
Abstract
Background:
Primary dysmenorrhea is a common gynecological disorder that affects many women of reproductive age. Ginger, a widely used spice with anti-inflammatory properties, has been suggested as a potential treatment for the painful cramps associated with this condition.
Objective:
The aim of this systematic review and meta-analysis was to evaluate the efficacy of ginger for pain management in primary dysmenorrhea.
Methods:
Our systematic review was registered in Prospero (CRD42023418001). Six English (PubMed, Scopus, Web of Science, PsycINFO, CINAHL complete, and Cochrane) and one Persian electric database (SID) was searched up to May 2023 for English or Persian studies that measure the effect of ginger on pain in dysmenorrhea. The Cochrane tool was used to assess the risk of bias of the included studies. Random effects meta-analyses were performed to obtain standardized mean differences (SMD) and 95% confidence intervals (CI).
Results:
Out of the 804 articles initially identified from the search, 24 were included for qualitative analysis and 12 for quantitative analysis after a full-text evaluation. The combined results of the studies indicate that ginger is notably more effective than placebo in reducing both the intensity (SMD = −1.13; 95% CI = −1.59 to −0.68, I 2 = 81.05%) and duration of pain (SMD = −0.29; 95% CI = −0.46 to −0.12). There were no differences between ginger and nonsteroidal anti-inflammatory drugs (NSAIDs) (SMD = 0.01; 95% CI = −0.24 to 0.25), or exercise (SMD = 0.06; 95% CI = −0.66 to 0.78) for pain intensity. Safety-related data were infrequently reported.
Conclusions:
The results of this meta-analysis suggest that ginger can effectively reduce pain associated with dysmenorrhea. The findings are limited due to risk of bias in the included studies and the unclear risk-benefit ratio.
Introduction
Primary dysmenorrhea is a spasmodic or colicky pain that occurs in the lower abdomen in the absence of pelvic diseases and can spread to the back and thighs, and can also be accompanied by nausea, vomiting, and changes in digestive habits. 1,2 It has a prevalence of 16–91% among women of reproductive age, of which 2–29% experience severe pain. 3 Dysmenorrhea can suppress the economic and social aspects of people's lives and negatively affect the quality of life and mental health. 4 –6 Since women facing dysmenorrhea are generally students or workers; it leads to huge losses in the economy and production. 7
The cause of dysmenorrhea has not been definitively identified, but it seems that the increase in the release of prostaglandins F2 (PGF2) and E2 (PGE2) leads to severe or irregular contraction of the uterine muscles and vasoconstriction, and finally ischemia and pain. 8
Currently, nonsteroidal anti-inflammatory drugs are commonly used to treat dysmenorrhea. However, prolonged use of these drugs can lead to a 20–25% tolerance, and result in various side effects, including diarrhea, heartache, nausea, headache, drowsiness, dysuria, lethargy, anorexia, vomiting, indigestion, giddiness, and skin inflammation. In severe cases, the use of these drugs can even lead to stomach ulcers and chronic kidney diseases. 6,9,10 Treatment with medicinal plants is common today because they have been shown to be safe and effective. 11
Although the use of ginger in Indian and Chinese medicine dates back several thousand years, it is now widely recognized as a popular spice. 12 Also, many studies have shown that ginger has anti-inflammatory properties by inhibiting the production of prostaglandins (through inhibition of cyclooxygenase) and leukotrienes. 13 Moreover, it has pleiotropic pharmacological activities like gastrointestinal, antioxidant, and analgesic effects. 14 Therefore, in addition to relieving the pain of dysmenorrhea, ginger can also relieve its digestive symptoms, including nausea, vomiting, and diarrhea. 13,15
A number of meta-analysis studies have been conducted on the effect of ginger on the severity of dysmenorrhea pain. In a meta-analysis that was conducted on seven clinical trial studies, a clear effect of ginger on pain intensity perceived by a visual scale in people with primary dysmenorrhea was confirmed. 14 In another meta-analysis that reviewed five studies, ginger, and nonsteroidal anti-inflammatory drugs were equally effective in reducing pain. 11 However, the number of meta-analysis and systematic reviews conducted with the aim of investigating the effect of ginger on pain duration is much less. In a meta-analysis with nine studies, the intensity of pain in the ginger group has been investigated compared witho placebo, but in terms of pain duration, only cinnamon has been investigated, and a study that measures the relationship between pain duration and ginger consumption has not been included. 16
However, ginger, a well-known and widely used plant in Persian medicine (PM), has been emphasized for its pain-relieving effects and has been studied by researchers in this field for its potential in improving dysmenorrhea. Therefore, various clinical studies in Persian language have been conducted to investigate the efficacy of this herbal plant in Iran or Persian-speaking countries, and these studies are not commonly included in meta-analyses due to language bias.
