
Abstract
Objectives:
Chronic nonspecific neck pain (CNNP) is prevalent among health care workers, with particularly high rates among nurses. Nurses experiencing CNNP often report decreased job satisfaction, increased absenteeism, and reduced productivity. In recent years, nonpharmacologic approaches have gained attention as effective treatments for the management of CNNP, with exercise and manual therapies representing two of the most common. Early evidence shows that multimodal treatments may be more effective than unimodal strategies. The purpose of this current study was to assess the feasibility and observe the clinical outcomes of combined multimodal chiropractic care (MCC) and Tai Chi (TC) for CNNP in nurses.
Methods:
A single-arm mixed-methods pilot trial was conducted including 16 weeks of MCC and TC in nurses with self-reported CNNP. Feasibility outcomes were recruitment, retention, and adherence to the interventions. Clinical outcomes of interest included neck pain and related disabilities. Secondary outcomes of interest were functional, affective, and work-related performance. Qualitative interviews were also conducted.
Results:
Of the 59 screened, 36 met the eligibility criteria, and 21 were enrolled. The retention rate was 71.4%, and adherence rates were 85.3% for MCC and 62.5% for TC classes. Multiple pain and disability-related outcomes exhibited modest improvement from baseline to 16-week follow-up. Qualitative analysis identified six emergent themes: (1) neck pain being an inherent part of nursing, (2) nurses push through their pain, (3) MCC relieves pain and is instructive for preventing pain, (4) TC provides overall relaxation, (5) both interventions increased body awareness and improved posture, and (6) scheduling difficulties were a key obstacle for participating.
Conclusions:
Observed reductions in neck pain and disability suggest the potential utility of combined MCC and TC interventions for managing CNNP. Along with qualitative feedback regarding facilitators and barriers to participation, the findings support and inform a future randomized trial evaluating the combined benefits of MCC and TC for CNNP in nurses.
Clinical Trial Registration #NCT06523036.
Introduction
Chronic nonspecific neck pain (CNNP) refers to symptoms arising from benign neuromusculoskeletal sources and lasting at least 3 months. Estimates of the prevalence of CNNP range from 30% to 50% in the general population. 1 –4 The impact of CNNP is especially burdensome for nurses. Up to 45% of nurses report experiencing work-related neck pain annually. 5 Despite its prevalence, neck pain is often overlooked and underreported, particularly in comparison to back pain. 6 In addition to physical discomfort, CNNP often has adverse functional, psychological, and social consequences. Nurses experiencing CNNP report decreased job satisfaction, increased absenteeism, and reduced productivity. 7 –10 CNNP in nurses is also associated with a higher attrition from the workforce, 11,12 negatively impacting patient outcomes and imposing substantial economic consequences. The average hospital in the United States loses between $5.2 and 9 million per year in nursing-related attrition costs. 13
The causes and consequences of CNNP are complex and best viewed from a biopsychosocial perspective, in which pain interplays with psychosocial factors, 14,15 supporting the need for multimodal treatment approaches. In recent years, nonpharmacologic approaches for pain have gained attention as being effective. 16 Multimodal chiropractic care (MCC) and Tai Chi (TC) are two promising interventions that have individually shown promise in managing CNNP, making use of distinct yet complementary mechanisms. 17,18
MCC, a noninvasive and drug-free approach, combines manual therapies, education, and movement-based therapies to alleviate pain and improve musculoskeletal function. 2,19 Evidence supports the use of components of MCC, such as spinal manipulation or mobilization, in improving CNNP. 2,19 TC, a mind–body activity, incorporates slow movements, breath training, and multiple mindfulness-related techniques (e.g., mental focus, heightened body awareness, and imagery). 20,21 TC has demonstrated benefits for chronic musculoskeletal pain, including CNNP, 18,22 fostering improvements in postural awareness, strength, and flexibility while reducing key causes of chronicity, rumination, catastrophizing, and perceived stress. 23 –25 However, the combined effects of chiropractic care and TC have not been explored. Given the multiple and complementary mechanisms underlying these two interventions, the combination of these modalities could have both additive and synergistic effects.
