
Abstract
Background:
As a prominent part of complementary and alternative medicine, Chinese Medicine (CM) has proved its strengths in treating a diverse range of acute and chronic medical conditions and is at present recognized in 196 countries and territories worldwide. In 2012, Australia regulated the CM profession under the National Regulation and Accreditation Scheme (NRAS) by legislation and reports quarterly demographic information about individual CM practitioners so to ensure public interest, although research examining the change of CM workforce in Australia has been scarce.
Objective:
This study aims to investigate the construction of the CM workforce in Australia and more importantly, evaluated its development in the last decade to capture the trajectory and trend in the present period and future potential changes.
Methods:
Data were sourced from the Australian Health Practitioner Regulation Agency (AHPRA) annual reports and the Chinese Medicine Board of Australia (CMBA) registration statistics from 2012 to 2023. A descriptive analysis was conducted with demographic variables, including profession, age, and gender, and chi-square tests and linear regression modeling were carried out to assess the variations between regions and across years.
Results:
The population of CM practitioners in 2022/2023 stagnated with slight decrease to 4,823, in contrast to the increase rate of 2.9% in the whole health care community. The number of young CM registrants (<35 y) shrank by 37.5% from 691 in 2012 to 432 in 2023. In comparison with other health care professions, CM comprises the smallest proportion of the population aged younger than 25 (0.2%) and the largest proportion aged older than 65 years (16.2%), advancing into an aging era.
Conclusions:
This study indicates a worrying potential decline in CM workforce in Australia, which is likely to be further exacerbated by the lack of new graduates and rise of median age among practitioners. Meanwhile, continued advancement in Western medicine technology and standards requires substantial efforts to increase both a better understanding of CM and demonstration of its efficacy. Furthermore, greater effort is needed to recruit and educate new young CM practitioners in Australia and to broaden the international training pipeline for a sustainable development of CM practice.
Introduction
Characterized by the Yin-Yang theory and holistic methodologies, Chinese Medicine (CM) is referred to as a medical science developed in ancient China from people’s life experience and clinical practice to treat diseases and maintain health. 1 In previous decades, CM has made a remarkable and swift migration, no longer confined within the Chinese national boundaries. More than 40 countries, regions, and international organizations have signed specialized cooperation agreements on CM with hundreds of overseas CM centers and bases in operation. 2 There are more than 300,000 clinics practicing CM across the world, approximately 4 billion people have benefited from Chinese herbal medicine products, and the annual trade volume of the industry is nearly 500 billion yuan. 3–4 The practice of Traditional Chinese Medicine, with a diverse range of therapies including acupuncture, moxibustion, cupping, scraping, massage, and herbal medicine, has gained a foothold in 196 nations and territories to date across the world, Australia being the first Western country to provide CM legal recognition and protection. 2
Development and recognition of CM in Australia
It was not until the mid-1800s when the first wave of Chinese immigrants embarked on a voyage across the Pacific Ocean before landing on the continent of Australia that ushered in a new chapter for CM in Australia. Along with the increase in numbers of Chinese people settling in Australia, the need for and reputation of CM rose. Driven by financial incentives or genuine passion, individuals of both Chinese and non-Chinese origins have chosen to pursue careers as CM (TCM) practitioners. This includes those with medical backgrounds as well as individuals who have transitioned from other professions, especially during the early days when qualification standards were relatively lenient. In 2007, it was reported that 19.3% of the national population in Australia had received at least one form of CM treatment. 5 Another national survey conducted five years later revealed a prevalence rate of 9.5% in young and 6.2% in middle-aged women who had consulted an acupuncturist in the past year. 6 According to a survey conducted in the state of Victoria, Australia, CM practitioners are characterized by high-level education, diverse background, and often a rich clinical experience. 7
Formal CM training courses entered the Australian tertiary education system in the 1990s to provide CM students with both theoretical and practical competence. As of August 2023, six higher education institutions in Australia were accredited by the Chinese Medicine Board to offer CM programs. These institutions collectively offered eight CM programs, with three of them in a teach-out mode that provide necessary support for the present students to finish their studies before being formally discontinued. 8 The Australian Federal Government initiated the registration of CM practitioners on July 1, 2012, marking a nationwide official recognition for CM practice and providing legitimate protection and regulation for individual CM registrants and their clients.