The aim of this study was to systematically review studies on the effect of ginger on pain-associated variables in primary dysmenorrhea based on Persian and English language studies to obtain the complete body of evidence. Studies comparing ginger to placebo, pharmacological or nonpharmacological interventions were included.
Methods
To assess the impact of ginger on pain intensity experienced by individuals with primary dysmenorrhea, this systematic review and meta-analysis adhered to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. 17 The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD42023418001.
Search strategy
We conducted a comprehensive search across six English electronic databases, namely PubMed, Scopus, Web of Science, PsycINFO, CINAHL Complete, and Cochrane, as well as one Persian database called SID. The search encompassed records in both English and Persian languages, up until September 20, 2023. In addition, we utilized Google Scholar to search for relevant gray literature. The search queries utilized combinations of keywords such as “ginger” and “dysmenorrhea,” along with their synonyms. The detailed search strategies employed for each database can be found in the Supplementary Data S1. Furthermore, we screened the references of the included studies to identify any potentially eligible article for inclusion.
Eligibility criteria
We incorporated interventional studies, whether randomized or nonrandomized, which explored the impact of ginger on pain intensity and/or pain duration specifically related to primary dysmenorrhea in human subjects, regardless of its underlying causes. We also included studies that lacked a control group. The following types of studies were excluded from our analysis: (1) Studies that did not investigate pain in the context of dysmenorrhea; (2) studies that provided insufficient data to calculate the effect of ginger on pain intensity in dysmenorrhea; (3) duplicate studies or those with overlapping participants; (4) observational studies, reviews, editorials, conference papers, case series/reports with fewer than five cases, or animal experiments; and (5) qualitative study designs. Moreover, for the purpose of conducting a meta-analysis, studies without control groups were also excluded.
Study selection
R.M. and N.S. conducted separate screenings of titles and abstracts for potentially eligible studies using EndNote. Subsequently, the full texts of identified studies were independently obtained and evaluated by the same authors. Any conflict concerning study design or methods, as well as the ultimate decision on including studies in the review, was resolved through a consensus meeting with M.P.
Data extraction
Two authors (R.M. and N.S.) autonomously extracted the relevant information from the included articles. In case of any disagreement, further discussions were held to reach a consensus. The extracted data encompassed various general characteristics of the included studies, including the first author, publication year, country of origin, study type, sample size, interventions, main findings, potential side effects, and limitations.
Risk of bias assessment
We evaluated the potential for bias in the included studies using the Cochrane Collaboration's risk of bias tool. 18 Two reviewers, RM and NS, independently appraised the studies for bias. The assessment categorized studies into three grades: “'Low risk” when risks were adequately addressed due to clear study design, “unknown risk” when risks persisted due to insufficiently stated details, and 'high risk' when significant risks that could impact the study outcome were identified through biased study design. In cases of disagreement, a third reviewer (M.P.) served as an arbitrator.
Quantitative analysis
The overall effect size [standardized mean difference (SMD)] was derived from the mean changes and standard deviation (SD) of pain intensity in both the tDCS and Sham groups. SD was calculated using the standard error (SE) and 95% confidence interval (CI) based on the method outlined by Hozo et al. 19 Pooled unstandardized differences in means and corresponding confidence intervals from the studies were computed using a random effects model. Heterogeneity between studies was assessed using the chi-squared test and I 2 statistic. To estimate heterogeneity variance in meta-analyses, we used the restricted maximum likelihood (REML) method. Publication bias risk was evaluated through Egger’s and Begg’s tests, examining the relationship between effect size and standard error or sample size with resulting p-values indicating asymmetry significance. A funnel plot, plotting effect size against standard error for each study, was used to visualize publication bias; symmetrical distribution suggests low risk, while asymmetry indicates high risk. A sensitivity analysis tested the pooled effect size's robustness. All analyses were conducted using Stata software (version 17, Stata Corporation, College Station, TX), and a significance level of 0.05 was applied.
Results
Study selection
Figure 1 depicts the PRISMA flow diagram. The search criteria initially yielded 804 articles from the databases based on the proposed keywords. After full-text evaluation, 24 studies for qualitative analysis and 12 studies for quantitative analysis were included.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) of the included studies.
