resulting in the exclusion of seven articles due to improper participants (n = 4), nonRCTs (n = 1), combined interventions (n = 1), and improper outcomes (n = 1). Consequently, 10 articles were included in the analysis. In addition, 10 articles were identified through manual searching, with six articles excluded for improper participants (n = 3), improper outcomes (n = 1), and improper comparisons (n = 2). Therefore, four articles from the manual search were included in the analysis. In total, 14 articles 31 –43 from both database search (10 articles) and manual search (four articles) were included in the final analysis (Fig. 1).
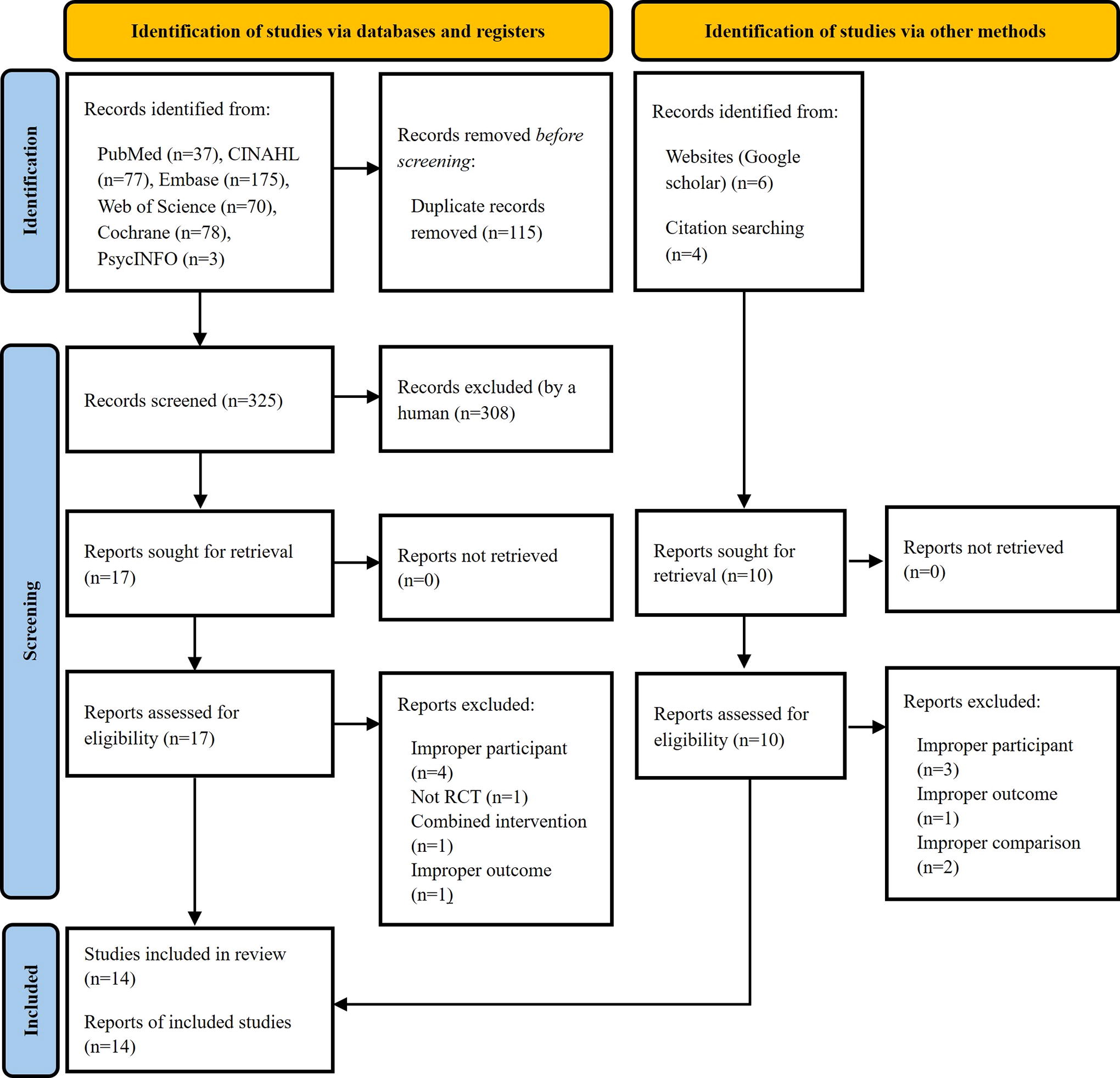
Flowchart summarizing the process of study selection.