Chinese Medicine Board of Australia
The Council of Australian Governments (COAG) decided in 2008 to establish a single National Registration and Accreditation Scheme (NRAS, simplified as National Scheme hereafter) for health practitioners to get registered. The National Scheme aims not only to manage health services, but to regulate individual health practitioners nationwide and is a vital part of the national health system. The Australian Health Practitioner Regulation Agency (AHPRA), responsible for implementing this National Scheme, works together with 15 partner national health practitioner boards (hereafter referred to as National Boards), including the Chinese Medicine Board of Australia (hereafter referred to as the Board), to ensure public safety and practice qualification across the country.
At present, more than 877,000 health practitioners from 16 professions are registered with AHPRA and the population of all health professions increases around 3% each year since the National Scheme began. 9 Meanwhile, practitioners under registration are monitored by Aphra to ensure compliance with restrictions placed on their registration for concerns about health, performance, and conduct. Guided by such principles, titles of “acupuncturist,” “Chinese herbal dispenser,” and “Chinese herbal medicine practitioner” are legally protected titles. Anyone who calls themselves a CM practitioner must be registered with the Board and it is an offense to conduct medical practice without registration. As an authoritative national agency in Australian health system, AHPRA, together with the National Boards, claims to provide accurate and complete data, and strives to be transparent, fair, and accountable. The analytical reports available on the AHPRA websites are open to the public and have proven to be a valuable resource for conducting in-depth investigations into the demographic information and long-term goals of CM practitioners. Studying the history and status quo of CM registrants can provide insights into the strengths and drawbacks of CM practice and shed light on its future development.
Registration standards
For initial registration, the Board requires all applicants to demonstrate adequate English proficiency, provide a history of criminal convictions (if existent), and to have obtained professional indemnity insurance for a successful registration. In general, the conditions for registration have been quite consistent for the past decade, except for the most frequently complained issue of the English language requirement raised from IELTS 6 to 7 points per course, making it more challenging for non-native English speakers to register despite having a rich clinical experience. 10
Based on registrations by division, CM registrants can be differentiated with their titles of acupuncturists, Chinese herbal medicine practitioners and Chinese herbal dispensers. Meanwhile, a list of educational courses and units of study are provided by institutions accredited and approved by the Board to ensure the applicants’ competence.
Since 2012, the Board has been publishing quarterly data profiling Australia’s CM workforce, including a number of statistical breakdowns about registrants. In 2022, the Board celebrated the 10th anniversary of national regulation of CM in Australia. It is therefore timely to look retrospectively the past decade since the development of CM registration and the composition of practitioners in its present and prospective situations.
Objectives of this study
By conducting a comprehensive investigation of the CM workforce in Australia, with reference to other medical professions and longitudinally spanning over 11 years, this study aimed to examine the demographic changes in the CM practitioner community nationwide, and accordingly, proposes possible solutions for reforming the present situation.
The demographic information of CM practitioners, with reference to other professions, contributes to a better understanding of the present status of CM practice in Australia. The longitudinal study of population change in the past decade could assist in providing a reliable and effective index to predict CM development in the foreseeable future.
Materials and Methods
The data of Australian CM registrants were retrieved and downloaded from “Statistics” on the Australian national health website Chinese Medicine Board of Australia (https://www.chinesemedicineboard.gov.au/About/Statistics.aspx), where registration data and statistical breakdowns are produced quarterly to be shared with the public community since the establishment of the Board in 2012. Information covers: registration type by principal place of practice, registrations by principal place of practice percentages, registrations by division (specialty), age, gender, etc. Due to the fact that the registrants’ data do not vary hugely from season to season within a year and that a simplified manner of analysis is sufficient to trace progression, only data of the last reporting period (October 1 to December 31) from year 2012 to 2022 are compared in parallel for descriptive analysis in this study. Nevertheless, due to the time constraints when the study was conducted, the data in 2023 were only available till June, which were therefore obtained and analyzed together as indicators for yearly change.
From a broader perspective, the data regarding all health care professions were obtained and analyzed from AHPRA’s annual reports [Australian Health Practitioner Regulation Agency-Annual reports (ahpra.gov.au)] unless specified otherwise. Information about the national population can be found from the Australian Bureau of Statistics (ABS, https://www.abs.gov.au/statistics/people/population).
The majority of the data were analyzed descriptively. A chi-square test was utilized to assess variations in the distribution of CM practitioners across regions. For the changes of population in different age groups over time, a linear regression model was conducted, with reported F values and coefficients. All statistical analyses were carried out using SPSS 28.0 and effect sizes were also reported.