Description of studies
Table 1 shows the overall data of the included studies. Of the 24 studies included in this systematic review, 17 studies were RCT, 21,22,24 –29,31,34 –37,40 –42 4 studies were non-RCT, 30,32,33,38 and three studies were crossover. 23,25,39 Overall, 18 were conducted in Iran, 20 –22,24 –29,32,36 –42 four in India, 30,31,33,34 one in Pakistan, 35 and one in Indonesia. 23 Participants in two studies 21,23 were high school students, in three studies were nursing students, 30,31,33 and in 19 studies were university students. Overall, the sample size in the ginger group ranged from 10 to 78. Among included trial studies, in 22 studies, ginger was in the form of dry powder. In one study, ginger oil was smeared, 23 and one study used ginger tea. 30 The daily intake of powdered ginger ranged from 500 mg to 2,000 mg. The first three days of the period were the most usual ginger therapy duration.
Study Characteristics
BID, twice a day; DRSP, daily record of severity of problems; MDQ, menstrual distress questionnaire; NRS, numerical rating pain score; QID, four times a day; TID, three times a day; VAS, visual analog scale (0–10 cm); VMS, verbal multidimensional scoring system; WBS, Wong-Baker Faces Pain Rating Scale.
Ginger was compared to placebo in 9 studies: five two-arm trials comparing ginger to placebo, 20 –22,26,39 one three-arm trial comparing ginger to placebo and zinc, 21 two three-arm trials comparing ginger to placebo and valerian, 29,36 and one three-arm trial comparing ginger to placebo and curcumin. 37 The main finding in all studies was consistent and pain duration or severity significantly decreased in ginger groups compared to placebo, except in one study. 20