Study characteristics
A total of 14 articles were analyzed, all published after 2014, and all 14 were from Iran. Most of the studies were conducted in CCU settings (10 articles), whereas one study each was conducted in the intensive care unit, emergency department, heart departments, and unspecified hospital department. All participants were diagnosed with ACS, with five studies specifically focusing on the diagnosis of myocardial infarction or acute myocardial infarction. The sample size ranged from 32 to 77 participants in both the experimental and control groups. The mean age ranged from 44.77 to 73.97 years in the experimental group and from 49.25 to 72.62 years in the control group. Age information was not provided in two of the studies. The proportion of female participants ranged from 27.3% to 100% in the experimental group and 16.7% to 100% in the control group (Table 1).
Characteristics Of The Included Studies
ACS, acute coronary syndrome; AMI, acute myocardial infarction; CCU, coronary care unit; ICU, intensive care unit; MI, myocardial infarction; NR, not recorded; RCT, randomized controlled trial; SD, standard deviation.
Characteristics of the interventions in the included studies
Upon examining the characteristics of the interventions, most studies used inhalation therapy (13 articles), whereas massage (one article) was rarely used. Regarding the specific type of intervention, most studies used a single essential oil (13 articles), with lavender essential oil being the most commonly used (five articles). The number of intervention sessions varied from one to nine, and the duration of a single session ranged from 69 sec to 12 h. The total intervention duration ranged from 1 to 3 days, with most studies (11 articles) lasting 2–3 days. The most commonly used measurement tool was the State-Trait Anxiety Inventory (12 articles), followed by the Hospital Anxiety and Depression Scale (two articles). Blood pressure was measured in some studies (five articles). In the control group, placebo was the most commonly provided intervention (nine articles), followed by routine care (five articles). Among the 14 studies, three studies reported that participants experienced no side effects, whereas the remaining 11 studies did not investigate the side effects experienced by the participants (Table 2).
Characteristics Of Interventions In The Included Studies
Length refers to the time per session.
Duration refers to the total number of weeks/days the intervention was provided.
BP, blood pressure; HADS, Hospital Anxiety and Depression Scale; NR, Not reported; SSAI, Spielberger’s State Anxiety Inventory; STAI, State-Trait Anxiety Inventory.
Risk of bias
The quality of the 14 RCTs was evaluated using the revised Cochrane RoB2 tool for RCTs (Fig. 2). In this evaluation, three articles were assessed as having “some concerns” in the first domain, which is the “randomization process.” This indicates that the allocation sequence was not adequately randomized and that there was insufficient information on whether the allocation sequence was concealed until the intervention was assigned.

Risk of bias summary according to the revised Cochrane risk-of-bias tool for randomized trials.
In “deviations from intended interventions,” appropriate analysis, such as intention-to-treat analysis, was not used to estimate the effects allocated to interventions, resulting in a “high risk” rating. In terms of the measurement of the outcome, it was rated as “some concerns” in five studies as they did not use placebos. The remaining two domains were judged to be “low risk.” Therefore, the overall risk assessment indicates that out of the 14 RCTs, six were assessed as “low risk” (42.9%), whereas the remaining seven RCTs were assessed as having “some concerns” (50.0%), and one RCT was assessed as having “high risk” (7.1%).
