
Abstract
Objective:
Binaural beats, or the perceptual auditory illusions created when simultaneously presenting two similar frequencies to each ear separately, have been used to reduce anxiety in various procedures. Unfortunately, no prior study involved preprocedure binaural music exposure among patients undergoing upper gastrointestinal endoscopy, and this study sought to investigate its effect on anxiety and tolerance among participants undergoing sedation-free upper gastrointestinal endoscopy.
Methods:
The prospective, controlled, randomized trial included the participation of 96 Turkish patients aged between 18 and 70 years who were scheduled for an upper gastrointestinal endoscopy, regardless of sex or illness, and were divided randomly into two different groups to undergo endoscopy, namely, the binaural beats group (n = 48) and a control group (n = 48). Patients in the binaural beat music group wore headphones, and music was given 15 mins before endoscopy; however, no particular treatment was given for either group. Anxiety levels were assessed by using the State Trait Anxiety Inventory questionnaire, in addition to changes before and after endoscopy to measure patient satisfaction based on the physician’s recorded numbers of retches noted by doctors as tolerance was documented and compared among both groups.
Results:
The results showed that following this procedure, in the music group, state scores remained significantly lower than before them (p = 0.016), compared with the control group (p > 0.05). There was no significant difference regarding changes in diastolic or systolic heart rate or blood pressure (p > 0.05). However, the procedure tolerance and satisfaction scores were significantly higher in the music group than those without music (p < 0.05).
Conclusion:
For patients undergoing upper gastrointestinal endoscopy, music with binaural beats was found to significantly reduce anxiety levels and increase patient tolerance, providing an alternative option to sedative medications as a potential sedative treatment option.Clinical trials registration number: NCT06114524.
Introduction
Gastrointestinal diseases are highly prevalent and carry significant morbidity and mortality rates among all age groups. 1 Gastroscopy is an imaging procedure used for diagnosing and treating upper gastrointestinal conditions such as gastroesophageal reflux disease, peptic ulcer disease, and stomach cancer. However, gastrointestinal endoscopy procedures are invasive and often cause patient anxiety and discomfort. Application of anesthesia or sedation can significantly lower patient anxiety and stress, with benzodiazepines and opioids being some of the most frequently utilized agents to achieve this purpose in clinical practice. 2,3 However, the use of sedative agents may result in cardiopulmonary complications such as phlebitis, hypoxemia, hypoventilation, airway obstruction, hypotension, vasovagal episodes, and cardiac arrhythmias, as well as aspiration. 4,5 Therefore, for short-duration endoscopic procedures such as upper gastrointestinal endoscopy, performing sedation-free endoscopy has become a viable solution to minimize side effects and costs.
Music therapy has been proven effective in reducing stress and anxiety in various medical conditions. 6 Music can affect the brain’s right hemisphere, triggering emotional reactions and reducing pain perception. 7 Music-aided digestive endoscopy has been shown to alleviate discomfort and anxiety, increasing patient satisfaction. 8 Gerald Oster described binaural beat music as a unique form of audio 50 years ago. 9 Binaural beats happen when two sounds with identical intensities but differing frequencies are presented separately. When binaural beats are played to a person listening through stereo headphones, it is believed that the brain can receive distinct signals from both ears instead of perceiving the two frequencies in isolation, thereby causing the creation of a third sound, which is the distinction between the two. Research has demonstrated the efficacy of binaural beats in not just enhancing cognitive functions but also dramatically reducing anxiety levels as well as pain perception. Garcia-Argibay et al. conducted a meta-analysis showing that binaural beats consistently reduce anxiety and enhance cognitive abilities. 10 Mallik and Russo conducted a randomized clinical trial demonstrating that music coupled with auditory beat stimulation significantly reduced anxiety levels. 11 According to a study by Wiwatwongwana et al. on patients who underwent cataract surgery, those exposed to binaural beats had reduced anxiety and heart rates compared with controls. 12 Olcucu et al. conducted experiments on male patients undergoing diagnosis cystoscopy and ureteral stent removal, finding that the binaural beats group had significantly lower intervention tolerance rates, lower visual analog scale (VAS) scores for pain, and decreased anxiety scores. 13 Isik et al. reported similar findings in dental surgery patients, with preoperative anxiety reduced by binaural beats. 14 The binaural rhythm has been proven to alter a person’s physiological state through various studies. Studies have demonstrated that binaural beats in the theta band (4–7 Hz) reduce anxiety and increase hypnotic susceptibility. 14 –16
While binaural beats have been studied in various medical contexts, their use during upper gastrointestinal endoscopy procedures has not been explored. Due to high patient volumes and limited recovery rooms, pharmaceutical sedation is not used in our endoscopy unit. Therefore, this prospective randomized study aims to investigate the impact of using binaural beats, especially in the theta frequency, as an endoscopic sedative to reduce anxiety levels and improve procedural tolerability.
