
Abstract
Introduction:
Primary dysmenorrhea (PD) is associated with decreased performance and reduced quality of life in young adults. This study aims to evaluate the effectiveness of implementing Arogya Rakshak Panchatantra (ARP), a naturopathic lifestyle practice, among young female adults with PD.
Method:
This open-label, parallel-arm, randomized controlled trial included 52 young female adults with PD aged between 16 and 25 years. They were randomly assigned to the ARP group practicing the ARP module for 2 months or the control group maintaining their routine lifestyle. The primary outcome was changes in heart rate variability (HRV), while secondary outcomes included menstrual distress, quality of life, pain, and daytime sleepiness, all evaluated at baseline and during the first three menstrual cycles in both groups. To evaluate the feasibility, the study also monitored self-reported symptoms, emotions, adverse events, calorie intake, and adherence to the intervention. The effectiveness of ARP was evaluated using repeated measures analysis of variance and a generalized linear model.
Results:
In the intervention group, we observed significant improvements in the high frequency component of HRV (p = 0.007), as well as reductions in weight (p = 0.017), visual analog scale pain (p = 0.000), and retrospective symptom scale score (p < 0.011). There were no significant changes in other HRV metrics, quality of life, or daytime sleepiness. Participants reported mild symptoms such as headaches, colds, body pain, diarrhea, constipation, fever, and weakness, with no serious adverse events.
Discussion:
This trial is the first to examine the long-term impact of ARP on young females with PD, suggesting it could be an effective and feasible management option. Further research with larger sample sizes is needed to confirm these findings.
Introduction
Primary dysmenorrhea (PD) is one of the most prevalent yet disregarded and undertreated conditions among the females. 1 PD affects nearly 50%–70% of women of reproductive age. 2 PD is characterized by spasmodic and painful cramps in the lower abdomen that begin immediately before or at the onset of menstruation, in the absence of any pelvic pathology. PD is associated with elevated prostaglandins (PGF2a, PGE2) and inflammatory mediators, such as vasopressin, C-reactive protein (CRP), vascular endothelial growth factor, tumor necrosis factor-alpha, and interleukin-6, which contribute to increased uterine tone and contractions. 3 –7
Paracetamol, aspirin, and nonsteroidal anti-inflammatory drugs are commonly employed to manage PD; however, they are often linked to gastrointestinal side effects such as nausea, vomiting, and diarrhea, as well as an increased risk of stroke. 8,9 Alternative approaches for managing PD are gaining popularity. These include transcutaneous electrical nerve stimulation, transdermal nitroglycerin patches, heating pads, rest, sleep, exercise, chiropractic care, acupuncture, meditation, aromatic oils, ginger root tea, warm saltwater baths, increased intake of calcium and magnesium, boosting vitamin D levels, consuming nutrient-rich foods, prayer, and quitting smoking. 3,10 –15 Despite the availability of various therapies, PD remains a predominant reproductive issue among women. The duration, dosage, and long-term impact of integrating these therapies have not been well explored, highlighting a research gap in understanding the effects of combined behavioral changes.
Arogya Rakshak Panchatantra (ARP) includes combination of holistic lifestyle regimens like prayer, exercise, fasting, water drinking, and moderate eating. 16 ARP is a traditional strategy used in yoga and naturopathy system of medicine for most of the ailments including PD. Individual components of ARP have been shown to improve clinical outcomes for PD. 11,17,18,19,20 However, the long-term effects of integrating these interventions, especially in relation to PD, have not been studied. This study aims to investigate the impact of two months of ARP practice on heart rate variability (HRV), menstrual distress, daytime sleepiness, and quality of life in young female adults with PD. The study also aims to assess the feasibility of introducing such lifestyle interventions.
Method
Study setting
This open-label, parallel-arm, randomized control trial was conducted at Sant Hirdaram Medical College of Naturopathy and Yogic Sciences for Women, Bhopal. The study was approved by the Institutional Ethics Committee (F.No:12/SHMCNYS-IEC/P22/2022–2023) and registered in the Clinical Trial Registry of India (CTRI/2022/11/047041).
Study population
Undergraduate medical students residing at the residential facility attached to the study setting were invited to participate through direct person-to-person contact. Participants were briefed on trial-related procedures, the overall duration, guidelines to follow, and the data collection process. Informed consent was obtained from all eligible participants.