Effects of aromatherapy on anxiety
Primary outcome measures
A systematic review and meta-analysis were conducted on 14 RCTs that investigated the effects of aromatherapy on patients with ACS. Regarding self-rated anxiety measurement, the pooled overall effect of aromatherapy was −1.66 (95% CI: −2.47 to −0.85), indicating a large effect size. However, considerable heterogeneity was observed in the overall effect size (I 2 = 97.46%, p < 0.001) (Fig. 3).

Forest plot: effect of aromatherapy on self-rated anxiety levels. CI, confidence interval; SD, standard deviation; SMD, standardized mean difference. The minus signs before the means indicate decreased anxiety scores from the pretest to the posttest.
Secondary outcome measures
In the four RCTs investigating the physiological effects of aromatherapy on blood pressure, the pooled overall effect of aromatherapy on systolic blood pressure (SBP) was −0.65 (95% CI: −1.15 to −0.15), indicating significant effect. However, considerable heterogeneity was observed in the overall effect size (I 2 = 84.73%, p < 0.001). Similarly, for diastolic blood pressure (DBP), the SMD was −0.42 (95% CI: −0.92 to 0.08), suggesting no significant effect (Fig. 4A, 4B).
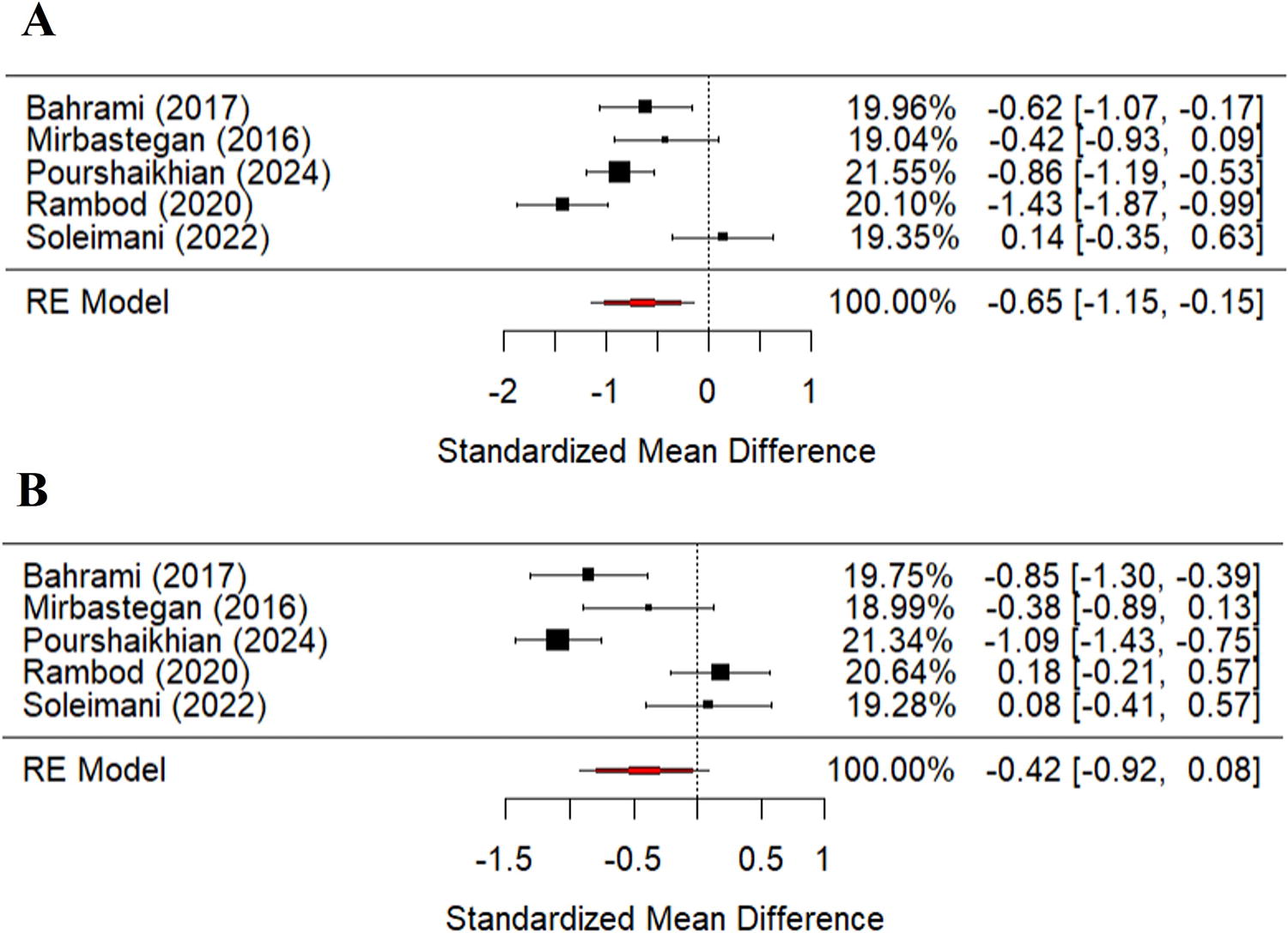
Forest plots: effect of aromatherapy on blood pressure.