Atashak et al. 20 used the Combination of Exercise and ginger in comparison with exercise, and placebo. In addition, Pakniat et al. 40 conducted a study comparing the combination of ginger and mefenamic acid with the combination of mefenamic acid and placebo; consequently, pain severity was significantly reduced in the ginger group. In a similar study, Adib Rad et al. 25 applied ginger in the first cycle and novafen in the second cycle, comparing novafen in the first cycle with ginger in the second cycle. However, no significant difference in pain severity was detected.
To measure pain intensity, the visual analog scale (VAS) was the most common measurement scale. Three studies measured intensity on a 5-point Likert scale 3,15,19 and two studies used a menstrual distress questionnaire (MDQ) and numerical rating pain score (NRS) 17,18 Khayat et al used a daily record of severity of problems (DRSP), 37 and Davood Abadi et al. used Wong-Baker Faces Pain Rating Scale (WBS). 36 Four studies assessed pain duration, three studies collected data on the number of days in pain, 4,29,32 and one study collected the number of days without pain.
Adverse events
Sixteen studies did not report safety-related data, and two studies reported that no side effect occurred. Five studies reported safety data and reported headache and heartburn as the most common side effects of ginger. 6,21,24,26,40
Risk of bias within studies
Bias due to random sequence generation (selection bias) was low in 12 studies, high in 11, and unclear in one study. Bias due to allocation concealment (selection bias) was deemed low in 12, high in nine, and unclear in three studies. The performance bias and detection bias were reported high in six and ten studies, respectively. On average, the quality assessments indicated that the risk of bias was moderate (Figs. 2 and 3).
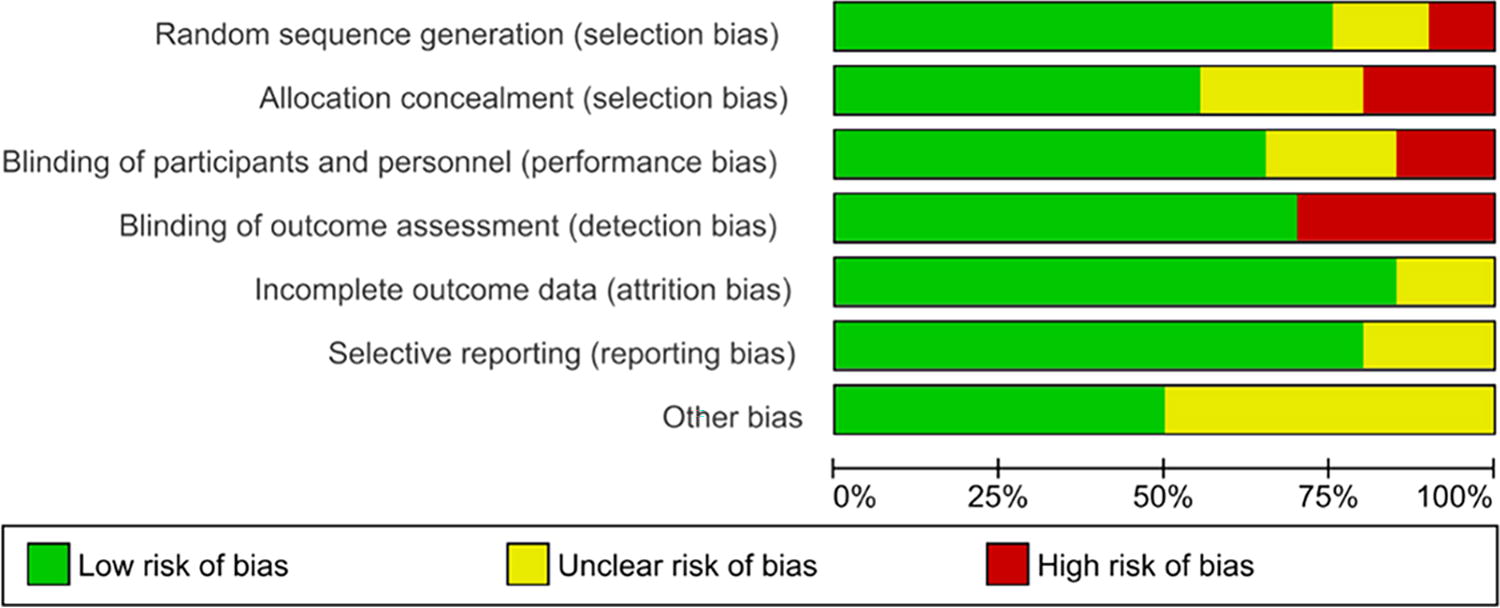
Risk of bias in the individual domains for all included clinical trials.
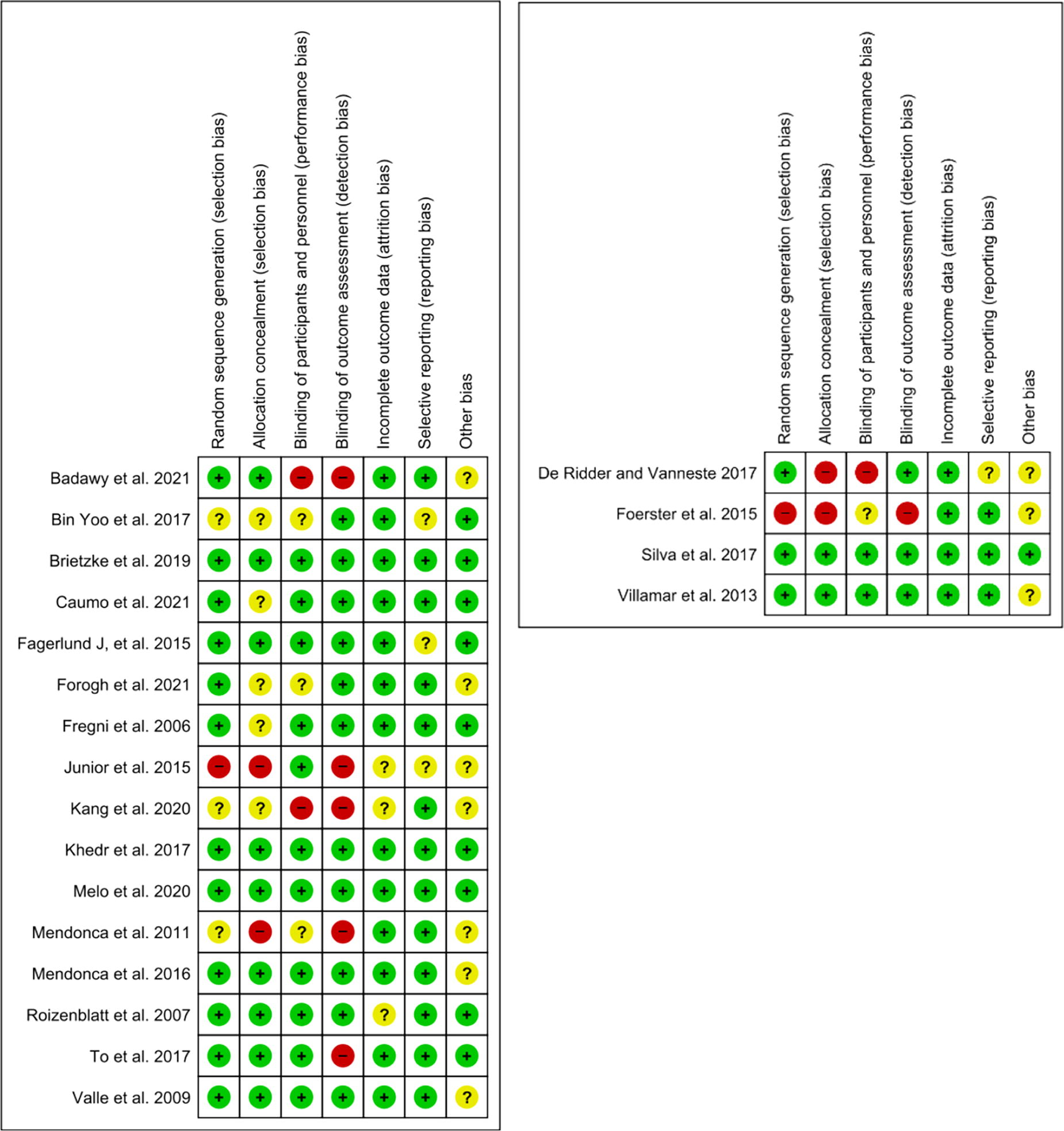
Risk of bias of included randomized clinical trials (left) and crossover trials (right).