The objective of this single-arm mixed-methods pilot study was to evaluate the feasibility of combining MCC and TC training for nurses with CNNP. Hypotheses included that it would be feasible to recruit and retain nurses with CNNP in a 16-week combined intervention period, that nurses would adhere to the interventions and outcome assessment protocols, and that qualitative and quantitative outcomes would inform the potential effectiveness and design features of a future randomized trial.
Methods
Participant recruitment and eligibility
This study was approved by the Partners Human Research Committee Institutional Review Board (#2019P003845). Participants were recruited from electronic and printed advertisements throughout relevant Brigham and Women’s Hospital (BWH) clinics as well as email using BWH department lists with department manager approval. Participants who expressed interest were screened via phone for self-reported eligibility consistent with the Bone and Joint Decade Task Force grades I and II (Table 1). 27 Those eligible signed (electronically) an approved informed consent form through Research Electronic Data Capture (REDCap) 28,29 tools hosted at BWH. Study staff reviewed the informed consent document, explained all study procedures and risks, and answered questions before the participants signed the informed consent document. Eligibility criteria were confirmed by treating Doctors of Chiropractic (DCs) at the first chiropractic visit. The overall design, conduct, and reporting of this study follow the Consolidated Standards of Reporting Trials 2010 extension for nonrandomized feasibility trials 30 (Supplementary Table S1) and are reported on ClinicalTrials.gov (NCT06523036).
Study Eligibility Criteria
BWH, Brigham and Women’s Hospital.
Procedures
After the informed consent process was completed, participants were scheduled for a baseline assessment, physical examination, and first chiropractic visit at the Osher Clinical Center for Integrative Health (OCCIH). Subsequently, eligible participants were scheduled for nine additional chiropractic visits and asked to register for weekly classes at one of the two approved TC programs in the greater Boston area. Weekly classes lasted for the 16-week intervention period. After completing the 16-week intervention period, participants were asked to attend a follow-up outcomes assessment visit at the OCCIH. Baseline and follow-up assessments included a battery of standardized questionnaires, semi-structured qualitative interviews, and gait assessment.
Interventions: Chiropractic care
Enrolled participants were scheduled for a total of 10 treatments over 16 weeks. All chiropractic treatment involved a standardized protocol administered by one of the two DCs at the OCCIH. The treatment plan included appropriate elements of MCC, as described in Table 2. Treatments were customized to the participants’ clinical needs and consistent with protocols previously established for treating chronic neck pain comorbid with migraine headaches. 26,31
Key Components of Multimodal Chiropractic Care
Interventions: TC
Participants were simultaneously enrolled in weekly TC classes at one of the two community-based TC schools that were used for prior pragmatic studies. 32,33 One school taught a Wu Style TC program and the other a Sun Style. Both programs offered hour-long classes that included traditional qigong warm-up exercises emphasizing mindful repetitive stretching, breath training, and mental focus, followed by more formal practice of choreographed TC sequences. Lead instructors in both programs each had more than 25 years of training and teaching experience and were asked to teach participants as typical enrolled students, with no special study-specific modifications. Participants were offered both in-person and online options over the 16-week intervention period. Participants were also asked to practice TC for a minimum of 30 min, three additional days per week. Both schools provided materials to facilitate home practice. Compliance with this training schedule was monitored with participant-completed weekly attendance and home practice logs collected and managed through REDCap. 32,34 When attendance and/or practice logs were not submitted on time, participants were contacted by trial staff within 1 week.
