
Abstract
Introduction:
Mindfulness-based interventions (MBIs) are effective in improving mental health outcomes, including depression, anxiety, and post-traumatic stress disorder (PTSD). However, research on how MBIs have been tailored for racial and ethnic minoritized communities is limited. To address this gap, this scoping review utilizes the Ecological Validity Framework to systematically explore cultural adaptations in MBIs for communities of color. Concurrently, this review examines the effectiveness of culturally adapted MBIs.
Methods:
Following PRISMA guidelines, the authors conducted a search on MEDLINE, PsycINFO, and Embase databases from 2010 to 2023. Inclusion criteria required studies to be published in English, accessible in full-text, and peer-reviewed, focusing primarily on communities of color or diverse non-White populations (comprising 75% or more of the sample). Exclusion criteria were studies primarily centered on behavioral interventions other than MBIs, studies lacking primary outcomes, and studies not explicitly addressing cultural adaptations.
Results:
Search results identified 371 publications, 13 of which met the inclusion criteria. The most frequently reported cultural adaptations were surface-level adaptations, which can enhance the relevance of MBIs by modifying the language, content, format, or intervention delivery. MBIs with surface-level adaptations reported significant improvements in mental health outcomes, including depression, anxiety, and stress levels.
Conclusion:
Findings from this review indicate that culturally adapted MBIs for communities of color could potentially make them more relevant and acceptable. Surface-level and deep structure adaptations are both necessary to ensure MBIs are responsive, relevant, and sustainable across diverse contexts and populations.
Introduction
Mindfulness-based interventions (MBIs) have been shown to protect against the adverse effects of stress and improve a range of mental health symptoms, including depression, anxiety, and trauma 1 –3 MBIs may be particularly useful for ethnic/racial minorities who face unique stressors such as racial discrimination and trauma exposure, factors linked to higher risks of lifetime PTSD, 4 and lower psychological well-being 5 that ultimately contribute to health disparities. 6,7 By addressing the psychological and physiological response to both proximal and distal stressors, mindfulness practices may offer unique benefits in improving stress reactivity and increasing self-compassion toward these systemic/environmental experiences. 8
Socio-economically disadvantaged, racial/ethnic minority adults that engage in mindfulness practice report various positive outcomes, including improved anger management, enhanced control over thoughts and emotions, increased awareness and focus, and a greater sense of relaxation and calmness in daily life. 9 As Black adults in particular often report turning to religion and spirituality for coping with stress, including race-based stressors, 10 MBIs may be relevant by aligning with spiritual and religious practices such as prayer, meditation, sitting in stillness, and being in community with others. 11 In addition, these interventions may provide a cost-effective, group-based approach that can be integrated into various settings and require less training. 3 Indeed, research findings indicate that MBIs maintain a weighted mean attrition rate of 22% comparable to other active interventions when administered to diverse populations. 12 In turn, MBIs may serve as a viable alternative for individuals faced with challenges with cognitive-behavioral approaches. 13
Despite these reported benefits, previous studies on MBIs have primarily been tested on highly educated, employed, and White populations. 8 As such, research is limited on MBIs for racial and ethnic minoritized communities. 14 To date, only one meta-analysis has examined the effectiveness of MBIs on health outcomes for communities of color. Sun et al. 12 conducted a meta-analysis comprising of 24 samples from randomized controlled trails (RCTs) with a total of 2156 participants (94.4% African American, Asian American, and Latinx/Hispanic individuals) and found that MBIs had a minimal effect size (g = 0.11) compared to active controls and a modest effect size (g = 0.26) compared to inactive controls (false discovery rate corrected p = 0.002 and p = 0.007, respectively). This review provides evidence of modest effectiveness of MBIs in communities of color when compared to control groups.
However, researchers have identified several challenges in engaging communities of color in MBIs, including the appropriateness of language/content material, limited consideration of their lived experiences, and mistrust toward health care providers. 8 Moreover, the content of MBIs often center on White culture, experiences, and values, which may reduce their relevance and applicability for racial/ethnic minority populations. 8 Therefore, further research is needed to examine how MBIs can potentially address these challenges and broaden their relevance to diverse populations and settings to meet these specific needs.