Synthesis of results
In total, 12 studies were included for meta-analysis.
Pain intensity of ginger versus placebo
Overall analysis
In total, six studies assessed the effect of ginger compared to placebo on pain intensity in women with dysmenorrhea. Analysis showed that participants receiving ginger experience a significant decrease in pain intensity compared to controls (SMD = −1.13; 95% CI = −1.59 to −0.68). As notable heterogeneity was identified (I 2 = 81.05%) and to detect potential sources of heterogeneity, subgroup analysis was performed (Fig. 4).
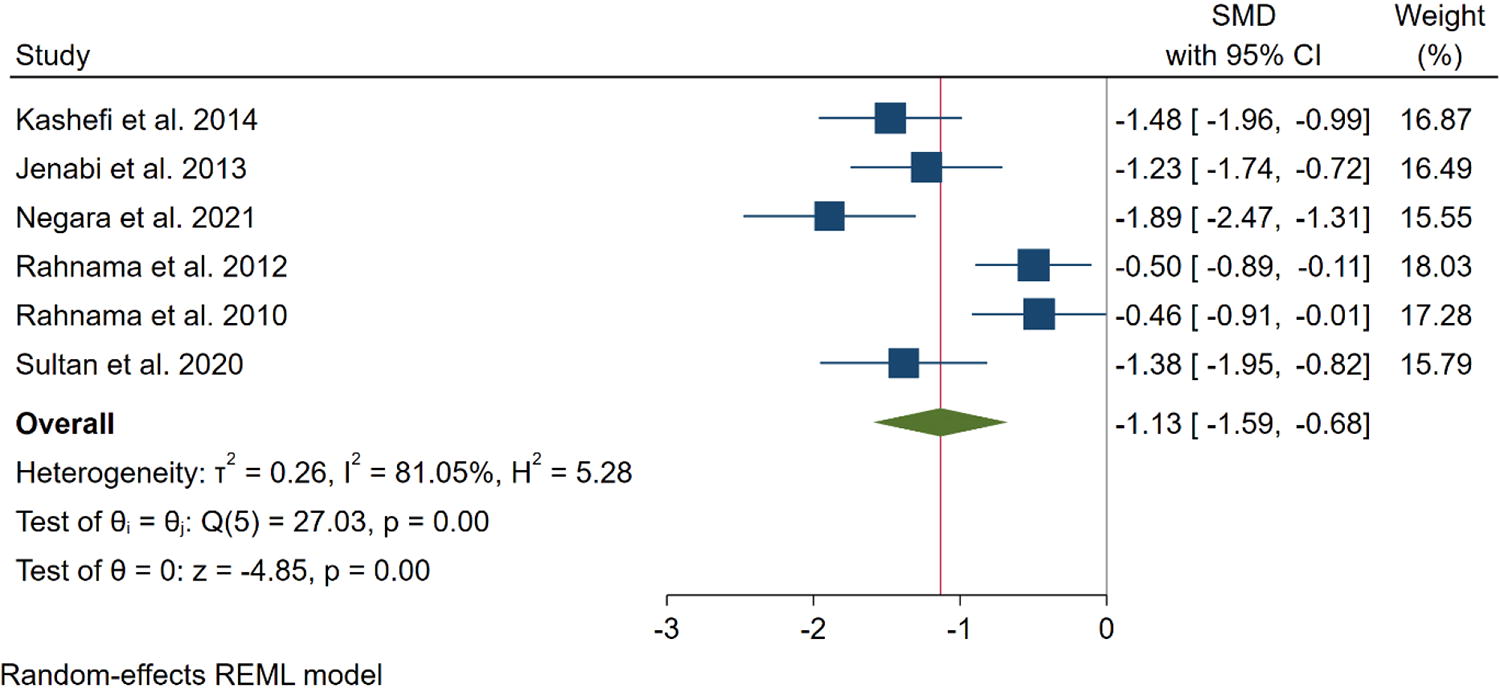
Meta-analysis of the effect of ginger compared to placebo on pain intensity in women with dysmenorrhea.