Outcomes
Feasibility was assessed with respect to participant recruitment, retention, and adherence rates for chiropractic and TC interventions. Recruitment was evaluated with respect to the rate of enrollment (number of interested participants/number enrolled) and the percentage of eligible participants who consented to participate. The sample size of 21 subjects was chosen in anticipation of providing adequate data to estimate recruitment from various sources, enrollment rate, and duration of the recruitment period for future trial planning. Retention was measured by the percentage of participants who completed the 16-week intervention and follow-up measures. Adherence was measured by the percentage of intervention sessions attended by each participant. Recruitment feasibility was a priori defined as 21 participants enrolled within a 6-month period. Retention feasibility was a priori defined as 75% of participants retained throughout the 16-week intervention period. Adherence to interventions was deemed feasible a priori by 70% attendance at chiropractic visits and 60% attendance at weekly TC classes. Throughout the intervention period, participants were administered weekly REDCap surveys, delivered by email, which contained questions about TC home practice.
Adverse events were monitored at three levels: (1) questions included in weekly REDCap surveys, (2) monthly check-in call by the study staff, and (3) by clinicians and TC instructors. Any reported events were monitored and graded based on predefined criteria based on expectedness, severity, and relation to the study interventions. 26
All clinical outcomes were collected at baseline and at the 16-week follow-up visit. Clinical outcomes were obtained using standardized questionnaires comprising functional measures of pain including pain intensity (PI), Neck Disability Index (NDI), pain on movement (POM), and bothersomeness of pain (BOP). PI scores were acquired from the Patient-Reported Outcomes Measurement Information System 29 (PROMIS-29) single 0–10 numeric rating item. 35 –40 NDI scores were assessed using the 10-item questionnaire, with scores ranging from 0 to 50. 41 POM was assessed using a previously validated and reliable protocol. 42 BOP was assessed by asking participants to indicate the bothersomeness of their pain in the 7 days prior to their assessment using a 0–10 numeric rating item. 43
Additional outcomes including the PROMIS-29, Maslach Burnout Inventory (MBI), and General Self-Efficacy 6-item scale (GSE-6) were included as measures of quality of life, psychosocial health, and employee health-related outcomes. PROMIS-29 is a system of validated, highly reliable, and precise measures of patient-reported health status for physical, mental, and social well-being. 35 –40 The MBI is a widely recognized 22-item psychological inventory assessing occupational burnout. 44 It is particularly relevant in high-stress professions such as nursing and provides valuable insights into the multifaceted nature of burnout by capturing emotional, cognitive, and motivational aspects. 45 The GSE-6 is a validated instrument designed to measure individuals’ beliefs in their ability to cope with and successfully perform tasks in challenging situations. 46 It has shown correlations with work satisfaction, stress, and psychological well-being. 47 Additional collected outcomes are reported in Supplementary Table S2.
Qualitative interviews
Qualitative interviews were completed at baseline and follow-up to gain insight into participants’ interest in and experience with the trial. Semi-structured qualitative interviews focused on participants’ perceptions of neck pain, its influence on their work and personal lives, and rationale for joining the trial. Each interview was audio recorded, deidentified, and then transcribed verbatim. Using grounded theory methods for comparing categories, 48 we developed a final set of themes.
Analysis
Data analysis was carried out with R Statistical Computing Software. 49 Descriptive statistics were used to summarize patient characteristics at baseline and the feasibility of recruitment, retention, and treatment. Descriptive statistics were used to summarize each of the clinical outcomes collected at baseline, 16-week follow-up, and the change between these two timepoints. Within-group change was also assessed with Cohen’s d, a standardized effect size. 50 Data collected from participants at baseline who were subsequently lost to follow-up were not included in the final analysis.
Results
Patient flow and demographic characteristics
One hundred nurses expressed interest in participating, and 58 were screened for eligibility. Twenty-nine participants were excluded after screening. The resulting 21 individuals were enrolled in the trial (Fig. 1). Fifteen participants completed the trial intervention period and the 16-week trial visit. Baseline characteristics are summarized in Table 3.