One way to enhance the acceptability, feasibility, and effectiveness of MBIs for diverse populations is to incorporate cultural adaptations into these interventions. 15,16 Recent studies have demonstrated that culturally tailored MBIs are effective in enhancing mental health outcomes across various populations. 13,17 –19 These findings suggest that culturally adapted MBIs may have the potential to reduce disparities in mental health outcomes among communities of color. However, little is known about the specific types of adaptations utilized in MBIs, the underlying rationale for their implementation, and the theoretical frameworks guiding the adaptation process. 19 –21 While Sun et al. 12 found that most studies in their meta-analysis included some adaptation, only two explicitly incorporated cultural adaptation strategies, though the specific types were not detailed. Understanding how and when researchers culturally tailor MBIs is crucial for directing future efforts toward developing culturally relevant approaches that yield better outcomes for communities of color. 8,22
Cultural adaptations are systematic modifications to evidence-based treatments or interventions. Cultural adaptations can be defined as “considering language, culture, and context (e.g., socioeconomic status, acculturative stress) in a way that is compatible with the client’s cultural patterns, meanings, and values.” 23 To systematize cultural adaptations, researchers have identified core components of an intervention that may be modified to better consider the cultural values and lived experiences of diverse communities. These components have been integrated into models or frameworks that serve as guides to describe a specific approach and act as a point of reference to assess how well an adaptation works to meet a population’s specific needs. 24
To this end, Bernal et al. 23 developed a framework known as the Ecological Validity Framework (EVF). This framework consists of eight dimensions (language, persons, metaphors, constant, concepts, goals, methods, context) in which an intervention may be adapted to be culturally congruent with a client.;The EVF provides a guide for researchers to identify the specific adaptations in existing interventions that align with the experiences and customs of communities of color. By using this framework to assess cultural adaptations in MBIs, researchers can identify whether MBIs have been culturally adapted, the types of adaptations incorporated, and which components have not been attended to in the MBI literature. Table 1 presents an overview of the eight dimensions and potential examples within MBIs.
Cultural Adaptation Dimensions of the Ecological Validity Model
Adapted from the Ecological Validity Model (Bernal et al. 23 ).
MBI, mindfulness-based interventions.
Importantly, cultural adaptations of empirically supported treatments have shown enhanced efficacy among racial/ethnic minority populations. 25 Griner and Smith 26 conducted a meta-analysis comparing culturally adapted interventions to traditional mental health approaches. While their review did not specifically focus on mindfulness interventions, it assessed the effectiveness of a wide range of mental health interventions, encompassing both individual and group therapies. Their review comprised 76 studies with 25,225 participants, predominantly female (55%) and ethnically diverse (31% African American, 31% Hispanic/Latino American, 19% Asian American, 11% Native American, 5% European American). This meta-analysis found an overall effect of culturally adapted mental health interventions, exhibiting random effects weighted average moderate effect sizes across all 76 studies (d = 0.45) and across 62 studies with experimental or quasi-experimental designs (d = 0.40). Importantly, they found a moderate effectiveness of interventions conducted with groups of same-race participants (d = 0.49) compared to those with mixed-race participants (d = 0.12), suggesting the utility of tailoring adaptations to specific racial/ethnic groups for optimal outcomes. The meaningful impact of culturally adapted interventions highlights the importance of identifying effective strategies for tailoring MBIs for communities of color.
The lack of a standardized approach for tailoring interventions and insufficient documentation of these adaptations present challenges for researchers aiming to effectively modify existing interventions. 21,27 Currently, there is a paucity of research exploring the specific types of cultural adaptations in MBIs, with only one study focused on Hispanic populations. 19 To address this gap in the literature, this study aims to conduct a scoping review to systematically describe and report the types of cultural adaptations in MBIs tailored for communities of color, utilizing the EVF. A secondary aim was to report efficacy/effectiveness outcomes of culturally adapted MBIs. This review seeks to advance understanding of tailored approaches and content utilized in MBIs for communities of color. The findings from this review have implications for researchers aiming to develop more culturally sensitive interventions for communities of color to enhance their acceptability, feasibility, and effectiveness.
