
Abstract
Introduction:
Acupuncture’s role in surgical and postoperative contexts is gaining traction. However, the evidence remains patchy and is often of low-grade quality, particularly in the context of postintestinal surgery.
Purpose:
To assess acupuncture’s efficacy in pain relief and functional recovery after abdominal surgery.
Methods:
We searched PubMed, Cochrane, Web of Science, and Google Scholar for randomized trials using manual acupuncture as the main intervention. Outcomes included postoperative pain, analgesic use, nausea, gastrointestinal (GI) regeneration, and length of hospital stay. For risk of bias assessment Cochrane risk of bias tool 2 was employed. Registered with PROSPERO: CRD42022311718.
Results:
Of 700 records till May 2023, 8 trials (551 patients; 16–200/trial) were included. Due to factors such as varying experimental settings and unpublished protocols, there was high risk of bias and heterogeneity, making meta-analysis unfeasible. Safety data were documented sufficiently by two trials. However, acupuncture showed marked benefits in pain relief, less analgesic use, fewer nausea cases, and improved GI recovery. One study reported reduced hospitalization time.
Conclusion:
Due to the varied methodologies and potential biases in existing studies, the definitive effectiveness of acupuncture remains unclear. To confirm the potential benefits of acupuncture as suggested by the reviewed studies, it’s imperative to have more standardized study protocols, well-defined interventions and controls, and objective measures of efficacy.
Introduction
As the application of manual acupuncture in surgical contexts gains momentum, 1 –4 the scientific community remains divided on its efficacy. 5,6 The traditional medical community is increasingly recognizing acupuncture, with two-thirds of all guidelines discussing acupuncture interventions. However, these guidelines often fall short in their utility due to vague identification of target populations, insufficient details about acupuncture procedures, omission of alternative treatment options, neglect of critical patient outcomes, failure to consider patient values and preferences, and overlooking a significant portion of existing acupuncture research. 7 In 1999, the World Health Organization released guidelines on basic training and safety in acupuncture. 8 This document outlined the training programs deemed suitable for acupuncture practitioners by professional experts and health regulators. Yet, there remains an absence of standardized acupuncture treatment protocols for consistent comparison and evaluation.
Abdominal surgery often poses postoperative challenges to both patients and medical practitioners. One of the primary concerns following this surgery is ensuring an effective recovery process, which encompasses not only pain relief but also the re-establishment of gastrointestinal (GI) function. 9 Beyond mere pain relief, effective management of postoperative pain has cascading benefits. Alleviating pain can not only reduce the psychological distress, such as anxiety, experienced by patients but can also decrease their dependence on opioids. This, in turn, mitigates opioid-associated side effects, expediting the recovery process and potentially shortening hospital stays. 4,10
In light of these challenges, our review is driven by a quest: Are there systematic, or even standardized, acupuncture strategies that can effectively address these postoperative complaints? By delving into this question, we aim to highlight the current state of evidence and offer directions for future research in this intriguing intersection of traditional and modern medicine.
Methods
The systematic review protocol has been registered on PROSPERO’s website (International Prospective Register of Systematic Reviews) and is openly accessible by registration no. CRD42022311718.
Eligibility criteria
Randomized controlled trials (RCTs) addressing postoperative pain and GI malfunction by manual acupuncture as the main verum intervention were eligible. Manual acupuncture is defined as puncturing the skin with press (permanent) or filiform (classical) acupuncture needles. To obtain De-Qi, the insertion is followed by lifting, thrusting and or rotation of the needle, performed by hand. 11 De-Qi may be translated as “needling sensation,” which is commonly characterized as a sore, numb, full or heavy sensation. 12,13 A connection of De-Qi to clinical efficacy of acupuncture is frequently assumed, but overall controversial. 13 –15 In this review, studies with mixed forms of acupoint stimulation such as additional electrostimulation, moxibustion, massage, or others were excluded to homogenize the assessment and comparison. As control group, standard care, sham acupuncture or any other treatment in direct comparison, such as electroacupuncture, were included. Studies accessible in English and German language for full text were included whereas articles in Chinese language were not, for pragmatic reasons. Trial participants had to be adults receiving abdominal surgery, without any restrictions on gender or ethnicity.