Materials and Methods
In this study, no interim analysis or stopping guideline was employed. The study was conducted without predefined interim assessments or criteria for early termination.
Study design
A randomized controlled trial was conducted in the endoscopy unit of the gastroenterology clinics of Abdurrahman Yurtaslan Oncology and Training Research Hospital in the capital city of Turkey between August 2023 and October 2023.
Sample and setting
The sample size for this study was determined based on the findings of a previous study with a primary outcome measure of the State-Trait Anxiety Inventory (STAI). In this study, a 5-point difference was observed in the preprocedure and postprocedure STAI-state (STAI-S) score change values between the two groups. Assuming that this 5-point difference in score changes between preprocedure and postprocedure will be considered significant, with an effect size (d) of 0.78, 95% power, and a 0.05 significance level, it was calculated that a minimum of 44 participants per group, totaling at least 88 participants, would be required for our study. 17 The group sample sizes were determined utilizing G-power 3.1 (Kiel, Germany).
A total of 96 patients were included in this study. Two researchers collected data. Patients aged 18–70 years who were scheduled for upper gastrointestinal endoscopy appointments were recruited without considering sex or underlying disease. Patients who had previously undergone endoscopic procedures were using medication for anxiety or panic disorder, needed urgent endoscopic intervention, had advanced dementia, had hearing problems, had anatomical or inflammatory disorders in the external ear canals, or did not want to listen to music for 15 min before the procedure were not included.
Procedure
The patients arriving for endoscopy procedures were included in the study. The binaural (music) beats group (n = 48) and the control group (n = 48) were randomly assigned to the eligible individuals. Throughout the subject recruiting phase, a block size of two was employed in blocked randomization to ensure a good participation balance between the two groups. A sequence group (either music or control) was created using computer-generated random codes in advance. This sequence group was then placed in a sealed envelope with a unique serial number by a researcher who was not involved in the investigation. These envelopes were opened only after the eligible participants agreed to participate and completed the consent process. In this study, only the researcher evaluating the results was blinded to the allocation sequence. The participants, medical personnel, and the gastroenterologists were not blinded to the intervention’s allocation due to its nature.
The participants were taken to a quiet room and asked to complete the STAI-S and STAI-trait (STAI-T) questionnaires before the endoscopy procedure. The STAI-S was then completed again 5 min after the endoscopic procedure. Blood pressure and heart rate were measured after completing the forms and 5 min after the endoscopy procedure. The endoscopy nurse provided information to the patients in the music group about binaural beats and their potential sedative effects. After completing the preprocedure forms, the music group received an MP3 player (Meizu Slim 8GB MP3 Player, Meizu Technology Co. Ltd., China) and in-ear stereo headphones. The music therapy was administered for 15 min before the procedure. The patients were allowed to adjust the volume as desired. Binaural beats (relaxing theta waves at 5 Hz, MusicMindMagic Production) were played for those in the music group. The endoscopic procedures were performed immediately after the music ended. The music was not played during the procedure because it was preferred that the patients could hear the related instructions.
The control group was kept in a quiet room for 15 min before the procedure. No music was played for the control group to assess the pure effects of binaural beats. During this time, they were not engaged in specific activities and were instructed to relax in a quiet environment. This approach was taken to ensure that any difference in outcomes between the groups was attributable to the intervention of music with binaural beats and no other variable. The endoscopic procedures were performed immediately after 15 min.
Topical anesthesia was given to all patients before the procedure. All procedures were performed using a video endoscope (Fujinon EG-590 WR, FUJINON Corporation, Saitama, Japan) by two expert endoscopists with over 15 years of experience, each of whom has successfully conducted more than 2,000 upper gastrointestinal endoscopies annually. Nursing staff distributed and collected all forms, accompanied the patients during their procedures, monitored the music listening time, and recorded vital signs. Procedure durations were determined from the procedure records. It is to be noted that no change was done to the trial methodology once it was commenced.
Instruments
STAI is a valid self-report measure comprising 40 items; 20 assess state anxiety (STAI-S), while the remaining 20 measure trait anxiety (STAI-T). Each component scores from 20 to 80, with higher scores indicating greater anxiety levels; it is widely employed in music research. 18 Cronbach’s alpha values for STAI-S and STAI-T have been reported at 0.92 and 0.90, respectively, and test–retest correlations are 0.84 and 0.86. The STAI-T assesses an individual’s overall anxiety tendencies and their general anxiety level. The STAI-S measures a participant’s current anxiety intensity. The two tests take ∼5 min to complete.