Methods
To achieve the study aims, the authors conducted a scoping review, a methodology well-suited for addressing broad research questions and identifying gaps in knowledge on a particular topic. 28 The search strategy was guided by the research questions: “What types of cultural adaptations in MBIs have been implemented within communities of color?” and “What effects do cultural adaptations have on MBI outcomes.” Primary search terms, utilizing appropriate Boolean operators, were entered into three databases (PubMed, PsychINFO, and Embase) to retrieve publications, as outlined in Table 2. To prioritize recent research, the authors restricted the search to peer-reviewed studies published between January 2010 and February 2023. In addition, the references of included studies were examined for relevant studies.
Database Search Terms and Results
The database search was conducted on March 13,2024 and included publications from 2010 to 2023.
To ensure relevance, studies had to meet the following inclusion criteria: include mindfulness meditation as core component, published in English, accessible in full-text, peer-reviewed, and focus primarily on communities of color or diverse non-White populations (constituting ≥75% of the sample). This threshold is consistent with previous reviews of MBIs among communities of color 11,12 and represents the tipping point for group homogeneity in culture and social norms. 29 Exclusions criteria were studies primarily focused on behavioral interventions other than MBIs (e.g., cognitive behavioral therapy (CBT), acceptance-based behavioral therapies, dialectal behavioral therapy), interventions lacking primary outcomes, and interventions that did not explicitly address cultural adaptations.
The selection process followed PRISMA guidelines 30 and a flow chart (Fig. 1) was employed to illustrate the record screening process and its outcomes. To ensure accuracy, all records from the initial search were imported into Zotero.org, a reference management software, to identify and remove duplicates. The lead author reviewed the remaining records and excluded irrelevant records based on title and abstract. Records that were unclear if eligible based on title and abstract were included in full text review. Full texts of relevant studies were thoroughly screened, and relevant data were extracted from studies that met the inclusion criteria. Throughout this selection process, the lead author worked closely with the senior author, a clinical psychologist who is highly experienced in mindfulness research and facilitation, to ensure mutual agreement on whether studies met inclusion criteria.