Inclusion criteria
The study included females aged 18–25 years with a regular menstrual cycle lasting between 28 ± 7 days for the past three months, a body mass index within the range of 18–25 kg/m2, a diagnosed case of PD based on PD consensus guidelines, 21 and a menstrual pain severity rated as 3 or more on a visual analog scale (VAS) during the screening.
Exclusion criteria
The study excluded participants with a history of systemic pathology, gynecological or psychiatric diseases, as well as those with secondary dysmenorrhea. Individuals using oral contraceptive pills or undergoing hormonal therapies within the past three months were also excluded. The screening was conducted on the second day of menstruation during the previous menstrual cycle, prior to the baseline assessments for all participants.
Sample size
The sample size was calculated using G*Power Statistical software version 3.1. Based on an assumed power (β) of 80%, a level of significance (α) of 0.05, and an effect size (d) of 0.8, the required sample size was determined to be n = 52. Due to the limited data available on the effect of ARP on PD, the effect size of 0.8 was derived from a previous study that examined the impact of physical activity (one component of ARP) on HRV. 22
Randomization
The study utilized a simple randomization technique, employing a computer-based random number generator (randomizer.org) to generate a random number sequence. Based on this sequence, eligible participants were allocated to either an experimental (ARP) or a control group. Allocation was concealed using sequentially numbered, opaque, sealed envelopes (SNOSE), which were opened just before the trial to prevent potential bias. The randomization and preparation of SNOSE were conducted by a researcher who was not part of the trial.
Blinding
The nature of the present study did not allow blinding of the investigators and the participants. However, the assessors, the data manager, and the statistician were blinded to the allocation.
Intervention
The experimental group practiced ARP for two consecutive months starting from the baseline (5th day of the last menstrual period before intervention) and had, whereas the control group maintained their regular lifestyle, which included an unstructured diet with three meals a day, no fasting regimen, and no structured participation in prayer or exercise.
Outcomes assessment
The baseline assessments for HRV, retrospective symptom scale (RSS), SF-12 Health-related quality of life questionnaire, Epworth daytime sleepiness scale (ESS), and VAS pain were conducted on the second day of the menstrual cycle prior to the intervention. Subsequent assessments were performed on the second day of each subsequent menstrual cycle over three months (three cycles), totalling four assessments during this period. Similar assessments were carried out for the control group at corresponding time points (Fig. 1).