Subgroup meta-analysis
Five out of six studies examining the impact of ginger on participants' pain intensity were RCTs, and the same one using oral capsules as the root of administration. These studies demonstrated a noteworthy reduction in pain intensity (SMD = −0.99; 95% CI = −1.43 to −0.55) (Supplementary Figs. S1 and S2). Among these trials, Negara et al.’s study was the only one that employed a within-subject crossover design and utilized ginger oil. A subgroup meta-analysis was conducted based on language and nationality. The results indicated that studies conducted in English had a significantly greater impact on improving pain intensity compared to Persian language studies (SMD = −1.27; 95% CI = −1.73 to −0.81 and SMD = −0.46; 95% CI = −0.91 to −0.01, respectively). In addition, the findings revealed that studies conducted in Iran had a significantly lower effect on improving pain intensity (SMD = −0.90; 95% CI = −1.41 to −0.40 and SMD = −1.63; 95% CI = −2.13 to −1.14, respectively) (Supplementary Figs. S3 and S4) (Table 2).
Additional Meta-Analysis of Included Studies
NA, not applicable; NSAIDs, nonsteroidal anti-inflammatory drugs; RCT, randomized controlled trial.
Sensitivity analysis and publication bias
The omission of Negara et al. 23 seems to have a relatively larger influence (when compared with other studies) on the estimation of the overall effect size (effect size = −0.99; 95% CI = −1.43 to −0.55, p < 0.001) and it does not influence SMD or 95% CI very much due to its low weight in the meta-analysis, which is 15.55% (Supplementary Fig. S5).
The funnel plot shows an asymmetrical distribution of data, representing a possible publication bias. This matched with what was found in Egger’s and Begg’s tests; Eggers’s and Begg’s tests showed high risk (p < 0.001 and p = 0.06, respectively) for publication bias (Fig. 5).
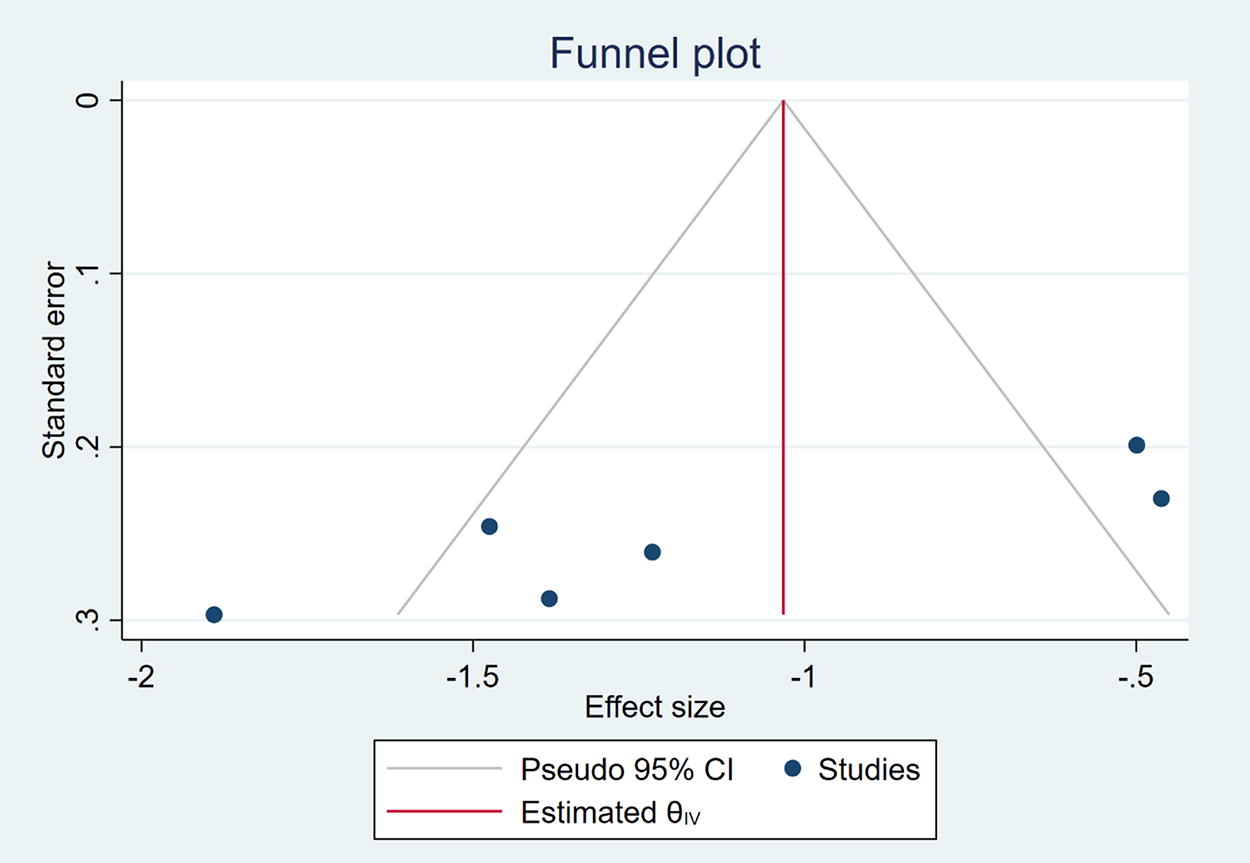
Funnel plot of the publication bias. CI, confidence interval.