The clinical outcome was assessed by the numeric rating scale (NRS) or visual analog scale (VAS) for pain, postoperative nausea and vomiting (PONV) were graded by quantity and timing, or by intensity on VAS. Flatus, peristalsis and defecation were assessed by hours of first occurrence after surgery, analgesics in milligrams and number of demands for analgesics. Although the chosen MESH-terms and synonyms for “postoperative” already included any possible postoperative regimen, we added Enhanced recovery after surgery (ERAS®) into the search terms, to emphasize our intention to assess the current data on an acupuncture treatment in an up-to-date setting, where enhanced recovery pathways are evidence-based best practice. The first ERAS®-protocol was published in 2005, 16 certainly precluding earlier research. However, prequels can be found in fast-track surgery strategies from the late 1990s, paving the way to a multimodal optimization of perioperative care. 17,18 Accordingly, an adherence to any guidelines such as ERAS® was not part of the inclusion criteria.
Search strategy
PubMed, Cochrane Central Register of Controlled Trials, Web of Science Core Collection, and Google Scholar were selected as databases and have been searched from their inception until May 22, 2023. The individual search strategies were created by consulting a second, independent professional literature search specialist and are provided within the Supplementary Data S2 (strategy for PubMed in Table 1). Google Scholar hits were limited to the first 100 as the search string can only consist of 250 characters. 19 Although only RCTs were eligible for inclusion, we decided to add terms for nonrandomized studies to increase sensitivity because primary hits were fewer than 1000. 20 EndNote (Version 20.5) was used to import hits and remove duplicates. Then titles and abstracts were screened to sort by eligibility criteria. In addition, we searched reference and citation lists of core articles and systematic reviews and included trials from database searching, using Web of Science Core Collection (Fig. 1). The entire screening process was done by two authors independently (S.S. and E.G.) and compared at every stage. When discordance occurred, it was resolved by consensus discussion.
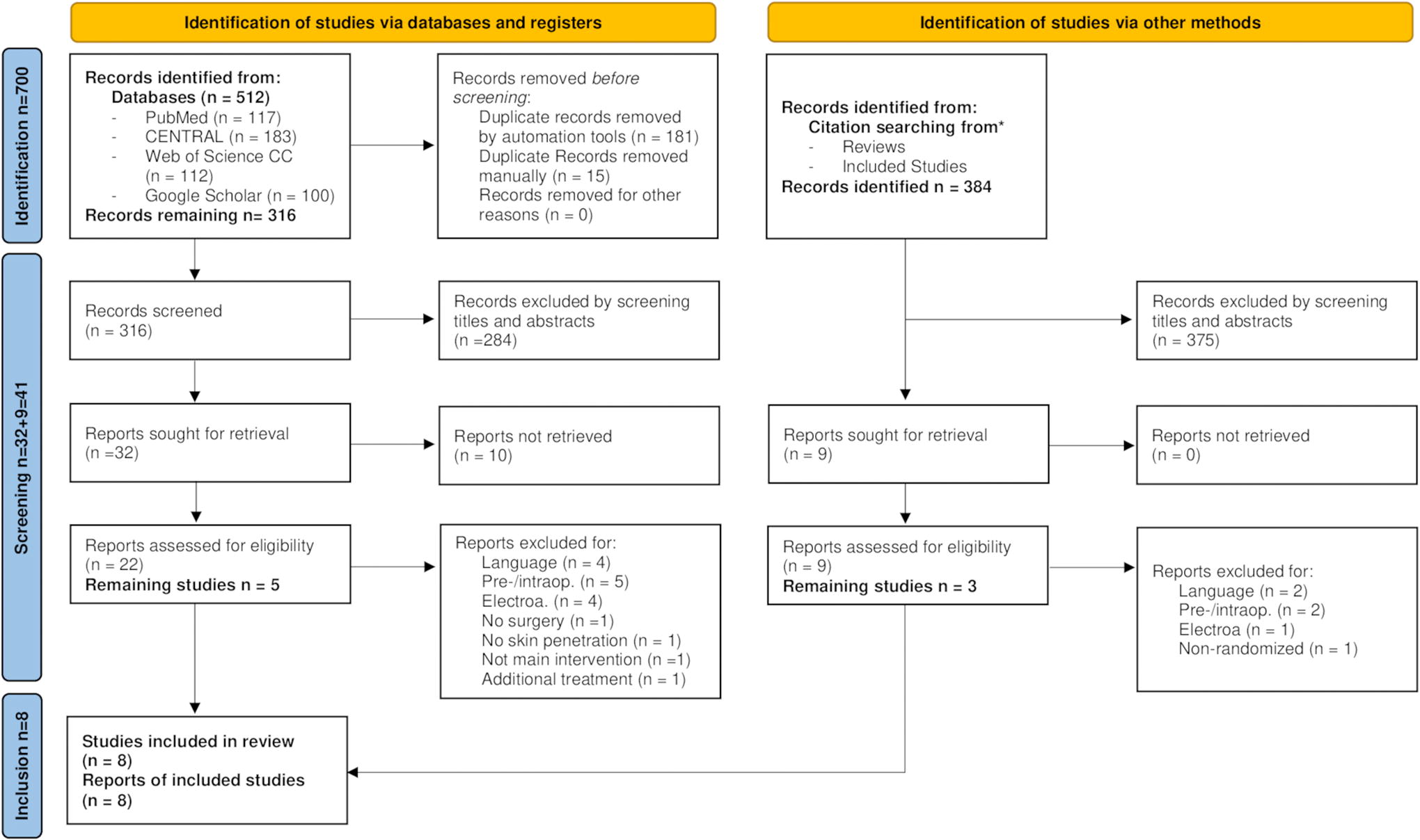
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources. 21 *Citation and reference search via Web of Science Core Collection (37/38 reviews and 7/8 studies listed, keywords “acupuncture” and “postoperative” had to be mentioned). Preop, preoperative (before anesthesia); intraop, intraoperative (between anesthesia induction and emergence); electroa, electric stimulation (no manual acupuncture group); no surgery, no directly surgery-related patient group; no skin penetration, noninvasive acupoint stimulation; not main intervention, Acupuncture group not reported on most outcomes; additional treatment, acupuncture group also received acupressure.
Full Electronic Search Strategy as Used in PubMed