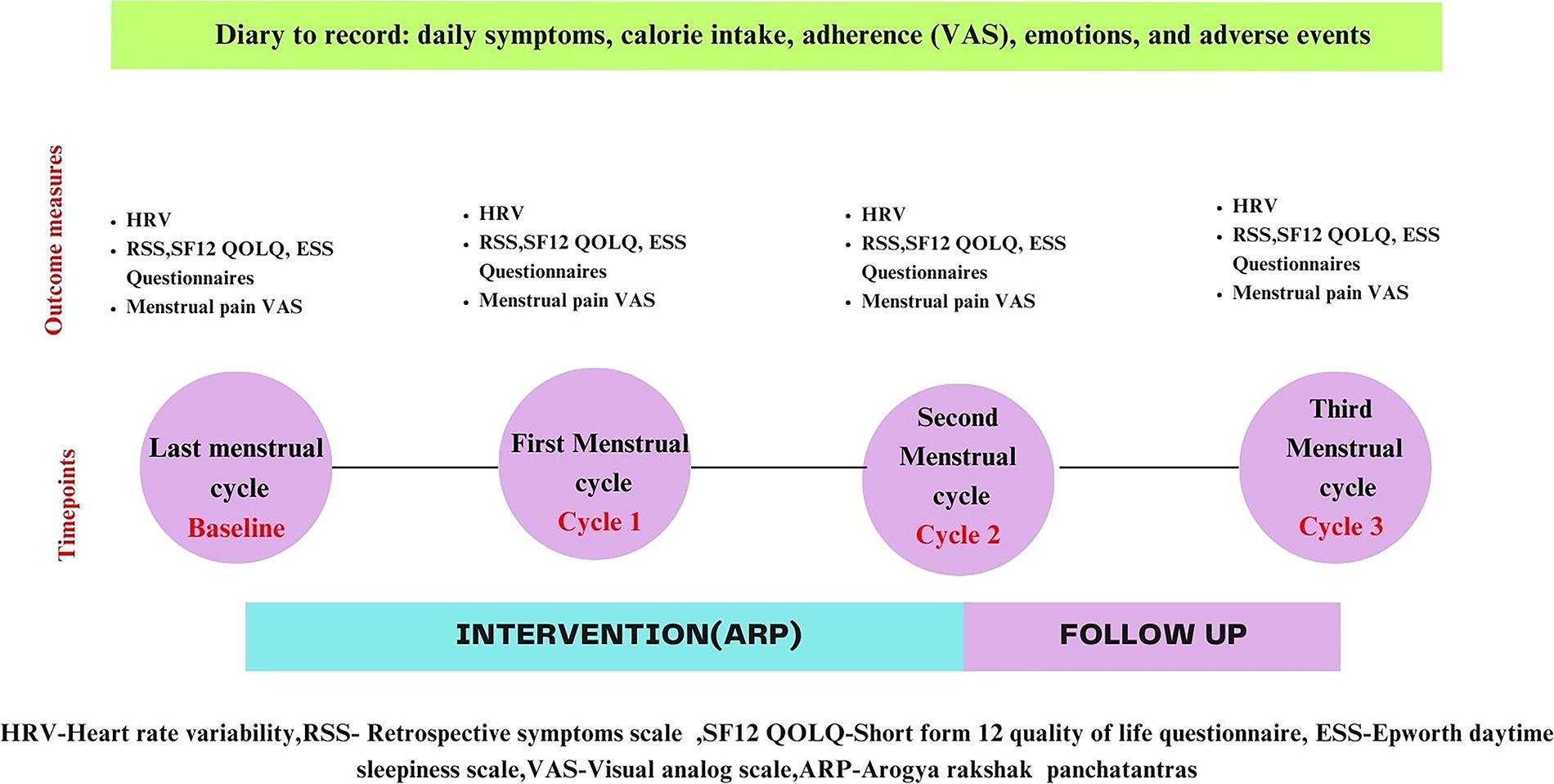
Time points for the assessment of outcome variables.
Primary outcome assessment
Heart rate variability
HRV was recorded using a digital physiograph (Recorders and Medicare Systems Private Limited, Chandigarh, India). The time domain indices of HRV included standard deviation of all NN intervals (SDNN), root mean square of successive differences between normal heartbeats, number of pairs of adjacent NN intervals differing by more than 50 ms in the entire recording (NN50), and percentage of successive NN intervals that differ by more than 50 ms from the total number of NN intervals (pNN50). The frequency domain indices measured were low frequency (LF) component, high frequency (HF) component, and ratio of LF to HF (LF/HF ratio). Also, heart rate (HR) and RR interval (the duration between two successive RR waves) were captured.
Secondary outcomes assessment
Retrospective symptom scale
The study utilized the RSS to measure participants’ experiences during their last menstrual cycle. The RSS assesses 18 common menstrual symptoms, with ratings for frequency (0–4) and severity (0–4). The sum of incidence and severity ratings for each symptom yields final scores. 23
SF-12 health-related quality of life questionnaire
The SF-12, a validated 12-item self-reported questionnaire, was used to measure health-related quality of life under two domains: The physical component summary (PCS) and the mental component summary (MCS). 24
Epworth daytime sleepiness scale
The ESS, comprising 8 questions, assesses daytime sleepiness levels on a scale of 0–24, with higher scores indicating increased daytime sleepiness . 25
Visual analog scale for pain
A 10-point linear VAS was used to record the subjective pain of the participants during the menstrual cycle.
Feasibility
To evaluate the feasibility, the study also monitored self-reported symptoms, emotions, adverse events, calorie intake, and adherence to the intervention.
Symptoms record diary
Participants in both the groups were provided with a daily diary to record any symptoms they experienced.
Calorie intake diary
To calculate daily calorie intake, participants in both the groups were asked to document the quantity of food items consumed using predefined utensils (spoons, bowls, and glasses) and/or specific quantities (grams).
Adherence record diary
Participants in the intervention group were asked to record daily adherence to the ARP using a visual VAS, a linear scale ranging from 1 to 10, with higher scores indicating better adherence.
Emotions record diary
Participants in both groups were asked to record their emotions using a single-word description (e.g., “Irritated”) throughout their menstrual cycles.