Moderator analysis
To explore the potential sources of heterogeneity, analyses were performed by classifying the data into categorical and continuous variables. Subgroup analyses were conducted to assess preselected categorical variables, including route of administration, type of essential oil, and mean age (Table 3). Regarding the route of administration, inhalation showed a large effect size with an SMD of −1.70 (95% CI: −2.33 to −1.08), whereas massage indicated no significant effect, and there was no significant difference between the two groups (p = 0.398). For the type of essential oil, single oils (rose, Melissa officinalis, Citrus aurantium, lemon, geranium, and peppermint) exhibited the largest effect size (SMD = −2.08, 95% CI: −2.28 to −1.29). In contrast, lavender essential oil showed no significant effect, with an SMD of −0.94 (95% CI: −1.91 to 0.04). The blended oils also demonstrated no significant effect and no significant difference between the groups (p = 0.211). Regarding mean age, the largest effect size was observed in the 40s (SMD = −5.03, 95% CI: −6.27 to −3.80), with a decrease in the anxiety-reducing effect as age increased to the 50s and 60s. The meta-analysis of variance revealed a significant difference between the groups (p < 0.001), indicating a potential source of heterogeneity. In addition, meta-regression analysis indicated that the mean age explained 49.7% of the heterogeneity in the mean effect size (QM = 35.73, df = 3, p < 0.001).
Moderator Analysis On The Effect On Anxiety
CI, confidence interval; df, degrees of freedom; Qb, between-group; QM, Q moderator.
A meta-regression analysis was conducted for continuous variables, such as the number of sessions and duration of intervention. The results indicated that none of these variables were significant moderators (Table 3).
Publication bias
To examine publication bias, the authors visually inspected the asymmetry using a funnel plot. The results revealed a visually empty region in the bottom right corner, indicating asymmetry (Fig. 5A). In addition, Egger’s regression test showed significant evidence of publication bias (t = −5.866, p < 0.001). The authors assessed the impact of publication bias on the study findings using the regression-adjustment method to make adjustments (Fig. 5B). Consequently, the mean effect size decreased from −1.66 (95% CI: −2.47 to −0.85) to −1.65 (95% CI: −2.46 to −0.85). The results of this study provide evidence of a large effect size, demonstrating credibility despite a slight decrease in the effect size after bias correction.