Similar search strings have been used for Cochrane Central Register of Controlled Trials, Web of Science Core Collection, and Google Scholar, adjusted to their connotation rules.
Data collection and analysis
The systematic review was built in accordance with the PRISMA (Preferred reporting items for systematic reviews and meta-analyses) guidelines for acupuncture (compare Supplementary Data S1). 22 The following parameters have been chosen for data extraction following the TIDieR-checklist (template for intervention description and replication): 23 author, year of publication, type of surgery, population size, intervention characteristics (execution and frequency of acupuncture), control group therapy, outcome measures and relevant numeric data of the included studies.
The quality of reporting was evaluated according to the Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guidelines. 24 Additionally, reporting of safety data was examined. An evaluation of heterogeneity across the studies was built upon Cochrane’s review on Heterogeneity and subgroup analyses. 25 To assess for risk of bias, a certified manual by Springer Medizin and Cochrane’s Risk of Bias Tool 2 was applied. 26,27 By applying the Grading of Recommendations Assessment, Development and Evaluation (GRADE) criteria, the quality of evidence has been analyzed for each outcome, rating risk of bias, consistency, directness, precision and publication bias across all studies reporting on the chosen outcome. Therefore, high-quality evidence, based on an RCT design, was downgraded by one level when detecting serious limitations. 28 Outcomes to be assessed were pain, administered analgesics, GI recovery, PONV, length of hospital stay (LOS), and fast-track-surgery compliance characteristics.
Results
Study selection
Identification and screening
After duplicate removal, we identified n = 700 articles for further assessment. The articles were identified via databases (n = 316), and via citation searching (n = 384). By screening titles and abstracts, we excluded n = 659. For further details see Figure 1. 28
Inclusion
According to our selection criteria every study included had to address the symptoms after abdominal surgery with manual acupuncture (intervention group), and control interventions should at least comprise best medical care without administering acupuncture (Table 2).
Summary Characteristics Following TIDieR-Checklist 23
P-scores as accurately as published.
Primary small local hospital or outpatient clinic, secondary large hospital, tertiary University hospital.
Main end point plasma leucine enkephalin not included due to incomparability to all other studies.
Main end point gastroparesis cure rate not included due to incomparability.
MIC, minimal invasive surgery; po, postoperative; POD, postoperative day; h, hours; NRS, numeric rating scale; PACU, postanesthesia care unit; EEN, early enteral nutrition; A, acupuncture; C, control; ER, effect rate; LOS, length of hospital stay.
We identified n = 41 studies to seek for full text reports, n = 10 of them being unretrievable, we found n = 8 with overall 551 patients eligible for inclusion (Fig. 1, Table 2).