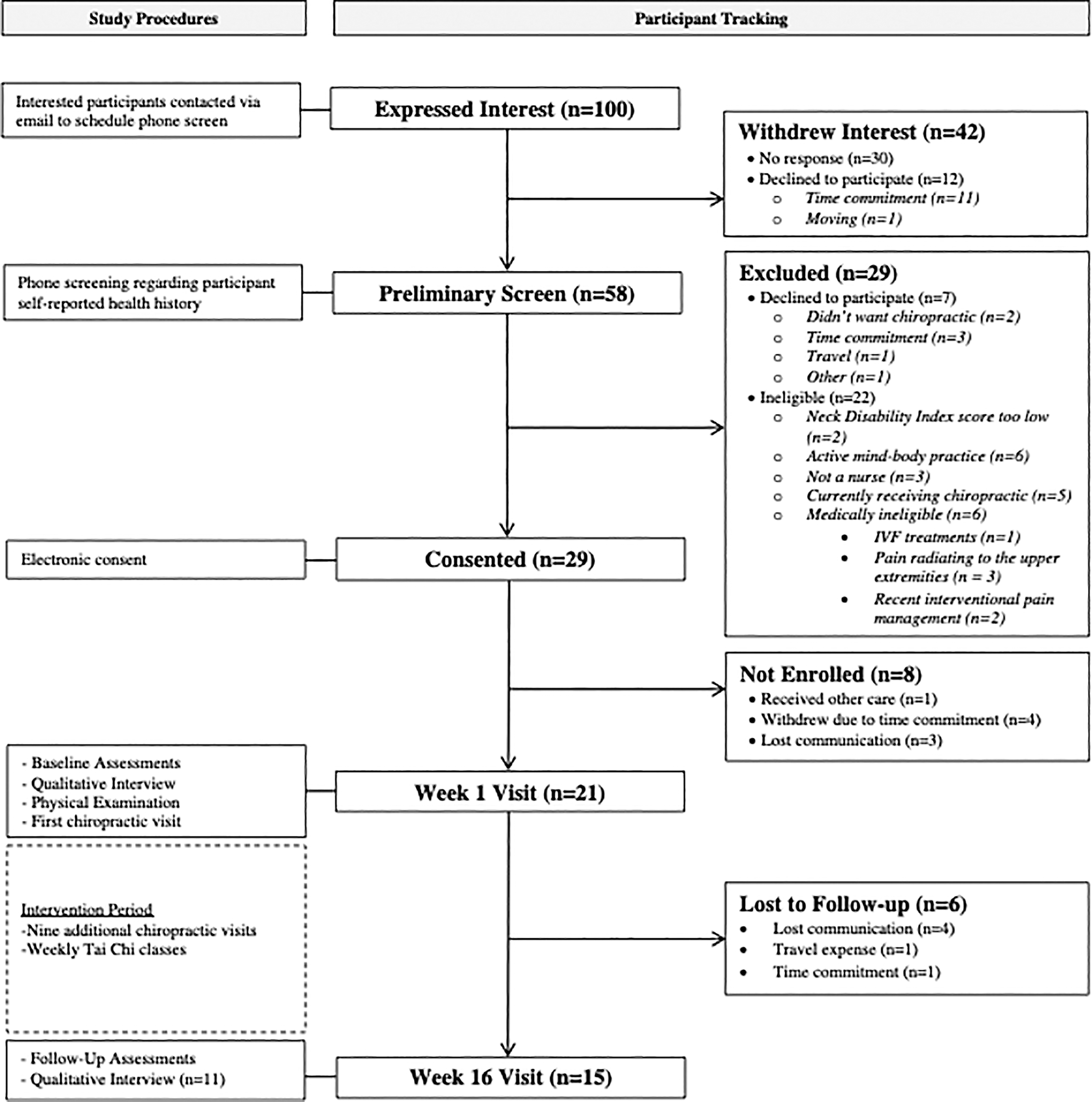
Consort diagram.