Pain duration. Ginger versus placebo
Overall analysis
Four studies measured the pain duration of dysmenorrhea. 27,29,32,36 The meta-analysis showed that ginger significantly had more effect on the reduction of pain duration in comparison to the placebo group (SMD = −0.29; 95% CI = −0.46 to −0.12) (Fig. 6).

Meta-analysis of the effect of ginger on pain duration in participants with dysmenorrhea in comparison to placebo group.
Subgroup meta-analysis
Subgroup analysis was performed based on the design of included studies; in crossover, and RCT studies ginger significantly had more effect on improvement of pain duration than placebo (SMD = −0.57; 95% CI = −1.47 to 0.32, and SMD = −0.28; 95% CI = −0.45 to −0.12 respectively), even though, RCT studies had a lower effect, there was no significant difference (p = 0.57) (Supplementary Fig. S6) (Table 2).
Pain intensity. Exercise versus ginger
Two studies 27,32 measured the difference in the effect of exercise and ginger on pain reduction and showed that there was no difference between them (SMD = 0.06; 95% CI = −0.66 to 0.78) (Supplementary Fig. S7) (Table 2).
Pain intensity. NSAIDs versus ginger
Analysis showed that there was no difference between NSAIDs and ginger in the reduction of pain in dysmenorrhea (SMD = 0.01; 95% CI −0.24 to 0.25). Analysis also showed there was no difference between mefenamic acid and ginger in reduction of pain in dysmenorrhea (SMD = 0.013; 95% CI = −0.9 to 0.35) (Supplementary Figs. S8 and S9) (Table 2).
Discussion
This review presents evidence from a meta-analysis of studies that ginger is an effective treatment for reducing dysmenorrhea symptoms. The pooled results demonstrate that ginger is particularly effective in reducing pain intensity and duration compared to placebo. However, the analysis also found that ginger is equally effective as NSAIDs in reducing pain severity. Furthermore, the analysis did not reveal significant differences between the effects of exercise and ginger on pain reduction.
Mechanisms
The accumulation of various substances such as prostaglandins, chemokines, cytokines, growth factors, and oxytocin induces myometrium hypercontractility and vasoconstriction, which are the primary mechanisms responsible for menstrual pain in cases of primary dysmenorrhea. 1 Prostaglandin F2α and E2 concentrations are higher in women with dysmenorrhea, 43 as these molecules are involved in inflammation and are synthesized by the enzyme Cyclooxygenase (COX). 44 NSAIDs, which are typically used to treat menstruation discomfort, reduce inflammation by inhibiting COX-1 and COX-2. Ginger, which contains gingerols and gingerdiones, also has anti-inflammatory properties and can inhibit the production of leukotrienes and prostaglandins by inhibiting COX activity. 45 In addition, ginger compounds can interact with the lipoxygenase pathway, reducing the activity of the 5-lipoxygenase enzyme. 46 This suggests that ginger may be effective in treating menstrual pain as an NSAID.