The reasons for exclusion were as follows: n = 6 were excluded for not being accessible in English or German (n = 1 Turkish, n = 5 Chinese), n = 7 applied acupuncture before or during surgery, n = 5 gave electrical stimulation only mentioned in the full text, one was not surgery-related, one used a noninvasive acupoint stimulation, one used manual acupuncture not as the main verum intervention and did not quantify most outcomes of acupuncture patients, one did not randomize patients into intervention and control groups, and in one study acupressure was performed additionally to acupuncture. Details and identification sources breakdown are shown in Figure 1.
First figure
Documentation of general characteristics of the studies revealed high heterogeneity
The six studies included revealed tremendous formal differences regarding design, controls, number of participants and the surgeries involved. The following characteristics of the studies are summarized in detail in Table 2.
In the first study, Li et al. 29 compared four lines of treatment (acupuncture, Chinese herbs, metoclopramide and placebo) in 16 hepatectomy for primary liver cancer patients using crossover design. As additional outcome they assessed plasma leucine enkephalin. By definition, such assessment was not a key parameter of our review and solely used in this study. Auricular acupuncture points of Heart, Lung and Shenmen were used; a stimulation of any kind was not stated. 29
In the second study, Grube et al. 30 included n = 66 patients receiving laparoscopic cholecystectomy or vaginal hysterectomy, comparing treatment with acupuncture, metamizole, and standard care in a parallel study design. Acupoints LI-4, LI-11, PC-6, ST-36, ST-44, SP-6, LR-3 were punctured bilaterally without stimulation. 30
In the third study by Wu et al., 31 only gynecological operations (caesarean) were included, treating n = 60 patients in post anesthesia care unit with manual acupuncture, electroacupuncture or standard care in a parallel study design. SP-6 was stimulated bilaterally until De-Qi sensation. 31
In the fourth study by Sun et al., 32 (n = 63) abdominal surgery patients without specification and unknown invasiveness were either acupunctured or administered metoclopramide. As the main end point gastroparesis was assessed by a procedure involving a gastric tube, that was not included. Their main acupoints were CV-12, ST-36, PC-6, and SP-6, which were stimulated each with individual methods (reducing, reinforcing, and supplementing). 32
In the fifth study by Kou et al. 33 parallel study design for acupuncture versus standard care in n = 40 open cholecystectomy patients was used. As an additional key parameter, they assessed GI recovery using a ranking system by defecation, bowel sounds, abdominal distension, body temperature, and PONV. For acupuncture treatment they applied ST-36, ST-37, ST-39, and GB-34 bilaterally with even “reinforcing-reducing technique.” 33
In the sixth study, Yuan et al. 34 randomized n = 200 laparoscopic cholecystectomy patients to one of four treatment groups applying parallel study design: acupuncture and standard care, acupuncture and early enteral nutrition (EEN), EEN, standard care only. The three acupoints ST-36, ST-37, and ST-39 were punctured and stimulated to attain De-Qi. 34
In the seventh study by Guo et al., 35 n = 64 patients receiving laparoscopic or open elective GI tumor resection were included. Using parallel study design, patients were either acupunctured by intradermal needle therapy 1 , 37 or administered adhesive tapes at the same locations. As presented, INT is performed correctly without pain deriving from puncturing the skin. Subsequently, patients were blinded to their group assignment. All patients in acupuncture and control group underwent ERAS protocol including preoperative education and nutritional care, perioperative anesthesia optimization, selective tube placement, normothermia maintenance and postoperative multimodal analgesia, PONV prevention, smart tube management, nutritional care, early oral feeding, and early mobilization. Acupuncture was performed bilaterally on LI-4, PC-6, LR-3, SP-4, ST-36, ST-37, and ST-39 with press needles, manual pressure was applied every 4 to 6 h until the patient felt a soreness, numbness, and/or pain. 35
In the eighth study, Wang et al. 36 randomized n = 42 patients after laparoscopic cholecystectomy into two groups. In parallel study design, patients either received acupuncture or were injected with Parecoxib Sodium. The acupoints LI-4, TE-5, GB-34, and GB-41 were punctured bilaterally and manipulated until De-qi was obtained. 36
The obvious heterogeneity of the studies is reflected by the differences in study designs (crossover, parallel, and number of study participants). Following inclusion criteria, a study using ear acupuncture was admitted, but none applying electroacupuncture, as is in many. Also, widely varying operations such as hepatectomy, caesarian section, open and laparoscopic cholecystectomy, GI tumor resection, or even unspecified abdominal surgery were considered and highly inhomogeneous. Considering acupuncture methods, eight acupoints have been used throughout several studies: LI-4, PC-6, ST-36, SP-6, LR-3, ST-37, ST-39, and GB-34. Still, verum treatment show vast differences: one to seven points were punctured one to seven times with varying duration, frequency, needles as well as stimulation technique applied. Further, controls varied greatly, as different treatments were used: for example, electroacupuncture, specific medication and standard care. Blinding of patients and therefore patient unconsciousness of verum or control group allocation was achieved only by Gou et al. 35 For the seven remaining studies, patients were aware of their assigned treatment, since comparing groups clearly differed in methodology. According to Cochrane’s review on heterogeneity and subgroup analyses, 25 all criteria of high heterogeneity (methodological, clinical, and statistical) are given. As this makes all studies relatively incomparable, a statistical meta-analysis was not performed.