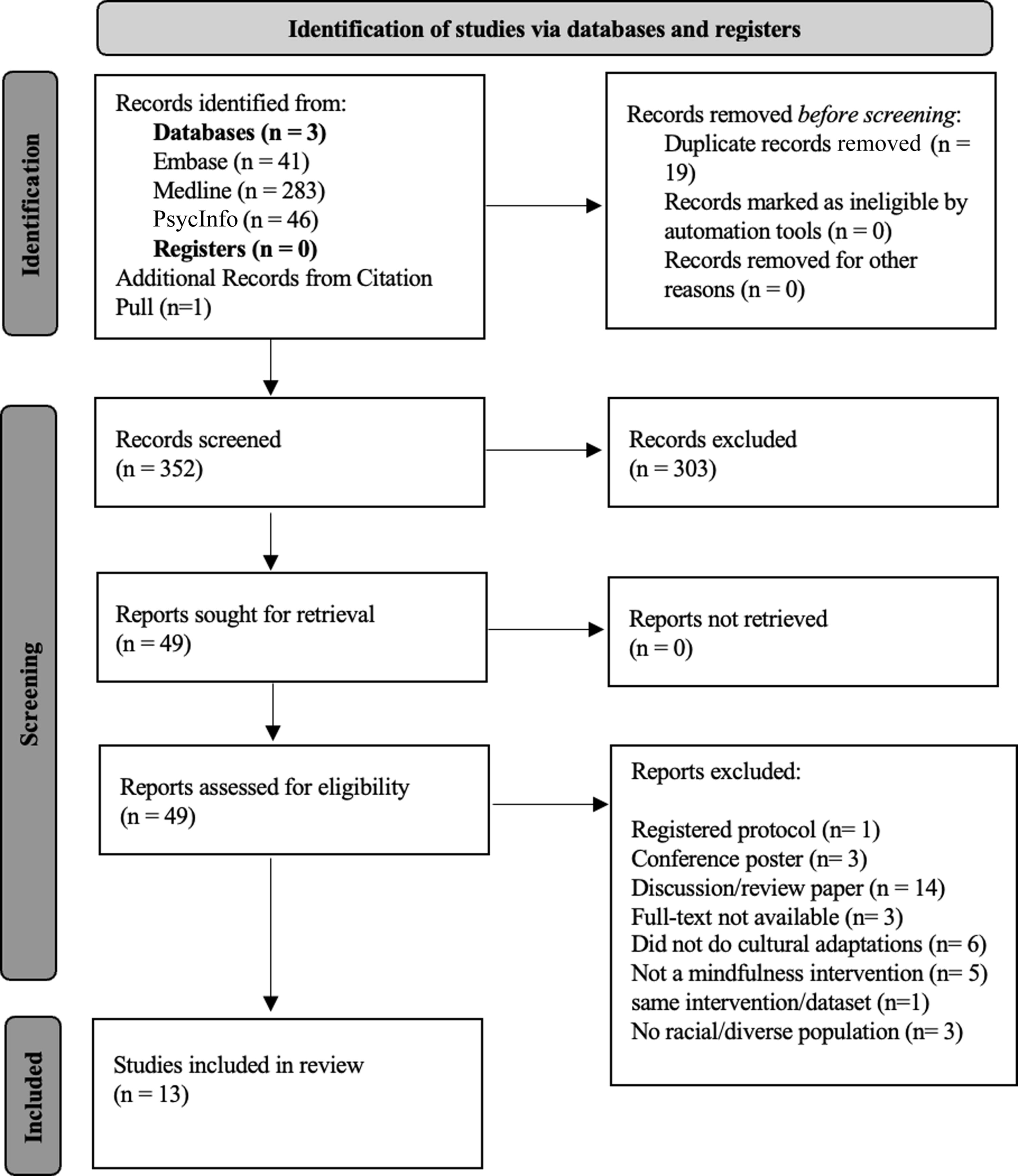
shows the authors’ study flow for selecting eligible studies that are included in this scoping review. The study selection process was conducted using the PRISMA-ScR framework described by Tricco et al. 30 PRISMA-ScR, Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews.
To evaluate cultural adaptations, various frameworks were considered, including the Cultural Sensitivity Model, 31 New Framework for Cultural Adaptation, 32 and the Cultural Treatment Adaptation Framework. 33 However, the EVF was selected for its widespread recognition in intervention research and previous use in assessing cultural adaptations across diverse settings. 19,34 –36 Using Microsoft Excel (Version 2019), the lead and senior authors designed a data-charting form based on the EVF framework to identify and extract relevant adaptations. The lead author independently coded the identified cultural adaptations and reviewed the adaptation selections with the senior author. Extracted data included study design, intervention details, sample characteristics, types of adaptations, and primary outcomes. Cultural adaptations were summarized and reported in descending order of frequency (Supplementary Data S1).
Results
The initial search generated 371 publications for review. After removing duplicates and irrelevant articles, the authors identified 49 independent peer-reviewed publications that met the initial inclusion criteria based on abstracts. Upon further review, 36 papers were excluded for the following reasons: registered protocol (n = 1); conference posters (n = 3); discussion and review papers (n = 14); full-text was not available (n = 3); did not contain cultural adaptations (n = 6); did not have a mindfulness intervention (n = 5); target group was not a racial/diverse population (n = 3); secondary analysis using same intervention/dataset (n = 1). The final sample consisted of 13 publications to review. The search procedure is outlined in the review flowchart (Fig. 1).