Baseline Demographics of Participants who Both Completed the Trial and were Lost to Follow-up
Note that participants who were lost to follow-up were younger, more educated, and had a shorter duration of their CNNP.
BMI, body mass index; CNNP, chronic nonspecific neck pain; IQR, interquartile range; NDI, Neck Disability Index; SD, standard deviation.
Feasibility
The a priori defined recruitment goal of 21 participants was met; however, the duration of recruitment, from September 2021 to October 2022, was longer than the 6-month target goal. Eighty-one percent of eligible participants consented to participate, and the enrollment rate was 4.76 participants per month. Participants attended a mean of 85.3% of the chiropractic visits (median = 85%, interquartile range [IQR]: 85%−100%) and 62.5% of the TC classes (median = 68.8%, IQR: 40.6%−87.5%). Two participants attended TC classes in person, while the remaining 13 attended virtually. Of the included components of MCC, manual spinal manipulation or mobilization and soft tissue relaxation/release techniques were used at 85% of visits; posture correction or spinal stabilization exercises were used at 83% of visits; stretching, strengthening, and motor control exercises were used at 71% of visits; ergonomic advice and modifications were used at 50% of visits; and education about participant conditions, including self-management advice, was used at 23% of visits. Extremity joint manipulation or mobilization and breathing or relaxation techniques were not reported during any visit (Supplementary Table S3). Participants completed a mean of 43 min (median = 45, IQR: 27–64) of TC home practice each week. About 71.4% of the recruited participants (15 of 21) completed the week 16 visit.
Adverse events
Nine total adverse events were reported during the study period, seven of which were determined to be expected and mild in severity, with five being definitely related and two being unrelated or unlikely related to the study interventions. Detailed information about the specific adverse events can be found in Supplementary Table S4. All adverse events were reported by participants through the weekly REDCap surveys.
Clinical outcomes
Results from clinical outcomes of primary interest are summarized in Table 4. Functional neck pain outcomes exhibited improvement from baseline to follow-up measurements. Reductions in mean scores (95% confidence interval [CI]) for PI and NDI were 1.7 (0.84–2.50) and 4.1 (2.62–5.51), respectively. POM, 1.1 (0.34–1.88), and BOP, 1.2 (−0.50 to 2.90), scores also demonstrated reductions in mean scores from baseline to follow-up.
Results for Clinical Outcomes of Interest at Baseline (Mean and Standard Deviation), 16-Week (Mean and Standard Deviation), Change from Baseline to 16 Weeks (Mean and 95% CI), and Cohen’s d (95% CI) (n = 15)
Denotes clinical outcomes where a decrease is considered an improvement, and as such were analyzed as baseline minus 16 weeks in order to maintain positive values for ease of interpretation.
PROMIS-29 scores were converted to T-scores.
APSRA, ability to participate in social roles and activities; BOP, bothersomeness of pain; CI, confidence interval; MBI, Maslach Burnout Inventory; NDI, Neck Disability Index; PI, pain intensity; POM, pain on movement; PROMIS-29, Patient-Reported Outcomes Measurement Information System 29; SD, standard deviation.
Quality of life, psychosocial health, and employee health-related change in outcomes were variable. Little change was observed in the PROMIS-29 subscales of depression and anxiety, as well as in the MBI subscales of depersonalization and personal accomplishment and the GSE-6. Modest improvements from baseline to follow-up were observed in the MBI subscale of emotional exhaustion and the PROMIS-29 subscales of sleep disturbance and physical function. Clinically important improvements 51 were seen in PROMIS-29 subscales of fatigue, ability to participate in social roles and activities, and pain interference (Table 4). Additional outcomes including measures of psychosocial, 52 –55 cognitive, 56,57 and physical function 58,59 are reported in Supplementary Table S2.