Low to high quality of reporting in acupuncture studies (STRICTA guidelines)
There is no generally accepted score of the quality of acupuncture studies. However, there is a widespread set of criteria of quality of reporting called STRICTA guidelines, first published in 2001. 24 Meeting of the 2010 revised criteria is summarized in Table 3 below. Only two studies 30,36 seemed to fulfill these by providing 15 out of 17 criteria. Among these, Wang et al. stated reporting in conformation to STRICTA, but disregarded setting and context of treatment and rationale for comparator treatment. 36 By most authors, detailed description of acupuncture points (uni-/bilateral), information passed to patients, as well as training and experience of practitioners was documented scarcely or not at all. 30
Number of STRICTA Guidelines Met in Individual Studies and Main Shortcomings 24
As indicated, STRICTA criteria as used in this review were issued in 2010. Four trials being published beforehand, the authors would not have been able to align with the guidelines. Still, high-quality research requires a detailed statement of methods to allow transparency and reproduction, regardless of its topic.
Documentation of safety data
Two out of nine studies reported on (serious) adverse events [(S)AE] in detail. 34,36 One mentioned documentation but did not give details. 29 The remaining five reported on side effects as part of their outcomes only and did not address other (S)AE during or after acupuncture. 30 –33,35
Main results and quality of evidence
Four of the eight trials, including 186 patients, reported on postoperative pain, presenting their results on VAS or NRS decimal scales. 29 –31,36 Comparing with pre-intervention, one study showed greater effects in pain reduction for all timepoints of measurement after acupuncture, between groups (p = 0.004). 30 One study observed increased pain reduction until 2 h after acupuncture, between groups (p < 0.05 at 0.5, 1, 1.5, and 2 h postoperatively). 31 The latest study presented significantly higher pain reduction for acupuncture patients at 6–9 h after surgery (p = 0.002; p = 0.008); at 12 h both groups had similar VAS reduction scores. 36 A fourth trial could not ascertain differences in relief of pain at any time point in between groups. 29 Quality of evidence for the outcome pain was assessed as “low,” downgrading the evidence level for serious study limitations such as high risk of bias (see section 3.5 and Table 4), clinical and methodological heterogeneity (see section 3.2 and Table 2). Also, some indirectness was detected due to crossover design in one study, 29 as well as imprecision, as exact NRS-respectively VAS-scores were not given by two studies.
Risk of Bias. Cochrane’s RoB 2: Revised Tool for Assessing Risk of Bias in Randomized Trials Used 27
For the key outcome of required analgesics three out of four reporting trials, including 184 patients, distinguished a significantly lower demand of analgesics for patients receiving acupuncture, p = 0.01; 30 p < 0.05; 30,31 p < 0.02. 36 The quality of evidence was judged “moderate,” due to serious study limitations (see section 3.5 and Table 4) and some indirectness, whereas no serious inconsistencies and precision of evidence have been detected and publication bias being improbable.
GI regeneration was assessed using a multitude of parameters in four studies, including 320 patients: Peristalsis, first flatus, first defecation, and first oral feeding. All four reporting trials discovered an earlier onset of GI-recovery events for acupuncture groups compared with control groups, p < 0.05; 29 p = 0.006; 33 p < 0.01; 34 p < 0.001. 35 Li et al. 29 stated no significant difference only for time to first flatus (p > 0.05), Kou et al. 33 presented p > 0.05 for defecation; however, when combining the criteria of GI function in a grading system, the acupuncture group showed superiority (p = 0.006) compared with the standard care group. Grading the quality of evidence at “high,” the endpoint “GI recovery” reached the highest level assessed. Serious limitations due to high risk of bias (see section 3.5 and Table 4) led to downgrading by one point. Directness, precision and undetected publication bias combined with high effect size, due to unambiguity and a high number of patients being assessed for the outcome, led to upgrading by one point.