Since no standardized endoscopic toleration scale was available, a customized toleration assessment scale was developed for this study. The patient toleration scale encompasses a four-point scale from 1 to 4, increasing patient discomfort (Table 1).
Four-Point Tolerance Scale
After the procedure, the patients were asked questions to evaluate their satisfaction with the unsedated gastroscopy (worse than expected, as expected, or better than expected) and their willingness to undergo the unsedated procedure again for their health (no or yes). The music group was also asked a question with three response options (yes, not sure, or no) regarding whether the music increased relaxation and whether they would like to listen to the same music again during a future procedure.
Statistical analyses
Statistics were performed using IBM SPSS version 27 (IBM Corp., Armonk, NY, USA). Independent-sample t-tests and Pearson’s chi-squared tests were employed to compare numerical and categorical variables. Repeated measures analysis of variance was performed to analyze the impact of the intervention. This analysis assessed the group, time, and interaction effects (group × time). Results were considered statistically significant at p < 0.05. As part of the analysis, baseline demographic characteristics for participants in both music and control groups were compared to verify whether randomization worked effectively and ensure that both groups were comparable from its inception.
Outcome consistency
In the article, no modification or change to trial outcomes was reported. The study design and outcome measures described in the article remained consistent throughout the study period, as presented in the Methods section. The article provides a detailed account of the study’s methodology and results without indicating any alteration to trial outcomes during or after the commencement of the study
Ethical approval
Ethical approval was obtained for this research from the hospital’s clinical ethics committee before starting (no. 2023-09/380). All research followed the principles outlined in the Declaration of Helsinki, and written and verbal informed consent was collected from each patient for this project. Ethical considerations were carefully reviewed, especially given that the control group did not receive the music intervention that could potentially alleviate anxiety. The institutional ethics committee reviewed and approved the study design, ensuring adherence to ethical standards and participant safety. (Fig. 1).
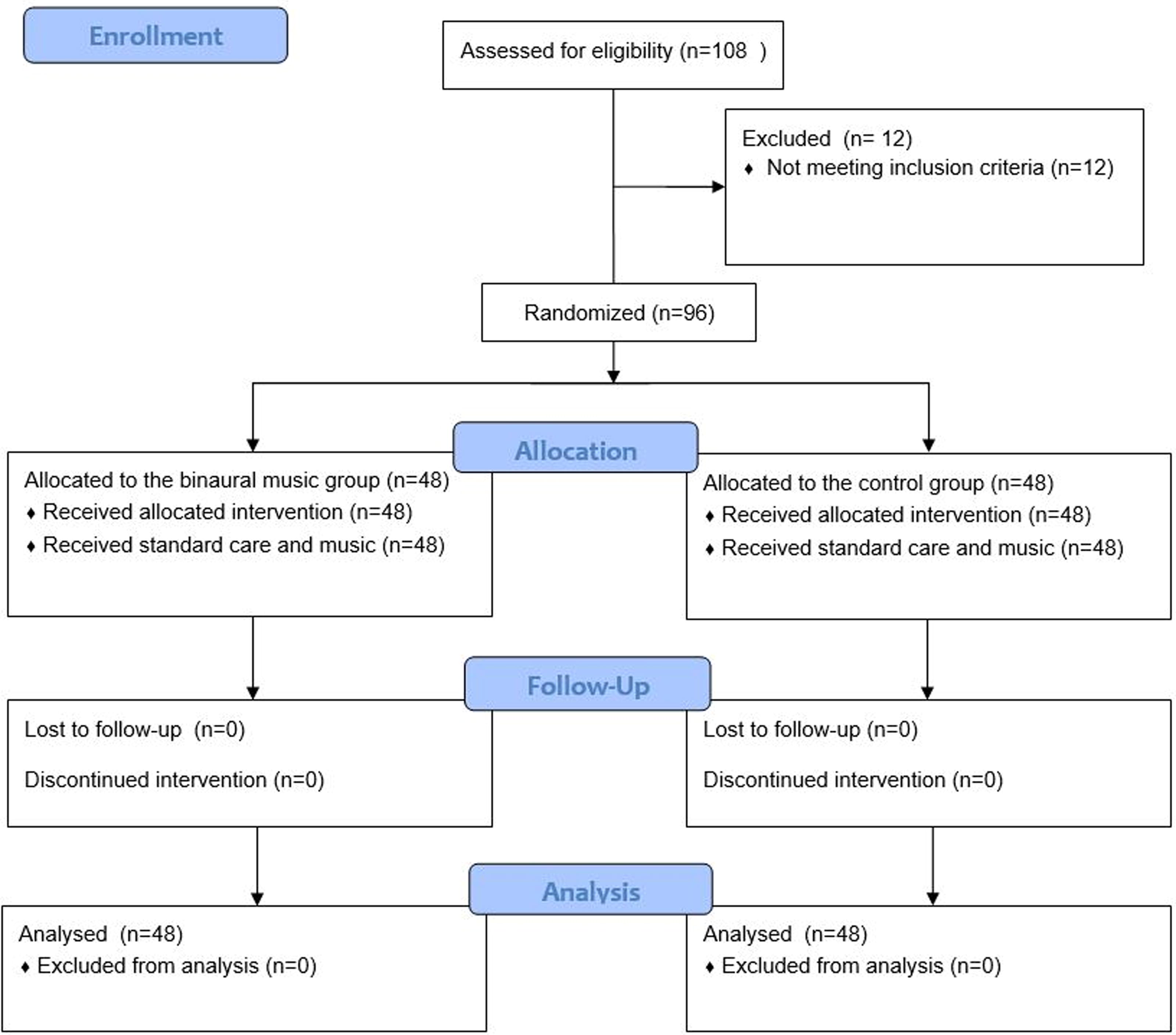
CONSORT flowchart.