Results
CM has a small group size compared with other health professions
With an annual growth of 2.4%, the national population in Australia reached 26.64 million at the end of June, 2023 (ABS), 11 among which 4,823 persons are registered as CM practitioners on the Board, making up 0.018% of the national community. That is to say, on average there are less than two individuals out of every 10,000 people in Australia practicing CM as a profession.
Despite most other professions, the population of CM practitioners in 2022/2023 encountered a decrease by 0.30% to 4,823, in contrast to the increase rate of 2.9% in the general health care community. 12 A chi-square test revealed a notable discrepancy in the distribution of CM practitioners compared with the population in each state (χ2 = 29.35, p < 0.001). The highest concentration of CM practitioners was found in New South Wales, with approximately 2.3 practitioners per 10,000 people, followed by Queensland (1.6 per 10,000) and Western Australia (0.9 per 10,000), while Tasmania had the lowest concentration at 0.8 practitioners per 10,000 individuals. Moreover, a correlation analysis conducted in SPSS uncovered a strong positive correlation (r = 0.911, p = 0.002) between the total state population and the ratio of CM practitioners in that state.
It can be seen from Table 1 that CM takes up 0.5% of the total health care population, representing an evidently small group size comparable with chiropractors and osteopaths, although the latter two achieved an increase of 3.2% and 4.0%, respectively. The registered health practitioner workforce has been predominantly female. All professions show slight to large gender differences and due to the significant number of nurses and midwives, the male-to-female ratio in the total health care population is about 1 to 3, and the trend of feminizing is still in progress. While female registrants outnumber males in many domains, the reverse is observed in chiropractic, medicine, and paramedicine, possibly due to the physically demanding nature of these professions. As for CM practitioners, the population is composed of 58.4% of females and 41.6% of males in year 2022/2023, similar to the gender composition in optometrists (58.6% vs. 41.4%) and podiatrists (59.0% vs. 41.0%).
Registration of Health Practitioners in Australia 2022/2023
The sum of registrants is smaller than the addition of all professions due to dual registration in nurses and midwives.
Age and gender
Based on the Annual Report 2022/2023 released by AHPRA and the National Boards where information of all health care registrants across 16 professions is presented, about 5% of the population are younger than 25 years, and about 7% of the registrants are older than 65 years, a stage strongly associated with retirement (noting that the official retirement age in Australia is presently set at 67 following pension system reforms). Overall, the age distribution of the population in the health care system suggests a predominantly young community, aligning closely with the national average age (mean = 39.8) according to the ABS. By contrast, among the 4,823 CM practitioners in 2023, only 0.2% of the registrants are younger than 25 years, 8.4% younger than 35 years, while 16.2% are older than 65 years, reflecting a receding group of younger individuals entering the CM field for a professional career. The majority (75.1%) of CM practitioners fall between the ages of 35 years and 64 years and the number of 55–64-year-old individuals outweighs that of 35–45-year ones. Compared with the other 15 health care professions, CM comprises the smallest proportion of the population aged younger than 25 (0.2%) and the largest proportion aged older than 65 years (16.2%), indicating an aging trend in CM practitioners. If no effective actions are taken, the CM profession will in the foreseeable future be faced with a workforce challenge where more CM practitioners will retire than those who newly join (Fig. 1).