Five trials reported on symptoms of PONV, including 295 patients, four of which presented a significantly lower prevalence of PONV in the acupuncture group (p = 0.001; 30,35 p = 0.004; 36 p < 0.05 for therapeutic frequency 30,32 ). Guo et al. 35 stated similar scores for vomiting in acupuncture and control patients (p > 0.05); 35 Wang et al. 36 found similar PONV scores after acupuncture only at 12 h postoperatively in between groups. Wu et al. 31 stated no significant difference between the intervention and control group. 31 Serious study limitations in risk of bias, diverging results, imprecision, but directness and undetected publication bias led us to classify the quality of evidence for “PONV-symptoms” as “low.”
One study monitored LOS, including 200 patients, and noted a significantly shorter period in patients treated with acupuncture (7.14 ± 0.90 resp. 5.36 ± 0.69 vs. 8.34 ± 0.85 days, p < 0.05, Table 3). 34 Level of evidence for this outcome was determined to be “moderate” for consistency, directness, precision, and no publication bias. Tracing serious study limitations in risk of bias led to downgrading the evidence.
Implementation of fast-track or ERAS® items and its effects has been shown by Yuan et al.: 34 two groups received EEN, one of which was additionally treated with acupuncture, comparing with a third group receiving just acupuncture and a fourth on an overall conventional regimen. For the outcomes first flatus as well as average postoperative hospitalization days, the AE-group (acupuncture plus EEN) presented the shortest average time periods, reporting a significance in comparison with every other group. First flatus was reported on average at 21.6 ± 4.5 versus 52.6 ± 7.2 h (standard care group) postoperatively, p < 0.01. Mean LOS was at 5.36 ± 0.69 versus 8.34 ± 0.85 days (standard care group) significantly shorter, p < 0.05. 34 While only one fast-track element was adopted, Yuan et al. did not track compliance. Guo et al. 35 conducted their study in a surgery department adopting ERAS® protocol. Both acupuncture and control group received 13 pre-, peri- and postoperative ERAS® components as elaborated in subitem 3.2. Within the study, ERAS® compliance was documented: The compliance rates of four elements ranged within 71.9 and 84.4%, including preoperative optimization, postoperative tube management, postoperative early oral intake, and early mobilization. The remaining nine elements were adhered to at least 85% of the time. 35
Risk of bias
Seven of the reported eight trials came to an overall high risk of bias, as for each study, one domain or more was judged to be at a high risk of bias 29 –34,36 (Table 4). Solely Guo et al. 35 was assessed to raising some concerns overall, three domains evoking low risk of bias. In general, the greatest part of risk of bias criteria were evaluated at “some concerns” because methods were not stated clearly (see also Table 2). Three trials have been classified for low risk of bias in random sequence generation, as well as in allocation concealment (D1) . 34 –36 While Yuan et al. were fully transparent in deviations from intended intervention and analysis protocol, four studies were assessed at high risk of bias for effects of assignment to intervention (D2): Grube et al. excluded 12% of randomized patients, 30 the other three were unclear in randomization and analysis protocol. 31 –33 Seven trials were rated low for risk of attrition bias (D3). 31,33,34 The effect of intervention assignment on outcomes by blinding of study participants and personnel (D4) was not counterpoised in six studies 30 –34 due to inadequate control treatment. Regardless of one published study protocol by Wang et al., 36 risk of reporting bias (D5) raised some concerns for every trial. 29 –36 There were no additional forms of bias detected in the eight included studies.
Discussion
Summary of findings
From an initial pool of 700 studies screened across four major databases and through citations, our review whittled the number down to eight based on strict eligibility criteria. A prominent feature of these studies was their high clinical heterogeneity, which rendered a quantitative meta-analysis unfeasible. However, our qualitative analysis underscored several noteworthy outcomes: a significant reduction in pain, abbreviated LOS, and marked improvements in GI-recovery when acupuncture was employed as opposed to standard care or other control groups. Evaluations of study quality were grounded in STRICTA criteria, while outcomes’ quality was gauged by GRADE. In addition, risk of bias and heterogeneity were assessed using the Cochrane approach.