Results
Data were collected from September 15, 2023, to October 25, 2023. A total of 108 patients were assessed, and 12 were excluded from the study as they did not meet the eligibility criteria. All 96 patients who participated in the study underwent the procedure, and all endoscopic procedures were completed. Regarding the binaural music intervention, none of the subjects experienced any discomfort. No significant adverse event occurred during any procedure.
Table 2 provides the demographic characteristics of the patients from both groups. There was no significant difference in age, sex, or education level. There were also no difference in specific indications of endoscopy (p > 0.05), which suggests the same demographic profile across both. In the same way, there was no statistically significant difference between the groups concerning STAI-T scores (p > 0.05), which suggests that they had the same initial levels and tendencies toward anxiety. There was no significant difference in procedure duration between the two groups.
Demographic Characteristics of the Patients
Values are presented as the mean ± SD and number (%).
SD, standard deviation; STAI-T, State-Trait Anxiety Inventory–trait.
Table 3 shows changes in systolic and diastolic blood pressure, heart rate, and STAI-S levels before and after the procedure, as well as the interaction effect (group × time) between the music group and control group. In the music group, the mean STAI-S score decreased by 5.14 points, whereas no significant change was observed in the control group. The interaction effect for STAI-S scores was found to be significant [group × time; F(1,94) = 6.029, p = 0.016] (Fig. 2). No significant interaction effect was found for the other parameters (p > 0.05).

Mean values of STAI-S score before and after the procedure in music and control groups. STAI-S, State-Trait Anxiety Inventory–state.
Descriptive Statistics and Effects of Intervention in Control and Music Groups over Time
Values are presented as the mean ± SD. Bold indicates p < 0.05.
DBP, diastolic blood pressure; G, groups; G × T, group × time; HR, heart rate; SBP, systolic blood pressure; STAI-S, state-trait anxiety inventory–state; T, time (before – after).
Table 4 displays the results of patient satisfaction. A significantly higher proportion of participants in the music group than control indicated that they would repeat an endoscopic procedure without sedation a second time (p < 0.05). Furthermore, many music group patients expressed interest in listening to similar music if future sedation-free endoscopic procedures needed to occur.
Patient Satisfaction
Values are presented as number (%). Bold indicates p < 0.05.
Table 5 displays patient tolerance evaluation results by the performing physician. Patient tolerance in the music group was significantly greater than in the control group (p < 0.05).
Patient Tolerance
Bold indicates p < 0.05.
Discussion
The prospective randomized controlled trial conducted demonstrates that listening to music containing binaural beats significantly reduces anxiety and enhances tolerance among patients undergoing upper gastrointestinal endoscopy without sedation. These findings align with previous studies that demonstrated the beneficial effects of binaural beats on decreasing anxiety and increasing tolerance during various medical procedures. Notably, our research adds new knowledge to the existing body by exploring an area not previously investigated—binaural beat application in upper gastrointestinal endoscopy. The significant decrease in STAI scores postprocedure among music group subjects as compared with the control group shows the potential of binaural beats as a nonpharmacological solution for anxiety reduction in clinical settings. Furthermore, the increased patient satisfaction and willingness to repeat procedures observed among music group patients underscore the potential advantages of incorporating binaural beats into clinical practice as part of routine care, especially for procedures where sedation may be avoided. These findings are particularly meaningful, considering the risks associated with sedative medications as well as health care needs that require cost-effective, patient-centric solutions.