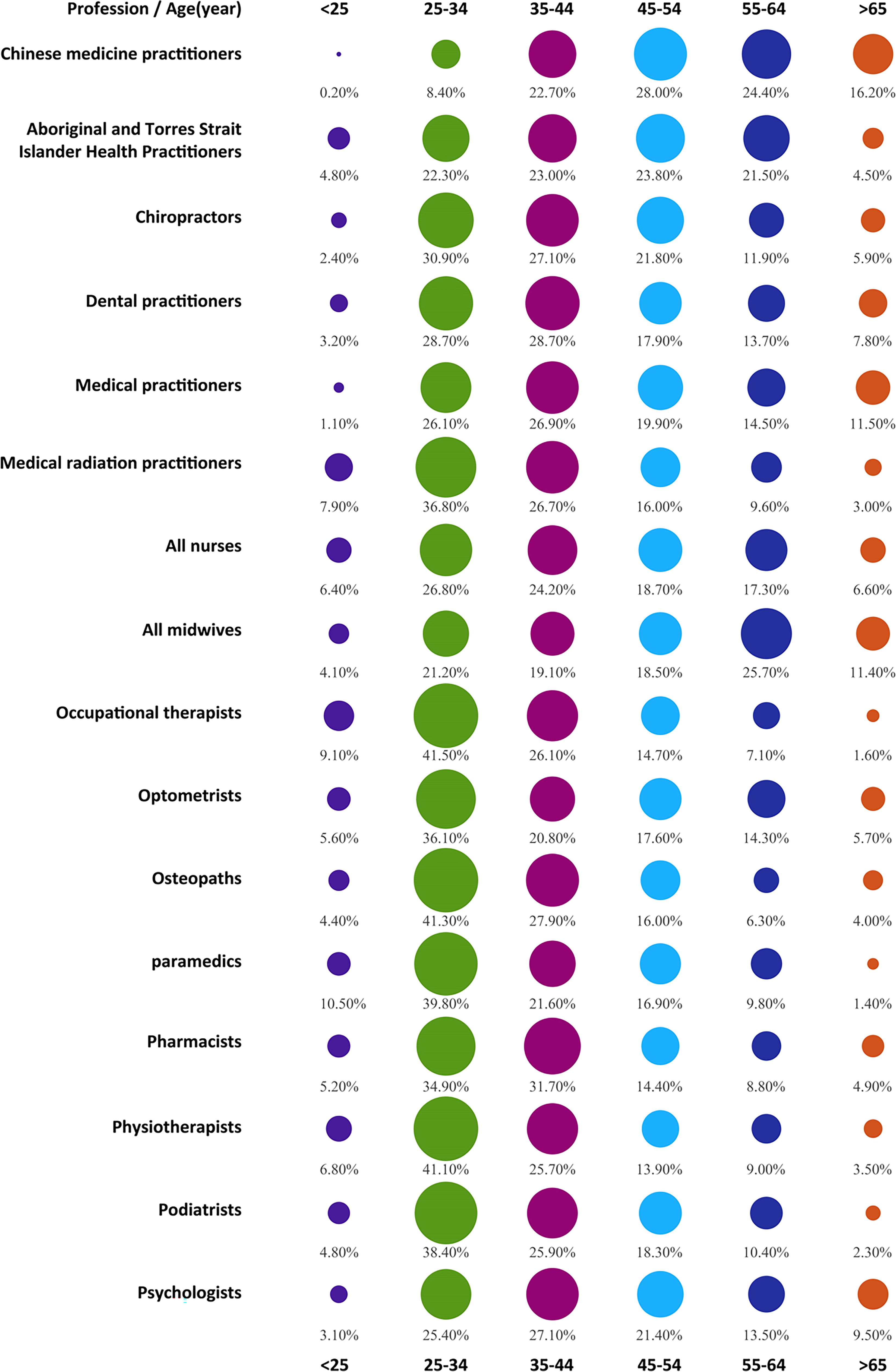
Age distribution across all health care professions 2022/2023. The colored circles indicate the different age ranges from under 25 to greater than 65 and their size indicates the population proportion.
CM workforce change from 2012 to 2023
Australia had a national population of 22.9 million in 2012 and this increased by 16.2% in 11 years, reaching over 26.6 million at the end of June, 2023 (ABS)[9]. During the same period, the health care registration number grew by 48.0% from 592,470 to 877,119 and the number of CM practitioners rose from 3,952 to 4,823 with a growth ratio of 22.0%, which is less than half of the increase among the general health care population.
Taken from another point of view, the annual rate of increase in the Australian national population stays around 1.5% and that of health care system is near 3.0%, while the number of CM practitioners after an increase in the first 5 years has stayed stable with little fluctuations in the past 7 years and has slightly decreased since 2021 (Table 2). The years 2014 and 2015 saw the biggest workforce boom (7.4% and 7.2%, respectively), but from 2017, the rate of increase slowed down to less than 1 percent, while in 2021 the population turned to a declining trend in various degrees. Noticeably alongside the population change in total CM practitioners, acupuncturists, Chinese herbal medicine practitioners and dispensers, all followed the trajectory of increase and decrease, although Chinese herbal dispensers reached their peak number later than the other two but still faced a flat change in recent years (Fig. 2).