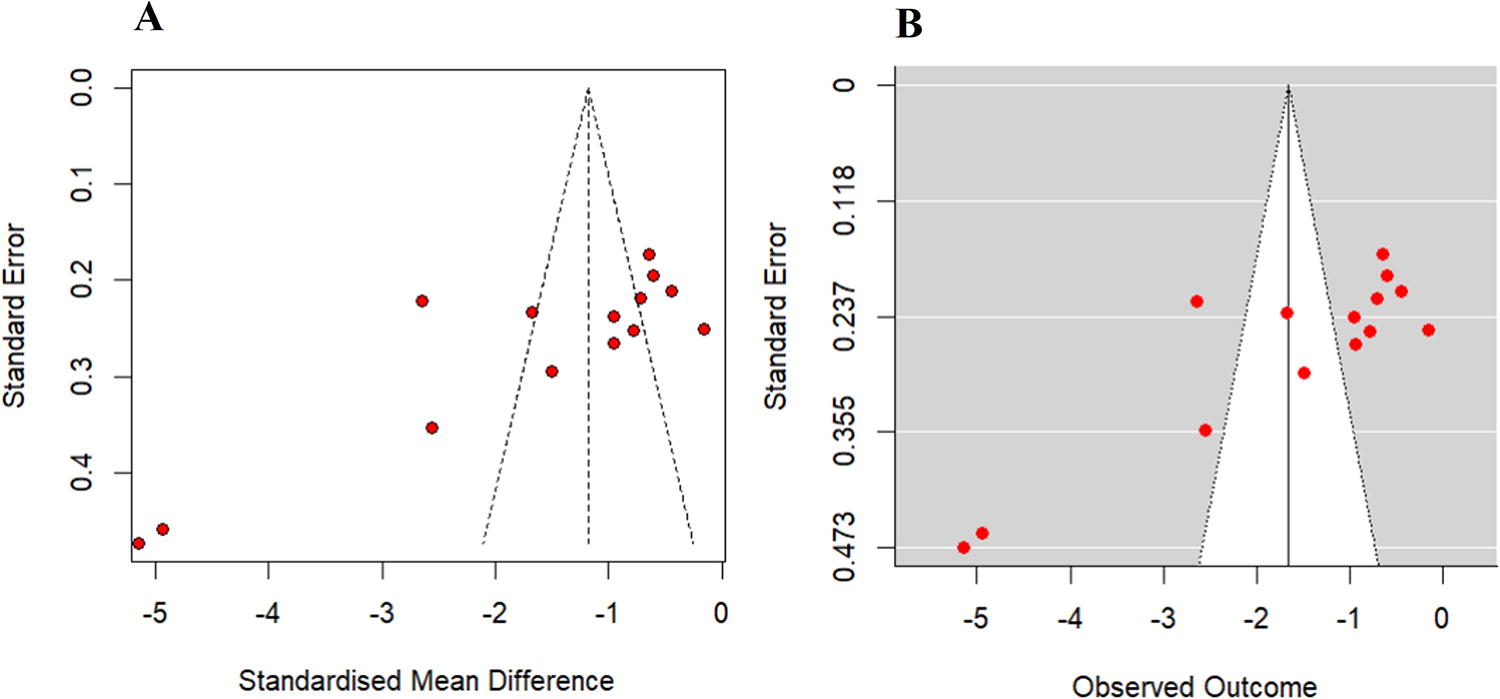
Publication bias.
Sensitivity analysis
Using a Baujat plot (Supplementary Fig. S1-A), the authors identified the studies that greatly influence on the overall effect size. The studies by Pourshaikhian et al., 44 Shirzadegan et al., 41 and Shirzadegan et al. 40 were found to have the greatest impact. When the study by Pourshaikhian et al. 44 was excluded, the SMD decreased to −1.58. Excluding the study by Shirzadegan et al. 41 resulted in a decrease in the SMD to −1.41. Similarly, when the study by Shirzadegan et al. 40 was excluded, the SMD decreased to −1.40 (Supplementary Fig. S1-B). However, as these differences were not substantially different from the overall mean effect size, the authors concluded that the effect of aromatherapy on anxiety in patients admitted to hospitals for ACS is credible.
Discussion
Interpretation of results and comparison with previous studies
This study analyzed the effects of aromatherapy on anxiety in patients with ACS by including 13 RCTs. First, in self-reported measures, aromatherapy showed a large effect size in reducing anxiety. However, no significant effects on blood pressure were observed during the evaluation of physiological effects. In addition, inhalation showed a large effect size, whereas massage did not show a significant effect. Furthermore, different types of essential oils, such as rose, Melissa officinalis, Citrus aurantium, lemon, geranium, and peppermint, demonstrated a large effect size, whereas lavender essential oil and blended oil showed no significant effects. Moreover, the study found that the greatest effect size was observed in individuals in their 40s, and as age increased, the reduction in anxiety effects diminished.