In total, 13 studies were included in this scoping review. Table 3 summarizes the key characteristics of the studies included. Among these, the most utilized cultural adaptation reported were method adaptations to MBIs (n = 10, 76.9%). Specifically, multiple studies recommended various ways to enhance the accessibility of mindfulness intervention classes, such as shortening their duration, 13,37,42,44 providing meal and/or transportation vouchers to participants, 13,37,42 offering childcare services. 18,39,40,42
Key Characteristics of Included Studies
MBI, mindfulness-based interventions; MBSR, mindfulness-based stress reduction; MENA, Middle East North Africa; RCT, randomized control trial.
Watson-Singleton et al. 46 also adopted their intervention into a mobile application to increase accessibility among Black/African American participants. Furthermore, Blignault et al. 39 uploaded audio of intervention content to various media platforms at no cost to viewers. To encourage engagement, Hartwell et al. 42 suggested that a 30-min settling-in period before the classes could promote community building, whereas Proulx 43 provided a 30-min debriefing session after each class to foster a collaborative approach to addressing the specific needs and stressors of Black/African American older adults. To enhance the quality of interaction between participants and the psychologist, Elimimian et al. 41 restricted class sizes to a maximum of 10 participants.
Another common adaptation reported was content adaptations (n = 8; 61.5%). Specifically, MBIs adapted for Black/African American/Latinx populations included themes on relieving trauma, dealing with anger, and community healing. 17,42,45 Amaro et al. 17 and Trombka et al. 45 described the need for trauma-informed content (e.g., acknowledging trauma and daily stress from lived experiences; language that emphasizes personal choice) when working with racially diverse populations. Ruiz-Iniguez et al. 44 recommended incorporating techniques rich in cultural musical sonorities with Cuban clients, as music plays a significant role in Cuban culture. Additional content adaptations for racial/diverse populations included addressing religion and/or spirituality, 18,39,40,46 and cultural practices that may aid in the learning of mindfulness. 44
Language adaptations were also commonly made (n = 8; 61.5%). Specifically, Watson-Singleton et al. 46 employed culturally familiar terminology in their mindfulness mHealth application to alleviate stress among African Americans. For example, the authors used “mindful” instead of “meditation” in their app and practices, considering African American women’s discomfort with the latter owing to its conflict with their religious practices, such as Christian prayer. Amaro et al. 17 recommended making literacy changes to enhance intervention acceptability for ethnically diverse low-income women. Furthermore, Bhambhani et al. 37 reported that group leaders were mindful of using language that was easy to understand given various levels of English proficiency among participants. Some studies translated the intervention entirely into different languages, including Arabic and Bangla, 18,39,40 Portuguese, 45 and Spanish. 41
Some studies also reported persons adaptations (n = 4, 30.8%). Blignault and colleagues 18,40 described using female facilitators with female participants, whereas Bigelow 46 used group facilitators that self-identified as transgendered when working with transgender participants. Watson-Singleton et al. 46 also reported using Black/African American facilitators in their mHealth intervention with a predominately Black/African American population.
A few studies also made context adaptations (n = 3, 23.1%). Specifically, Amaro et al. 17 suggested adjusting the length/style of body scan and mindfulness-based stress reduction (MBSR) exercise to reduce potential interference from traumatic experiences when working with diverse ethnic women with a history of trauma. Similarly, Bhambhani and colleagues 37 addressed contextual factors, such as the impact of race-based stress, marginalization within power structures, personal agency in group activities, and the importance of individual empowerment through appreciation of their resilience. Burnett-Zeigler et al. 13 implemented adaptations to an MBSR intervention within a federally qualified health left setting, targeting a population of Black/African American women with depressive symptoms. Their intervention included offering free, abbreviated classes, and streamlining teacher training to enhance feasibility.
One study incorporated metaphor adaptations (n = 1, 7.7%). Specifically, the authors utilized culturally relevant images, poetry tailored for Black/African American women, and poetic reflections from Black/African American poets 13. Importantly, none of the studies (n = 0) referenced concept or goal adaptations to MBIs.
Quantitative findings
A secondary aim of this review was to investigate quantitative outcomes from the reported studies, with 10 studies (76.9%) providing data on quantitative outcomes. Among the studies incorporating surface-level adaptations to MBIs, results demonstrated significant reductions in stress (n = 7; 70%), depressive symptoms (n = 6; 60%), anxiety outcomes (n = 5, 50%), and trait anger (n = 1; 10%).