Numerous studies have shown that ginger compounds can affect eicosanoids derived from arachidonic acid and the synthesis of thromboxane. The arachidonic acid cascade is thought to generate eicosanoids, including prostaglandin E2 and thromboxane, which may contribute to inflammation and act as a platelet aggregation agonist. 42,46 –49
Ginger's impact on the activity of the cyclooxygenase enzyme leads to a decrease in the production of prostaglandins and thromboxane through the cyclooxygenase pathway. This has been demonstrated in several studies. 42,50,51 Therefore, ginger, which activates endorphin receptors and acts as a thromboxane synthetase inhibitor, may be effective in reducing pain associated with dysmenorrhea. 52
Geographical attention
This review only included trials conducted in Asia, which raises questions about the applicability of these results to women from other cultures and populations due to the differences in pharmacokinetics and expectations of outcome. While a study in Denmark found that ginger has analgesic properties for pain caused by osteoarthritis, and another study in Georgia showed that ginger could reduce muscle pain caused by exercise, 53,54 it is unclear if these findings can be extended to non-Asian populations for the treatment of dysmenorrhea. Therefore, further studies should be conducted in different parts of the world to determine the effectiveness of ginger in providing pain relief, particularly for dysmenorrhea, in various populations.
Patient values and preferences
While medical treatments such as NSAIDs and oral contraceptives are highly effective in treating dysmenorrhea, there is still a failure rate of 20% to 25%. 15 Traditional, complementary, and alternative treatments, including herbal supplements, may be preferred by some individuals. 55,56 Ginger, in particular, may be a viable alternative for women with dysmenorrhea who either cannot or choose not to use conventional medications. When making treatment decisions, patients' values and preferences should be taken into account. A few recent research suggests that individuals may consider herbal supplements to be safer than pharmaceutical drugs, leading to a preference for herbal supplements. 57,58
Topical/orally
Studies have demonstrated that both oral consumption and topical application of ginger can reduce the intensity of menstrual pain. For instance, ginger compresses applied under the stomach area have been shown to be more effective in reducing menstrual pain than warm compresses. 59 In addition, ginger oil has been found to effectively reduce menstrual pain. 23 In fact, research suggests that ginger oil may be even more effective than raw ginger in managing different types of pain. 60
Therefore, both oral consumption and topical use of ginger may be helpful in managing dysmenorrhea. It is important to note, however, that blinding in studies involving ginger may be challenging due to its unique aroma and taste. This may lead to positive expectations that overestimate the observed effects. Although blinding has not been assessed in any trial, its effectiveness remains uncertain.
Safety remarks for using ginger
Although ginger is generally considered safe for most people, some potential side effects may occur. These may include mild gastrointestinal symptoms such as heartburn, diarrhea, or stomach upset. In rare cases, ginger may cause allergic reactions such as rash, hives, or difficulty breathing. 61 Ginger may also interact with some medications, including blood thinners (antithrombotic agents) and diabetes medications, so it is important to consult with a health care provider before using ginger as a treatment for menstrual pain. 62,63 Generally, reporting of safety-related data was insufficient in the included studies, which limits the evaluation of the risk-benefit ratio of ginger in primary dysmenorrhea.
Limitations and strengths
This systematic review and meta-analysis study has some limitations, such as a relatively high rate of low-quality pooled studies, studies conducted in limited resource settings, absence of necessary data for meta-analysis, and samples that may not be representative of the community, as most studies focused on students. These are rather common shortcomings seen in our recent publications as well. In addition, it is important to address the necessity for additional research to determine the most effective approach regarding treatment initiation, appropriate dosage, optimal duration, and potential contraindications or instances where the use of ginger should be avoided. However, to address these limitations, there are priorities that should be implemented in this research, including the inclusion of newly published trials, missed trials from previous meta-analyses, and new approaches for meta-analysis, such as considering alternative approaches like exercise as a therapeutic method, as well as studies conducted in the Persian language. By addressing these priorities, this systematic review and meta-analysis study could potentially improve the quality of its findings and enhance our understanding of the effectiveness and safety of ginger for relieving primary dysmenorrhea symptoms.
Conclusions
The results of this meta-analysis suggest that ginger can effectively reduce pain associated with dysmenorrhea. The meta-analysis results should be interpreted with caution due to the risk of bias in the included studies, the high heterogeneity between studies, limited sample sizes, and the unclear risk-benefit ratio. To obtain a more accurate and reliable understanding of the results, larger sample sizes and better methodologies should be used in future studies.
Confirmation Statement
All the authors declare that they are employed at an academic or research institution as researchers or faculty members where research or education is the primary function of the entity.
Authors’ Contributions
Conception and designing of study: R.M. and M.P.; data curation: N.S., H.G., H.G., and R.Z.; data analysis: R.M., G.H., and M.P.; article drafting: R.M. R.Z., G.H., and M.P.; critical revision: H.C. and M.P.; supervision: R.M. and M.P.; and all the authors read and approved the final version of the article.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Authors Disclosure Statement
The authors declare that there is no competing interest.
Footnotes
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Figure S8
Supplementary Figure S9
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.