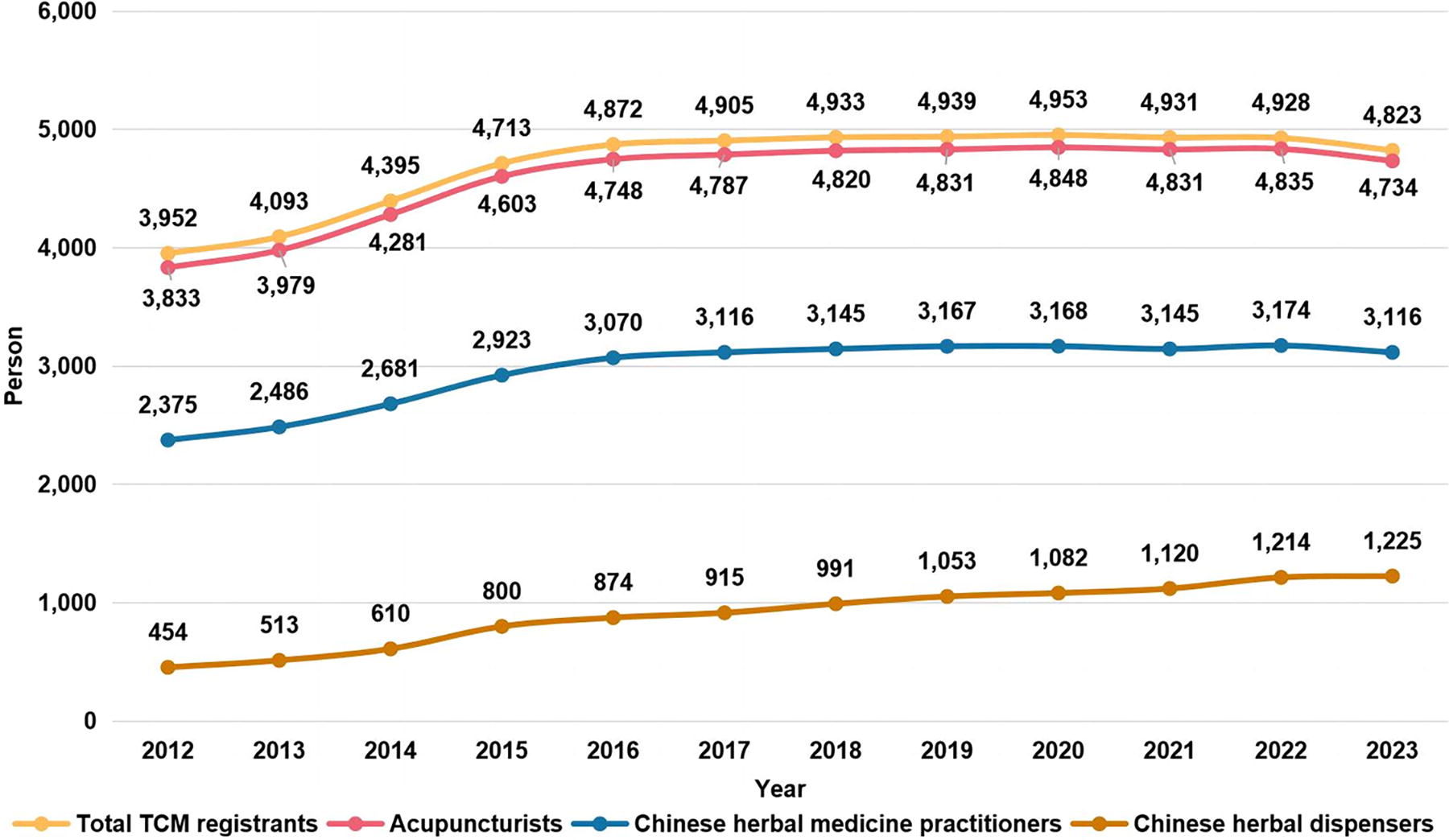
Line graphs indicating the numbers of Chinese Medicine registrants in different categories from 2012 to 2023.
Chinese Medicine Registrants by Division from 2012 to 2023
The greatest proportion (>96%) of the CM professionals chose to be registered under the division of acupuncturists, while about two-thirds of registrants aimed for Chinese herbal medicine practitioners and increasingly more people register themselves as Chinese herbal dispensers, although it should be noted that applicants can select more than one division for registration.
Gender
As illustrated in Figure 3, in 2012, the CM registrants were composed of 53.1% (2,097) female practitioners and 46.9% (1,854) males. In the following ten years, the gender ratio further diverged with continuous enlargement of the female proportion, and by 2023, female staff make up to 58.4% (2,816) of the whole profession (Fig. 3), which is consistent with most other professions in the health care system with more women than men engaged in medical practice.