Specifically, Blignault et al. 39 tailored their intervention with language, content, and method adaptations and observed a significant decrease in psychological distress from baseline to post-intervention, as well as from post-intervention to follow-up (all p < 0.001). They also reported significant decreases in depression scores across three time periods: baseline to 5 weeks (p < 0.02), baseline to 12 weeks (p < 0.001), and 5 weeks to 12 weeks (p < 0.004), along with a significant decrease in anxiety scores from baseline to the 12-week follow-up (p < 0.01).
In subsequent studies, Blignault et al. 18,40 adapted their intervention with language, persons, content, and method adaptations, resulting in significant improvements in stress (p < 0.001), depression (p < 0.001), and anxiety scores from baseline to post-intervention (p < 0.01). Blignault et al. 18 also observed significant improvement in psychological distress among both Arabic and Bangla speakers post-intervention (p < 0.001). Amaro et al. 17 reported that language, content, and context adaptations led to a decline in perceived stress scores among all participants, with a higher rate of decline observed among those with a higher dose of the intervention (p < 0.05). In addition, Elimimian et al. 41 found that their MBI containing language and method adaptations led to significant improvements in depression and anxiety scores from baseline to 24 months (p = 0.04).
Watson-Singleton et al. 46 found significant improvements in perceived stress levels with a medium effect size (p < 0.004, d = 0.73) after two weeks of their mindfulness app-based intervention, which incorporated language, persons, content, and method adaptations. Burnett-Zeigler et al. 13 reported metaphor, methods, and context adaptations to their MBI and found a significant decrease in stress with large effect sizes from baseline to 8 weeks post-intervention (p = 0.01, d = 1.06) and from baseline to 16 weeks (p = 0.02, d = 1.02), along with a significant decrease in depressive symptoms from baseline to 16 weeks (p = 0.04, d = 0.84). Similarly, Ruiz-Iniguez et al. 44 tailored their MBIs with content and method adaptations, reporting significant stress reduction and large effect sizes from baseline to post-test (p < 0.001, d = 1.08) and baseline to follow-up (p < 0.001, d = 0.95). Trombka et al. 45 adapted their intervention with language and content adaptations and found a medium-to-large effect size in reducing depression symptoms (p < 0.001, d = 0.67) and medium effect size in decreasing anxiety symptoms (p = 0.011, d = 0.48). Finally, Hartwell et al. 42 tailored their intervention with content and method adaptations, resulting in decreased trait anger from baseline to post-intervention; however, the sample size was too small to yield statistically significant results.
Discussion
This study examined the frequency and types of cultural adaptations to MBIs, and efficacy/effectiveness outcomes, for communities of color using the EVF. This scoping review identified 13 studies adapted for communities of color, with half of the studies focused on Black/African American populations. Notably, all 13 studies included at least one surface-level adaptation, while 11 studies incorporated multiple adaptations. Results indicate that MBIs with surface-level cultural adaptations are effective in improving health outcomes, including stress, depression, and anxiety.
Results indicated that the most frequently reported cultural adaptations were methods that focused on the techniques used to deliver the intervention. Specifically, ten studies incorporated adjustments to the practical and logistical aspects of the intervention to cater to the unique needs of a cultural group. Other prevalent adaptations involved changes to the intervention’s content (e.g., addressing trauma, daily stressors, religion/spirituality, etc.) and language (e.g., culturally relevant terminology to align with the client’s culture, values, traditions, or language). The least referenced cultural adaptations were in goals and concepts, which were not explicitly mentioned in any of the studies.
These findings suggest a tendency to focus on the logistical and procedural aspects of an intervention when tailoring MBIs to be culturally responsive. While method adaptations may not necessarily involve cultural content itself, they are still informed by cultural knowledge of specific community needs. Method adaptations are particularly important given that the effectiveness of an intervention is not solely dependent on its core content components but also on its delivery and implementation. Thus, considering logistical and methodological aspects may enhance the accessibility of the intervention by removing potential barriers to participation and promoting greater engagement.