First, aromatherapy had a large effect size in reducing anxiety in patients with ACS. This finding is consistent with a previous study 12 examining the effects of aromatherapy on anxiety in patients with various cardiovascular diseases, including hypertension, coronary heart disease, and ACS, which reported a large effect size. In addition, a study conducted on patients undergoing cardiac surgery, although not specifically on patients with ACS, showed a significant reduction in anxiety with aromatherapy inhalation therapy. 25 However, it is important to note that their study specifically focused on patients with ACS and included only RCTs to assess the effects of aromatherapy on anxiety. In contrast, previous studies targeted surgical patients and a broader range of patients with cardiovascular diseases, including both RCTs and nonRCTs. 12,25
In terms of the type of administration, inhalation showed a large effect size, whereas massage did not show a significant effect. This finding is consistent with a study conducted in patients undergoing cardiac surgery, although not specifically in patients with ACS, that demonstrated the effectiveness of inhalation therapy. 25 Patients with ACS are often in emergency situations, and most, as in this study, are admitted to the CCU. Therefore, inhalation, which allows for more convenient access, may be more beneficial than massage. However, in a previous study analyzing the effects of lavender massage therapy on anxiety reduction, although not specifically in patients with ACS, a moderate effect size was observed. 45 Therefore, massage may have an anxiety-reducing effect on patients with ACS. Because there was only one study related to the massage method in this study, to further demonstrate the anxiety-reducing effect of massage in patients with ACS, it is necessary to conduct future research specifically focusing on massage and repeat the meta-analysis.
Regarding the essential oil type, single oils, such as rose, Melissa officinalis, Citrus aurantium, lemon, geranium, and peppermint, showed large effect sizes in anxiety reduction. However, because of the limited number of studies available on each oil, it was impossible to determine the specific effects of each oil. In contrast, lavender, which is widely used for anxiety reduction, did not affect anxiety reduction in patients with ACS. Lavender is known to reduce anxiety by secreting substances such as encephalin, endorphins, and serotonin. 46 Moreover, lavender has been reported to have anxiety-reducing effects in various populations, 20,21,45 including among patients with various cardiovascular diseases. 12 However, this study provides evidence that offering a different single oil may be more beneficial for anxiety reduction in patients with ACS than using lavender oil. In addition, research on the use of blended oils to reduce anxiety in patients with ACS is limited to one study, which is insufficient to validate their effectiveness. Blended oils have the potential to maximize their efficacy through synergistic effects; 47 thus, further research in this area is needed. Future meta-analyses should be conducted to explore these aspects further.
In a subgroup analysis conducted by grouping participants according to their mean age, the largest effect size was observed in the 40s age group and the anxiety reduction effect decreased as age increased. Essential oils can be absorbed into the body through the skin or the olfactory system, 48 and it can be assumed that aging may affect these processes. However, it is difficult to find clear evidence that the effectiveness of aromatherapy decreases with age. Further research is needed to explore the relationship between age and the effects of aromatherapy. In this study, a significant anxiety reduction was observed in the 40s age group, which should be considered when implementing interventions for anxiety reduction in patients with ACS.