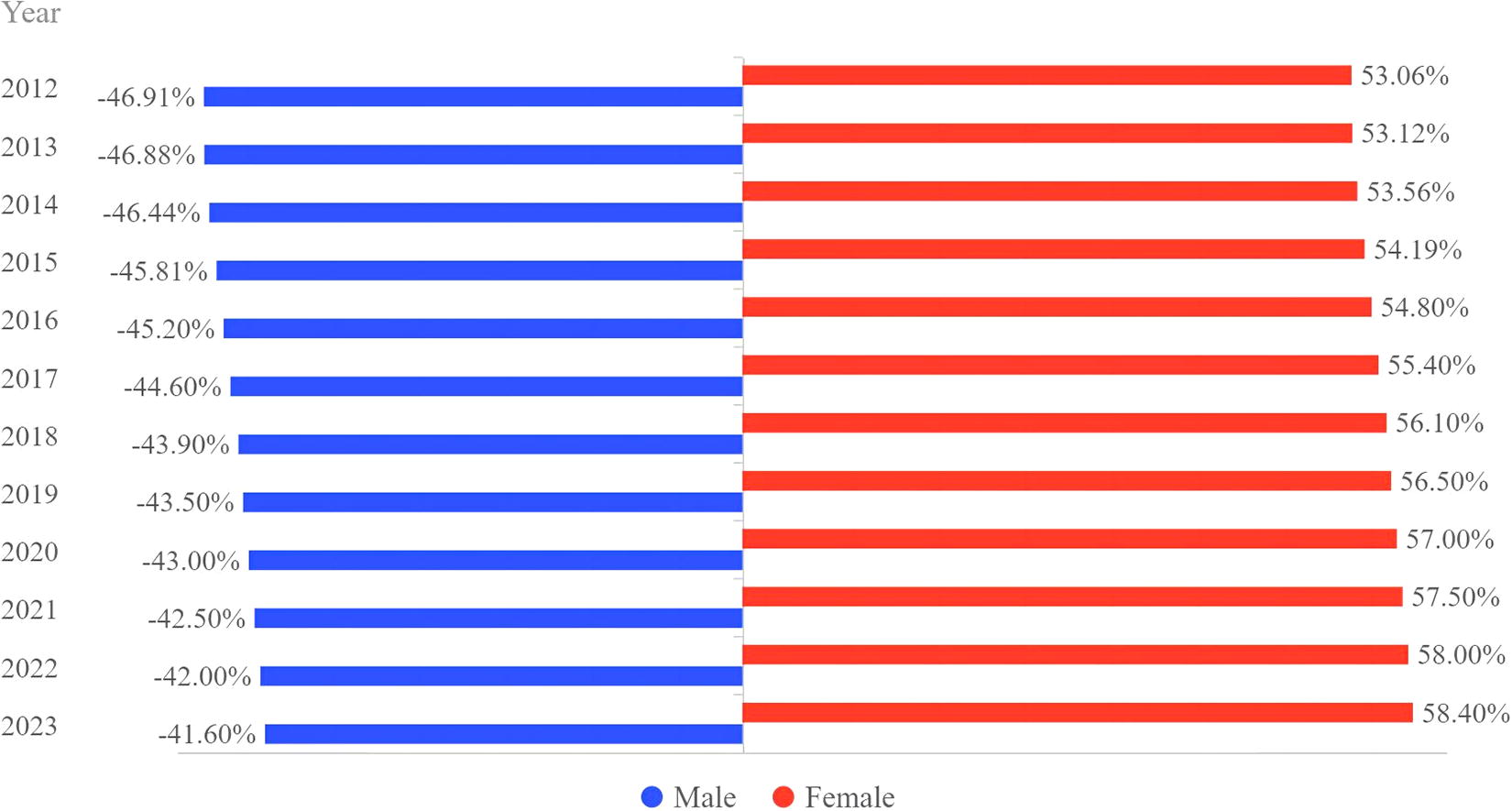
Bar graphs indicating the proportions of male and female Chinese Medicine practitioners from 2012 to 2023.
Age
CM practitioners in Australia are distributed over a wide range of ages from younger than 25 years to older than 80 years, with a trend of increasing weight toward an aged population (Fig. 4). In 2012, 691 out of 3,952 CM registrants (17.5%) were younger than 35 years, while 2,163 (54.7%) were between the ages of 25 and 54 years, and 1,098 (27.8%) were older than 55 years. In the following ten years, however, the number of young registrants (<35 y) has been constantly shrinking, and by 2023, the number decreased by 40.1% to 414. A linear regression analysis revealed a strong negative relationship between year and the number of young CM registrants [F(1, 10) = 26.274, p < 0.001, r2 = 0.724]. Registrants aged between 35 and 54 years increased from 2012 to 2016 but faced a turning point after 2017 when the numbers showed signs of stagnation. On the contrary, registrants older than 55 witnessed a stable escalation from 1,098 in 2012 to nearly 2,000 in the past four years, 4.7 times of registrants younger than 35 years. The linear regression analysis showed a remarkable increase of senior CM practitioners across years [F(1,10) = 136.623, p < 0.001, r2 = 0.932]. The striking contrast of the population changes among the young and the aged reflects a rather aging community in the Australian CM profession. Details are shown in Figure 4.