Overall evidence and limitations
The stringent eligibility criteria, coupled with the language limitations to English and German, yielded a surprisingly low number of relevant studies. This may suggest that this particular topic remains underexplored, especially considering that a sizable portion of acupuncture research originates from Chinese sources. Particularly the rejection of additional stimulation led to elimination of many, distinctly electroacupuncture trials. Conversely, ear acupuncture was not excluded, feeding to the lack of consistency in methodologies and study designs of the included trials and further compounding the challenge. Further variances in study designs (e.g., crossover versus parallel) and inclusion criteria, such as combining gynecological surgeries with GI operations, introduced significant variability in treatment outcomes. The treatment concepts itself varied tremendously which may reflect the heterogeneity of inclusion criteria to the studies and thereby the heterogeneity of patients involved. So far, it was not possible to identify any standardized therapeutic approach or any standardization of how to personalize therapies for recovery from abdominal surgery. We suggest that some theoretical pathway to the selection of acupoints may be developed in the close future, to address different postoperative complaints.
Further, STRICTA-evaluation revealed a low-to-mediocre degree of reporting quality, making it difficult to compare the intervention. Although later trials documented more transparently, only one study referred to STRICTA reporting guidelines. In this context, we would appreciate the development of a generally acceptable score for the assessment of acupuncture studies in continuation and extension of the well-known STRICTA-criteria.
Reporting safety of patients by detailed documentation of (S)AE was conducted by two trials only. Acupuncture is widely known as a treatment with very little side effects, 3 such as minor bleeding, hematoma or needle incision pain. 38,39 Nevertheless, documentation of such remains part of transparent medical research.
Risk of bias assessment was aggravated resulting from short depiction of methods and missing study protocols or missing STRICTA trial reporting standards. Only one of the included studies adopted a design for double blinding, although sham acupuncture has been proven to enable such. 40,41
Implications
The clinical heterogeneity of study design, inclusion criteria, acupuncture treatment and endpoint assessment necessitated a qualitative evaluation of outcomes. Since the study results show large differences in significance, a cautious interpretation is obligatory. Another reason for divergent findings, next to dissimilarity of intervention, could be the inclusion of relatively small trials.
Nevertheless, the partly large and positive results of improved GI recovery after acupuncture are notable and their importance in convalescence after bowel surgery ought to be recognized. Also, the lower analgesic demand in acupuncture patients may be considered alongside the results on pain reduction, its quality of evidence judged as moderate.
Two recent trials integrated the acupuncture treatment in an ERAS®-setting, including roughly half of the included patients of this review. An accentuated interpretation of results seems inadequate because exact influence of fast-track items was not assessed. Still, it may be highlighted that both studies received the lowest risk of bias rating.
As the recently increasing number of studies and its conjunction with fast-track surgery indicates, acupuncture may be developing as emerging clinical field within perioperative medicine. Its promising benefits led to first considerations by the ERAS® society while demanding more transparency. 42 In addition, the German Association of the Scientific Medical Societies (AWMF) recommends postoperative acupuncture after abdominal surgery as a supportive treatment for regeneration. However, a shortage of proficient acupuncturists has led them to moderate their recommendation. 43
Conclusions
The studies reviewed underscore the potential benefits of manual acupuncture in the postoperative phase of abdominal surgeries, especially in facilitating GI regeneration, pain management, and overall patient recovery. However, these findings are tempered by the glaring gaps in research quality. Future studies aspiring for excellence must embrace robust methodologies, including computer-based randomization, rigorous blinding protocols, and stringent allocation concealments. Such endeavors would not only elevate the quality of evidence but could also firmly position acupuncture as a pivotal component in perioperative care.
Footnotes
Authors’ Contributions
S.S.: Conceptualization, Methodology, Formal analysis, Investigation, Writing—Original Draft, Visualization. C.Y.: Conceptualization, Methodology, Validation, Writing—Review & Editing. J.G.: Validation, Resources, Writing—Review & Editing. V.B.: Methodology, Software, Resources. C.R.: Validation, Writing—Review & Editing, Supervision. F.H.: Conceptualization, Validation, Writing—Review & Editing, Supervision. E.G.: Conceptualization, Validation, Writing—Review & Editing, Supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.