Qualitative results
At baseline, a total of 21 semi-structured interviews, ∼20–30 min in duration, were conducted. 60 At 16 weeks, 15 participants completed an additional semi-structured interview focused on perceptions of facilitators and barriers to participation, effects of the interventions, and their impact on neck pain and overall quality of life. Of note, audio files for 4 of the 16-week interviews were not usable. Six themes were identified and described below. Supporting quotes can be found in Table 5.
Qualitative Quotes Grouped by Theme
Neck pain is inherent to nursing
Participants described the types of nursing activities they believed contributed to their pain: lifting and moving patients; conducting clinical assessments while bending over at the bedside; and using computers to chart notes by the bedside, at nursing stations, and in their cars after home visits, without consideration of ergonomics. They viewed CNNP as an inevitable part of nursing.
Nurses push through the pain
Despite their pain, nurses persisted with their assigned duties. They tolerated their pain, continued with their duties, and explained that if they became unable to manage the pain, they would leave nursing.
MCC prevents and relieves pain
Participants described the chiropractic sessions as hands-on, focusing on relieving pain and preventing future pain. DCs explained factors contributing to their neck pain and explored options to address the pain. Participants understanding of neck pain changed from viewing pain as a function of their stressful work lives to a fuller understanding of contributing postural factors and the overall health of their spine. They learned exercises and postural support strategies to prevent or diminish neck pain. By focusing specifically on exploring and addressing causes, participants experienced significant relief and learned how to prevent the pain.
TC provides overall relaxation
Participants viewed TC as a holistic way to move and achieve a meditative state, thereby reducing their overall stress. TC, however, did not have the same specific effects on neck pain as noted with chiropractic sessions; rather, participants viewed TC as a method to increase overall mind and body relaxation.
Combined interventions increase body awareness and improved posture in daily life
Participants described learning about body awareness and how to prevent or lessen pain. TC taught them to take a few moments to refocus, prepare for stress, and slow down. Chiropractic care included lessons to improve posture through exercises and supports. These participants developed a sense of agency over their neck pain, developing strategies (e.g., ergonomic training at the desk, breathing practice from TC) that generalized to their daily lives.
Scheduling, traveling, and payment as obstacles
Participants expressed scheduling as an obstacle to continuing TC and chiropractic care. Participants described problems with fitting sessions into their busy schedules. The personalization of chiropractic care seemed more compelling to find time to schedule. Although virtual sessions were available for TC, they required scheduling into participants’ routines and were not considered as satisfying as in-person TC. One nurse wished for access to chiropractic or TC sessions scheduled into their weekly work routines, at their worksites, as a health maintenance benefit.
Discussion
Nursing is health care’s largest occupation in the United States, 61 and nurses provide crucial care and support. 62 Nurses face unique stressors that can significantly impact their well-being. This is the first trial to explore the feasibility and potential benefits of combined MCC and TC for nurses with CNNP. Findings generally support the feasibility of delivering these combined multimodal interventions to a nursing population with CNNP. Modest improvements in pain and disability were observed. Qualitative findings inform feasibility and provide insights into participant’s experiences with improved body awareness, pain severity, knowledge, self-management capacity, and stress. Additionally, qualitative data indicated that nurses perceive CNNP as a challenge inherent to the profession, something to be endured while caring for patients. These findings support the feasibility and importance of conducting a fully powered controlled trial evaluating the combined effects of chiropractic care and TC for nurses with CNNP.
While recruitment rates were lower than expected, the target sample size was reached. The low recruitment rate was significantly influenced by the COVID-19 pandemic, which impacted nurses’ availability (i.e., professional and personal commitments) and ease of scheduling chiropractic appointments. Findings demonstrated favorable levels of adherence, supporting the acceptability of intervention components. Results from the qualitative interviews provided an initial understanding of barriers. The challenges described included the integration of chiropractic sessions and TC classes into the already demanding schedules of nurses, with the added complexity of virtual TC classes being more convenient but less satisfying than in-person classes. Additionally, the preference for interventions within the hospital during work hours emphasizes the importance of offering interventions that align with participants’ professional commitments. 63,64 While recruitment and adherence goals were met or exceeded, the slightly lower than targeted retention rates call attention to continued investigation into factors influencing the engagement of younger, more educated nurses with less duration of CNNP in future trials.