In addition, content adaptations that provide clients with additional material/information relevant to their cultural background are crucial. Researchers might consider how cultural practices contribute to the acquisition of mindfulness skills. For example, focusing on sound-based meditations when working with Cuban clients may be beneficial, which aligns with the high musical sonorities in Cuban culture. 44 Similarly, connecting mindfulness to themes of religion and spirituality may hold cultural significance for Black/African American communities. 11
Language adaptations were also frequently reported, which prescribes that the intervention is congruent with a client’s linguistic preferences. There is a general agreement that an intervention should be delivered, or at the minimum, be translated into the preferred language of the client. Language adaptations are reported as essential “surface-structure changes” that optimize MBI’s effectiveness for diverse populations. 15 However, Bernal et al. 23 argue that language adaptations should also be relevant to one’s dialect, particularly with “inner city, regional, or sub cultural groups.” Watson-Singleton et al. 46 and Amaro et al. 17 both demonstrated the use of culturally relevant terminology in their adapted MBIs for diverse populations. Although literacy changes that consider a community’s vernacular may increase the intervention’s accessibility for clients, they do not address deeper ideological issues that may be relevant to a client (e.g., sexism, homophobia/transphobia, racism, ableism).
Similarly, person adaptations do not necessarily incorporate these ideological, cultural, or contextual factors into the intervention. This adaptation simply requires an “identity match” between the client and the individual administering the intervention. This match can be based on ethnicity, race, gender, sexual orientation, and/or other characteristics. Although a simple and feasible adaptation to MBIs, it does not require the clinician/researcher to address cultural factors in treatment. Also, it may not always be pragmatic for the instructor to consistently match the client’s identities. Given the lack of diverse MBI instructors and the multiple barriers to instructor training, achieving a perfect match between instructor and participant identities may be challenging, especially within the group format of MBIs. 47 Nonminoritized MBI instructors can enhance their cultural competence by actively educating themselves about participants’ backgrounds and engaging informally with them before or after group sessions, such as attending community events and staying informed on relevant news impacting the community. By cultivating cultural humility, instructors can adapt their teaching approaches to be more inclusive and responsive to diverse needs. 48
Understanding a client’s cultural background should also prompt consideration of contextual factors that may influence an intervention’s acceptability within a specific diverse community. Contextual factors refer to the broader social, cultural, and environmental aspects that shape an individual’s experiences within their community. 23 These contextual factors can include various elements such as historical experiences, socioeconomic status, access to resources, and cultural mistrust in services that may play a role in shaping individuals’ engagement with MBIs. 22 However, only few of the reviewed studies mentioned tailoring an intervention based on the context in which participants were seeking MBIs. 13,17,37 To address this concern, researchers could leverage qualitative research to identify participant-specific factors impacting intervention acceptability, thereby enhancing treatment utilization. 38,43
Concept adaptations do amalgamate a client’s contextual factors and cultural background into treatment. Concept adaptations involve cultural adjustments to the case conceptualization process, including the psychological model and the process of change used to understand a client’s presenting problems. 19 For instance, Iacono 49 integrates minority stress theory into the case conceptualization process to inform the use of a mindfulness-based affirmative approaches for LGBTQ youth. This integration aims to enhance resilience and coping skills against discrimination (e.g., homophobia/transphobia, microaggressions). Importantly, none of the studies directly reported the use of concept adaptations. This may suggest a tendency for researchers to opt for “surface-level” modifications to interventions rather than deep conceptual changes that necessitate a more deliberate approach, such as theory that describes the underlying mechanisms of change.