Safety
Adverse events data were collected from participants in both the groups throughout the intervention and follow-up period and classified as mild (grades 1 and 2) or severe (grades 3, 4, and 5) according to the Common Terminology Criteria for Adverse Events. 26 Serious adverse events were defined as events that were life-threatening, required hospitalization, or resulted in significant disability. The research team documented these events on the Adverse Event Page. Assigned in-charges were trained to promptly report any serious adverse events to the research team, with medical assistance ready if needed. Documentation was further supported by record in the participant’s daily symptom record.
Data analysis
The data from the intervention and control groups were captured and entered into Microsoft Excel. Subsequently, the data were exported to IBM Statistical Package for Social Sciences Version 27 for cleaning and analysis. Prior to analysis, the study variables were checked for missing data and inconsistencies in data entry by running the codebook and frequency tables. The continuous study variables (such as weight, SF 12 PCS, SF 12 MCS, SDNN, RSS score, NN50, and VAS pain) were assessed for normality using Q-Q plots and Shapiro–Wilk tests.
The baseline data, the calorie intake, and emotional status/mood changes and symptoms of dysmenorrhea across the intervention and control groups are analyzed descriptively. Given that multiple assessments were done across the study timeline (i.e., baseline versus cycle 1 versus cycle 2 versus cycle 3), we employed repeated measures analysis of variance to analyze for within group comparisons across the intervention timeline (i.e., baseline versus cycle 1 versus cycle 2 versus cycle 3) in the intervention and control groups. Bonferroni correction was applied to adjust for error associated with multiple comparisons. The generalized linear model (GLM) analysis was conducted to ascertain the effectiveness of the intervention on the study variables at each cycle. GLM was applied due to their ability to handle complex longitudinal data, to represent effectiveness of the intervention. Hedge’s g was computed as a measure of effect size. A p value of ≤0.05 was considered statistically significant.