Clinical outcomes related to pain and disability demonstrated modest improvements with mean reductions in PI [1.7 (0.84–2.50)] and NDI scores [4.1 (2.62–5.51)]. While these reductions approached the minimum clinically important difference in both pain (∼2) 65,66 and NDI (5–10), 66,67 it is important to note that mean baseline PROMIS-29 pain interference and physical function scores were near the population average of 50. This suggests there may have been a smaller window for achieving substantial improvements. The modest reductions in pain and disability align with a growing body of literature supporting the benefits of chiropractic care and TC interventions individually. 2,18,19,68 –73 However, when combining interventions, additive or synergistic effects on clinical outcomes were not observed. While difficult to evaluate without a control group, the present findings suggest a need to understand how/when to integrate chiropractic care and TC interventions for optimal benefit. Interestingly, two components of MCC—extremity joint manipulation and prescribed breathing/relaxation techniques—were not utilized by the chiropractors in this study. Additionally, TC instructors did not receive neck pain-specific training for this study, though they were highly experienced in teaching classes with participants having various health conditions. Instructors typically provide guidance and adaptations to accommodate diverse student needs. Future trials investigating TC for the management of neck pain could benefit from providing instructors with additional training focused on neck pain-specific considerations and potential modifications.
Despite modest improvements in pain and disability, reductions in pain interference, emotional exhaustion (a key component of burnout), fatigue, and limitations in social participation were observed. These findings align with the established benefits of mind–body interventions and multimodal approaches in managing chronic pain and enhancing emotional resilience, particularly in health care providers. 74 –77 Results not only reaffirm the clinical improvements observed with multimodal approaches but also underscore the need to contextualize the management of CNNP within the biopsychosocial framework.
Key themes from qualitative findings suggest a complementary effect of combined interventions, emphasizing the significance of holistic mind–body approaches. Participants noted the importance of learning how to better manage and minimize their CNNP through exercise, postural awareness, and workplace ergonomics. Results demonstrate the transformative impact of mind–body interventions on nurses’ perspectives of CNNP, transitioning from an inevitable professional burden to a condition that can be actively managed. Both interventions were found to be enjoyable, showcasing the advantages of their combined utilization for CNNP.
Strengths and Limitations
This trial has several strengths. It represents the first trial to explore the combination of chiropractic care and TC for the management of CNNP in nurses. The qualitative component provided valuable insight into participant experiences. Limitations include the absence of a control group and a lack of blinding. To enhance generalizability, future research should involve diverse health care settings and a greater diversity of TC training programs. Additionally, strategies for improving recruitment and retention, such as flexible scheduling options, are needed.
Conclusions
This trial supports the feasibility of delivering combined MCC and TC for nurses with CNNP. The next step is to conduct a randomized, controlled trial with adequate statistical power.
Footnotes
Authors’ Contributions
P.M.W. was responsible for conceptualization. P.M.W., D.L., and W.B. were responsible for methodology and investigation. W.B., C.R.L., and P.R. were responsible for data curation and formal analysis of quantitative data with supervision from P.M.W. Formal analysis of qualitative data was completed by K.K. P.M.W., W.B., and K.K. were responsible for writing the original draft of this article. All authors contributed to reviewing and editing the final draft of this work. All authors read and approved the final article.
Author Disclosure Statement
P.M.W. has a financial interest in the Tree of Life Tai Chi Center, a Tai Chi teaching center. His interests were reviewed and are managed by Brigham and Women’s Hospital and Mass General Brigham in accordance with their conflict of interest policies. No other authors report any competing interests.
Funding Information
W.B. received funding for a postdoctoral fellowship from the
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.