The authors investigated the physiological effects of aromatherapy on anxiety in patients with ACS by examining its effects on blood pressure. Aromatherapy exhibited a moderate effect size on SBP, but there was no significant decrease in DBP. This result is similar to a study that specifically analyzed the effects of lavender oil on blood pressure in a population with various conditions, 21 where a small effect size was observed for SBP, whereas DBP showed no significant effects. However, the results of their review slightly differ as they demonstrated a moderate effect size in reducing SBP specifically in participants with ACS. While the previous study 21 focused only on the effects of lavender oil in all participants, their review examined the overall effects of aromatherapy on blood pressure, including various oils, specifically in patients with ACS. The findings of their review are inconsistent with a study that solely applied inhalation to patients undergoing cardiac surgery, 25 which showed no effects on SBP and DBP. The previous study targeted individuals undergoing cardiac surgery, 25 whereas this review focused specifically on those with ACS. In addition, the former study 25 solely included the inhalation method, indicating a discrepancy between the current review results and theirs. These findings indicated that the reduction in blood pressure may vary depending on the type of oils, population, and method of interventions being studied. In this review, a lack of studies was included in the analysis of blood pressure. In addition, despite the high heterogeneity observed, the limited number of studies made it difficult to identify the underlying causes of this heterogeneity. Therefore, in the future, conducting meta-analyses with additional studies could establish more definitive evidence regarding the effects of aromatherapy on blood pressure reduction.
Strengths and limitations
This study provided significant evidence for the large effect size of aromatherapy in reducing anxiety among patients with ACS, thus establishing a basis for its application in future ACS patient care. Furthermore, previous meta-analyses have analyzed the effects of aromatherapy on anxiety in patients with various cardiovascular diseases, such as CABG, hypertension, coronary heart disease, and ACS; however, no studies have specifically examined the effects of aromatherapy on anxiety in patients with ACS. One strength of this study was that it provided reliable results on the anxiety-reducing effects of aromatherapy in patients with ACS by including only RCTs. Finally, the study analyzed not only subjective self-reported measures but also the effects of aromatherapy on objective physiological indicators, such as blood pressure, which further adds to its significance.
This study had some limitations. First, although aromatherapy showed a significant effect size in reducing anxiety through inhalation therapy, it did not show an effect with massage therapy. However, the limited number of studies related to massage may have affected the accuracy of these results. Second, although efforts were made to include studies conducted in various countries, only studies conducted in Iran were ultimately included, which may limit the generalizability of the findings. Administration of essential oils has over 3000 years of history in Iran, and health care practitioners widely use it in clinical settings based on traditional knowledge. 49 The participants in this study were patients with acute ACS. Because aromatherapy is not commonly practiced in hospitals for such cases, the research appears to have been predominantly conducted in Iran. Thus, there is a need for future studies to be conducted in more diverse countries for broader clinical insights. Third, despite efforts to include gray literature or studies published in languages other than English, there were limitations in not being able to incorporate such studies into the analysis. Fourth, the research findings underscore the recognition that aromatherapy may be beneficial in alleviating acute anxiety states in specific contexts. However, its application is limited to a narrow range of situations. It is important to acknowledge that there are limitations to its broad application for anxiety disorders or long-term anxiety. Fifth, there was no statistically significant effect on DBP, which could be attributed to the limited number of included studies. Therefore, in future aromatherapy research, it is essential to measure not only subjective self-reported outcomes but also objective indicators such as blood pressure to enhance the validity of research findings. Finally, this study attempted to confirm the intervention effects of aromatherapy options for patients with ACS, considering factors such as the type of essential oil and route of administration. However, due to the limited number of included RCTs, there are limitations in objectifying the results, thus necessitating further research in the future.
Conclusion
This study demonstrated the significant effect of aromatherapy in reducing anxiety in patients with ACS. The inhalation method showed a stronger effect than the other methods, and individual oils, rather than the commonly used lavender essential oil, effectively reduced anxiety. In addition, this study found that the greatest reduction in anxiety occurred in the 40s age group. Furthermore, although aromatherapy decreased SBP, there was no effect on DBP. Considering these findings, developing a program for applying aromatherapy in clinical settings to reduce anxiety among patients with ACS while taking these factors into account could lead to more effective intervention strategies.
Footnotes
Authors’ Contributions
Ri Whaol Kim: Data curation, Software, Validation, and Writing—Reviewing and Editing. Myoungsuk Kim: Conceptualization, Methodology, Data curation, Formal analysis, Writing—Original draft preparation, Visualization, Investigation, and Supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Data Availability Statement
The study data are available upon reasonable request from the corresponding author.
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.