Bar graphs indicating the numbers of Chinese Medicine registrants across different age groups from 2012 to 2023.
CM student enrollment
Students provide primary sources of workforce in the health care system. A register of presently enrolled students is maintained by AHPRA as part of the national register launched in 2011, with details collected from over 130 accredited education providers. Students who undertake certain CM programs approved by the Board will be granted a qualification eligible for professional registration.
Figure 5 demonstrates distinct variations in numbers of students registered with CM programs, ranging from 1,169 in 2013 as the first calculation after the Board was established to the last three years, by which the count maintained around 1,500 (Fig. 5). In 2022, there were 1,574 students registered with the AHPRA, contributing 0.85% to the total size of 188,431 health care students under registration, a larger proportion of present CM practitioners (0.57%) among all health care registrants. However, due to close-ups of CM major in certain universities, the number of registered students in 2023 dropped to 923 in 2023, a considerable change from the previous ten years.

Bar graphs indicating the number of registered Chinese Medicine students and practitioners from 2013 to 2023.
Discussion
CM workforce structure change
Results presented in this study indicate an aging community of CM practitioners in Australia and a trend of deterioration. While the general health care community across 16 professions, including CM, witnesses a total annual surge of approximately 3%, alongside the national population increase of about 1.5%, the sum of CM practitioners has stayed stable with little fluctuations in the past 7 years and has decreased since 2021 to the present number of 4,823. On the contrary, according to the ABS release, the mean age of the national population in late 2022 reached 39.8 years, and the median being 38.5 years, representing a relatively youthful society. In the CM practitioner workforce, however, the median age of CM practitioners reached 51 years in 2021. 12 Moreover, a 2018 study showed that the majority of practitioners in complementary and alternative medicine obtained their qualification more than ten years ago, suggesting a lack of new comers in this field. 13 Indeed, the number of younger CM registrants (<35 y) has been constantly decreasing in the past ten years from 691 in 2012 to 414 in 2023 representing a significant drop of 40.1%. By comparison with other health care professions, CM comprises the smallest population aged younger than 25 years (0.2%) and the largest proportion aged older than 65 years (16.3%). In addition, the number of registrants exceeding 55 years has been constantly increasing from 1,098 in 2012 to nearly 2,000 in the past four years, which is 4.7 times the number of registrants aged younger than 35 years. With more and more registrants aged 35–54 years moving into an older age range over time, the number of CM professionals aged 55+ is estimated to rise even further. Taken together, set in a background where the health care system workforce maintains an annual increase, a stagnated or even shrinking number of registrants in CM could be further marginalized from its already fragile status. A reduced injection of young registrants in contrast to a large body of aging practitioners also strikes an alarm bell for the future of CM practice in Australia.
The distribution of CM practitioners, primarily concentrated in New South Wales, Victoria, and Queensland, correlates with the population density in these states and their contribution to the Australian economy, 14 suggesting an economic incentive driving the CM profession to establish practices in these more wealthy regions. Similar to most occupations in the health care system, more women and men are engaged in CM practice (58.4% vs. 41.6%). With regard to the female/male ratio of the whole national population being 50.37% versus 49.63%, it is therefore concluded that a larger proportion of women choose to participate in CM practice. This is in line with the fact that women are more likely to resort to Chinese herbs or acupuncture for therapeutic purposes 15 and a female practitioner may be of preference for patients to consult. The majority of CM practitioners are registered under the division of “acupuncturists,” possibly due to the situation that the use of acupuncture in Australia is more common than the use of Chinese herbal medicine. 4 This is also the case historically, where acupuncture was more easily introduced, taught, and practiced in Australia.
Student registration for CM
The number of student registrants had stayed around 1,500 in the past several years and maintained a proportion of ∼0.80% of all the health care students, until in 2023 the number slumped to 923 due to the fact that fewer students were admitted in the higher educational system. Still, since the data from AHPRA showed that very few CM practitioners younger than 25 are actually registered, this raises the question whether students who take CM as their mainstream interest pursue a long-term career in CM after graduation. It is reported that most CM practitioners in Australia work as individual professionals without being officially employed by a hospital, 16 and hence a lack of organizational incentive or professional security may discourage graduates from pursuing a career in CM practice.