Many people may need to know what binaural beats are and their applications in medical procedures. When first introduced, binaural beats may seem unusual, meaningless, or discomforting to listeners. Therefore, it is essential to inform patients about the potentially unusual and different nature of binaural beats before using them to reduce anxiety and pain. In this way, patients can be better prepared and more willing to listen to binaural beats.
Garcia-Argibay et al. found in their meta-analysis that binaural-beat exposure has a medium, significant effect on reducing anxiety levels, suggesting that longer exposure periods are more effective. 10 Furthermore, studies such as those by Wang et al. demonstrate the efficacy of nonpharmacological interventions like binaural beats in reducing preoperative anxiety and postoperative pain, respectively. 19 Tani et al. also support the effectiveness of binaural beats in enhancing patient comfort during colonoscopy procedures. 20 Our study provided the first comprehensive analysis of binaural music therapy’s role in endoscopy.
The utilization of analgesia and sedation is associated with cardiovascular complications. Reducing their use could improve the safety of procedures. In the study conducted by Ristankare et al. with 180 patients undergoing colonoscopy, in the group sedated with midazolam, lower blood pressure and blood oxygenation (SaO2) were observed compared to the control group without sedation. 21 In the study conducted by Kliempt et al. on 76 patients undergoing surgery with general anesthesia, it was shown that the group listening to binaural music required a lower dose of fentanyl compared to the control group. 22 Currently, the cost of the endoscopic procedure does not include the cost of anesthesia-delivered propofol sedation, which can vary from $150 to $1500 per case. 23 Therefore, binaural beats can be used in low-risk procedures such as endoscopy. In addition, further studies are needed to explore the use of music therapy in gastrointestinal endoscopic procedures such as upper gastrointestinal endoscopy, colonoscopy, diagnostic endoscopic retrograde cholangiopancreatography, and endosonography.
This study was a randomized clinical trial, which is its strength. However, it also had some limitations. First, neither the patient group nor the gastroenterologists performing the procedure were blinded to the group allocation. This lack of blinding may introduce potential bias regarding the effectiveness of the intervention. Second, we could not compare our results with other studies because no prior study has been conducted in patients undergoing upper gastrointestinal endoscopy involving preprocedure binaural beat music exposure. However, in many studies in various medical specialties, such as dentistry, urology, pulmonary medicine, and ophthalmology, statistically significant results (p < 0.05) in STAI or VAS anxiety scores, as in our study, have been observed regarding the anxiolytic effect of binaural music. 12 –14,24 Therefore, we recommend that similar studies be conducted in the future. Third, there is no clinically accepted score for evaluating patient tolerance to endoscopy. As a result, we developed a measurement scale based on the number of retches in this study. Fourth, our study did not include a patient population listening to non-binaural music. Therefore, we could not compare the effects of binaural music with other types of music.
Conclusion
This randomized controlled trial conducted at Abdurrahman Yurtaslan Oncology and Training Research Hospital demonstrates conclusively that binaural beat therapy can significantly lower anxiety among patients undergoing upper gastrointestinal endoscopy. This study demonstrated that patients exposed to binaural beats experienced greater reductions in state anxiety compared to the control group, as measured by STAI. These results were consistent despite no significant variation between groups in terms of demographic characteristics. Notably, binaural beats did not significantly alter physiological measures such as blood pressure or heart rate, suggesting their primary psychological effect. Binaural beat therapy was associated with greater patient satisfaction and tolerance among the group that received it, suggesting an overall improved experience and increased willingness to undergo future endoscopic procedures without sedation. This highlights its potential as an inexpensive, nonpharmacological way of improving comfort during medical procedures.
The study’s ramifications are significant when considering both risks and costs associated with pharmacological sedation. Binaural beat therapy could reduce sedative drug usage, while simultaneously decreasing risks and health care costs; further research should also be conducted to standardize binaural beat usage as well as validate the custom toleration assessment scale created specifically for this research project. Introducing binaural beat therapy into gastroenterological procedures presents an exciting breakthrough that promises better patient care and experience.
Footnotes
Acknowledgments
The authors are grateful to the participants for their involvement in this study. Also, the authors would like to thank all endoscopy nurses and endoscopy secretaries.
Authors’ Contributions
S.D.: Conceptualization, methodology, performing endoscopic procedures, validation, investigation, and writing—original draft; S.S.: Performing endoscopic procedures, data collection, and formal statistical analysis. Both the authors have approved the final version of the article.
Author Disclosure Statement
The authors report there are no competing interests to declare.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.