Results
A total of 52 female participants randomized to the intervention (n = 26) and control (n = 26) groups were enrolled into the study. One participant in the control group opted out of the study before the initiation of the study leaving the control group with 25 participants. The total study sample who completed the study were 51 participants. Figure 2 shows the detailed profile of the trial (CONSORT chart). The average age of the participants was 21.14 (±2.28) years. The baseline demographic characteristics are presented in Table 1.
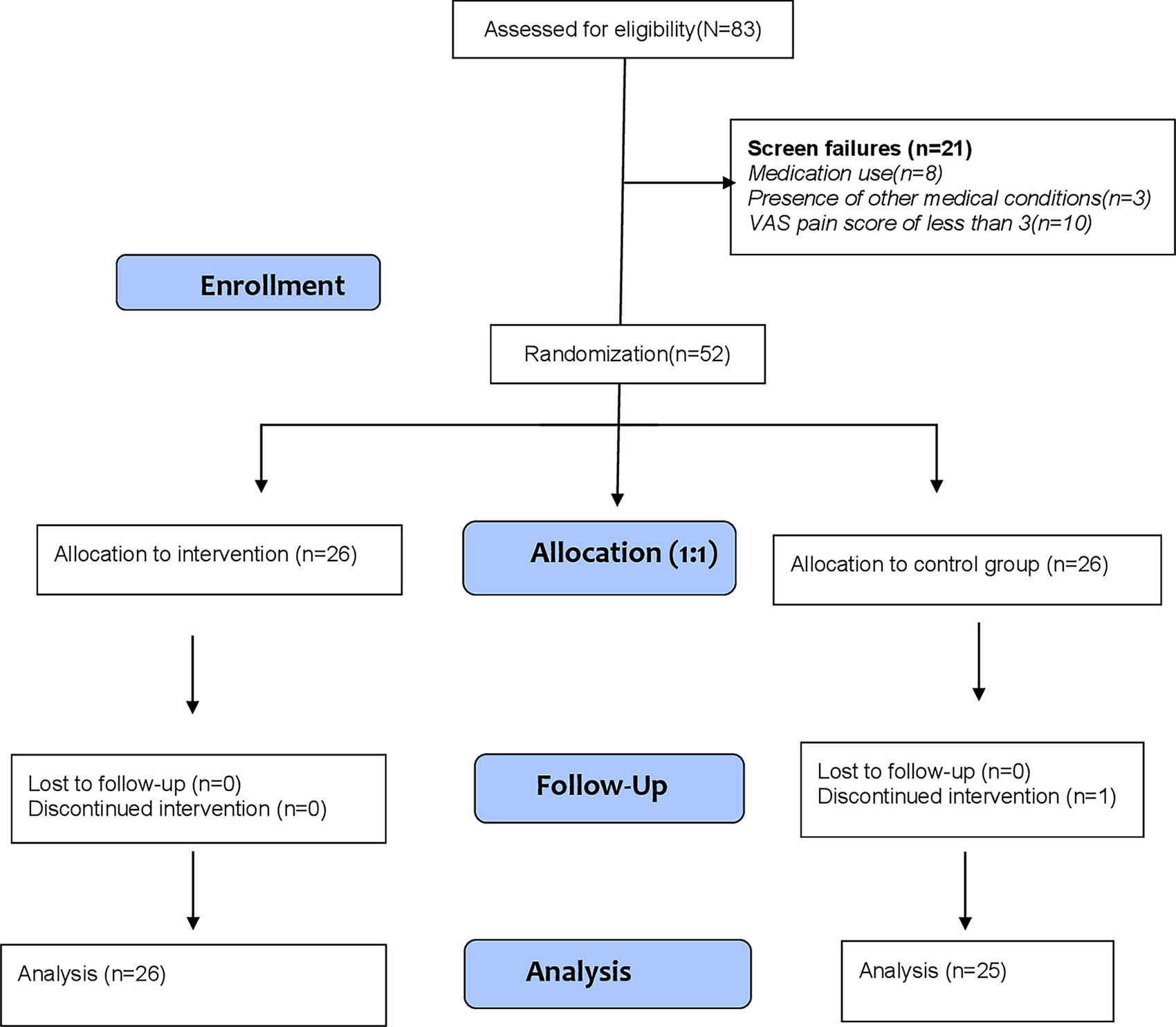
CONSORT Trial Profile.
Baseline Demographic and Clinical Characteristics of the Intervention and Control Group Participants
ESS, Epworth daytime sleepiness scale; HF, high frequency; LF, low frequency; NN50, number of pairs of adjacent NN intervals differing by more than 50 milliseconds in the entire recording; PNN50, number of pairs of adjacent NN intervals differing by more than 50 milliseconds in the entire recording; RMSSD, root mean square of successive differences between normal heartbeats; RSS, retrospective symptom scale; SD, standard deviation; SDNN, standard deviation of all NN intervals; SF12 MCS, short form 12 mental component summary; SF12 PCS, short form 12 physical component summary; VAS, visual analog scale; VLF, very low frequency.
Kilocalories.
Missing data were identified in 12 observations (six cases) in the intervention group and two observations (one case) in the control group, across variables including RSS score, ESS score, mean RR interval, and HR. The maximum number of missing data points per variable was two. Given the limited amount of missing data, the analysis was conducted following a per-protocol approach. However, a supplementary analysis using the intention-to-treat (ITT) approach was performed to ensure the reliability of the findings. For the ITT analysis, missing observations were imputed using the last observation carried forward method.