It is important to note that concept adaptations can be particularly challenging for researchers to achieve. 23 This is because the effectiveness of MBIs relies on core elements such as nonjudgmental awareness of the present moment and acceptance. 50 However, introducing “deep-structure” concept adaptations that may modify these core elements can present methodological challenges and potentially undermine treatment fidelity. 51 Given these complexities, researchers have suggested drawing from best practice methods for behavioral change interventions, deciding when and how to adapt MBIs based on considerations around necessity, safety, feasibility, acceptability, effectiveness, and scalability. 20 For example, Crane et al. 52 developed a comprehensive guide to identify the active elements of MBIs and discern components that can be flexible based on context, settings, and target population. Researchers should utilize these established frameworks and cultural adaptation process models to guide decision-making when integrating changes into their interventions. 53
In addition, metaphor adaptations were one of the least utilized cultural adaptations. Culturally relevant imagery and symbols may help prescribe powerful meanings that are significant to the cultural values of communities of color. However, only one study referenced the use of culturally relevant imagery. Burnett-Zeigler et al. 13 mentioned using Black/African American imagery and poetry tailored for Black/African American women in a community-based setting. Previous literature suggests that terms and imagery of “mindfulness” should match the cultural groups’ norms and be translated further to promote the accessibility of the intervention. 54
Moreover, using cultural knowledge to inform treatment goals is critical for communities of color. Yet, none of the studies explicitly mentioned adaptations to goals for MBIs. The omission of explicit goal adaptations may reflect the perception that the core goals of MBIs (e.g., stress reduction, improved psychological well-being) are universally applicable and may not require modification to address cultural or contextual factors. It is also important to note that MBIs are educational programs that focus on enhancing self-awareness and providing mindfulness skills for daily life challenges, differing from traditional psychotherapy. 50 Consequently, specific treatment goals may be less prominent in the context of MBIs. Instead, participants may engage in the goal-setting process at the beginning of an MBI to identify personal focus areas for their mindfulness practice. 55
Limitations
The findings of this review should be taken in the context of a few limitations. First, cultural adaptations were coded based on alignment with the eight dimensions outlined in the EVF. By focusing solely on the dimensions presented by Bernal et al., this scoping review might have overlooked other potential cultural adaptations that do not fall within those specified dimensions. Second, the inclusion criteria focused on English-language studies, possibly excluding adaptations in other languages. Given the multiple adaptations within each of the reviewed studies and the absence of control conditions in the majority of cases, the authors faced limitations in their ability to make claims about the specific additive impact of each adaptation. Finally, while the authors chose a scoping review approach, future meta-analyses could offer a comprehensive overview of the effect of culturally adapted MBIs.
Conclusions
Despite the limitations, this review highlighted the potential of culturally adapted MBIs, which already have a strong evidence base, to address the specific needs of diverse populations, particularly among Black/African American and Hispanic/Latinx communities. In addition, quantitative results found that MBIs containing cultural adaptations appear efficacious to varying degrees for communities of color. Notably, the authors highlight the role surface-level adaptations, which can enhance the relevance of MBIs by modifying the language, content, format, or delivery of the interventions. However, surface-level adaptations may not fully address the deeper structural and contextual factors influencing the health and well-being of communities of color. Tailoring MBIs may necessitate a “top-up” approach that involve deeper structural changes consistent with specific cultural values, beliefs, and practices of a community. Integrating both types of adaptations can ensure responsive, sustainable, and culturally relevant MBIs across diverse contexts. This adaptation process should be guided by frameworks to maintain treatment fidelity while considering contextual and population-specific factors.
Future directions
Further research is required to thoroughly investigate factors influencing the acceptability and relevance of MBIs among diverse populations. To better understand the effectiveness of culturally tailored adaptations to MBIs, researchers should also compare them directly to active interventions that have not been adapted. Finally, there is a need for more systematic and meta-analytic reviews using different cultural frameworks and models to identify other appropriate cultural adaptations to MBIs.
Footnotes
Acknowledgment
The authors would like to give a special thanks to Jennifer Martinez, PhD for reviewing earlier versions of this article.
Authors’ Contributions
A.M.: Conceptualization (lead); formal analysis (lead); writing—original draft (lead); review and editing (equal). I.B.Z.: Conceptualization (supporting); writing—original draft (supporting); writing—review and editing (supporting); supervision (lead).
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
The authors received no external funding.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.