Students are the key source of a future CM workforce, but universities have been confronted with operational difficulties due to low student enrollment. 17 Indeed one of the largest providers of CM education in Australia, the University of Technology Sydney, has recently ceased its accredited CM program. 18 Furthermore, at the time of writing, the RMIT university has also stated it will not have an intake of CM students in 2024, heralding the closure of another well-established educational program. 19 The loss of these accredited university programs will mean not only fewer students but also a drop in research capability and publications from Australian postgraduate researchers. While there is no sign of waning in consumer demand for CM services as yet, fewer students could directly result in a reduced number of professionals practicing CM in the future. Unlike in China, CM in Australia does not have a strong cultural basis and the odds of it being considered a cultural dogma or superstition do exist and may act to impede its development. In an era where evidence-based medicine is the predominant medical discourse, scientific validation for any form of medicine has become an ethical imperative and medical practice is required to be unbiased, reliable, and widely available to the majority of citizens. In this respect, however, CM often finds itself in need of measurable methods and standardized techniques to demonstrate therapeutic safety and efficacy. 16,20
CM is a unique profession with complex theoretical and practical approaches. However, due to distinct disparities in cultural perceptions, social norms, and life styles between China and the Western countries, CM is unfortunately often portrayed and practiced in an oversimplified manner and has therefore inevitably lost its original foundations, including theoretical and philosophical principles. Several surveys in Australia revealed that the majority of practitioners follow CM philosophies and theoretical frameworks to diagnose and treat patients. 6,21 Nevertheless, with the affiliated concepts of holism, five-elements, and Yin-Yang theory undermined in the Western countries, recipients mostly focus on the actual curative effects and are less likely to enquire into the mechanisms, which systematically explain and guide the diagnosis and treatment from a Traditional CM perspective. According to another survey conducted among CM practitioners in the State of Victoria, Australia, the majority of participants were attracted to the philosophy of CM or effects of treatment before they chose CM as a career. Regrettably, only a limited proportion were convinced by the income they could achieve, indicating that personal financial benefits may have been perceived as unsatisfactory. 7 With a totally diverse ideological system and worldview, most Westerners have substantial obstacles to overcome to understand, appreciate, and master CM knowledge, which might be another reason why fewer and fewer young people are pursuing CM as their career. 17 It is therefore suggested that basic concepts and theories of CM should be given more attention and emphasis in education and preferably explained in an accessible manner when CM is being used to treat specific problems.
In summary, it has been over 11 years since the Australian Federal Government implemented the registration of national CM practitioners on July 1, 2012. After an initial surge of prosperity, CM practitioners have come to a critical stage of an aging and shrinking workforce as fewer younger people enter the profession. Despite its popularity, CM is still referred to as complementary and alternative medicine in the Western countries, Australia being no exception. Reasons impeding the development of CM may vary from cultural diversity, weakness in quality control, as well as inadequate research validation and challenges to technological innovations. 22,23 To address this problem, essential efforts await to be taken to recognize, calibrate, revise, and modernize CM for a better integration into the Western medical system and consequently attract more people to enter the CM field for a career.
Conclusions
CM in Australia represents a minor health profession with a declining population and aging demographic, raising concerns for the long-term sustainability in the community. Results presented above are important for assisting with CM planning and reform in Australia and elsewhere in other countries, especially for CM practice to maintain a healthy and continuous evolution. In response to the changes of workforce constitution and biased age distribution, awareness and improvements should be made to advance the profession’s popularity to attract more interest and engagement.
Authors Disclosure Statement
The authors declare no conflict of interest.
Footnotes
Authors’ Contributions
Conceptualization: Q.L. and J.C.; methodology: Q.L.; formal analysis: Q.L., D. X., and J.L.; writing—original draft: Q.L.; writing—review and editing: K.M.K. and C.Z; supervision: C. Z. and J.C.; validation: C.Z.; funding acquisition: J.C. All the authors have read and agreed to the published version of the article.
Funding Information
This research was funded by the National Social Science Fund of China, Research on the cross-cultural communication of intangible cultural heritage of Traditional Chinese Medicine in Australia (grant number 19XXW005), and Chengdu University of Traditional Chinese Medicine Xinglin Project (grant number QNTD20222004).