Effectiveness of ARP
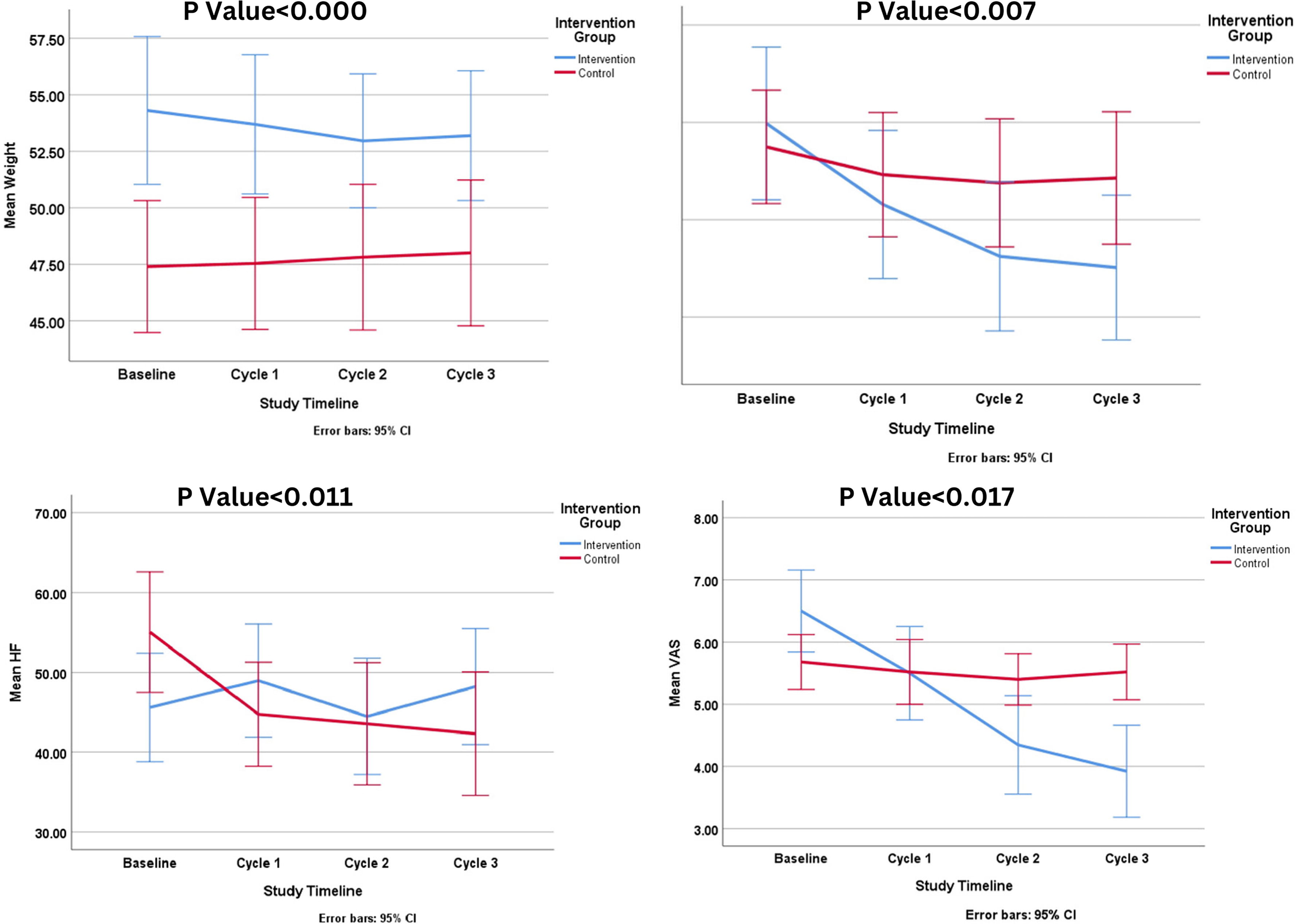
The repeated measures analysis of variance by ranks showed that among the participants in the intervention group there was a significant reduction in the weight (n = 26, baseline: 54.31 (±8.10), Cycle 3: 53.19 (±7.11), p = 0.008), RSS score (n = 26, baseline: 59.77 (±38.86), Cycle 3: 30.15 (±36.84), p = 0.008), ESS score (n = 26, baseline: 7.69 (±3.06), Cycle 3: 6.65 (±4.32), p = 0.039), and VAS pain (n = 26, baseline: 6.50 (±1.63), Cycle 3: 3.69 (±2.16), p = 0.000) (see Table 2). In control group, significant difference was observed in PNN50 (p = 0.023) and HF (p = 0.026) measures of HRV (see Table 3).
Employing generalized linear model, we observed the significant effectiveness on ARP on the HF component of HRV (Cycle 1: ES = 0.195, p = 0.016; Cycle 2: ES = 0.064, p = 0.046; Cycle 3: ES = 0.150, p = 0.007), weight [Cycle 1: Effect Size(ES) = 0.836, p = 0.011; Cycle 2: ES = 0.680, p = 0.006; Cycle 3: ES = 0.695, p = 0.017], VAS pain (Cycle 1: ES = 0.572, p = 0.000; Cycle 2: ES = 1.198, p = 0.000; Cycle 3: ES = 1.489, p = 0.000), and RSS (Cycle 1: ES = 0.435, p = 0.134; Cycle 2: ES = 0.721, p = 0.068; Cycle 3: ES = 0.782, p = 0.011), (see Table 4). However, no significant changes were observed in terms of other components of HRV, quality of life, and ESS. The analysis was conducted employing a per-protocol approach. The significant results are illustrated in Figure 3. A further supplementary analysis applying the intention to treat principle revealed significant effectiveness of ARP on weight, VAS pain, RSS, and HF measures (see Supplementary Data S2).
Changes in Study Variables Across Intervention Timeline (n = 26)
Repeated measures ANOVA, Bonferroni correction was applied for multiple comparisons.
ANOVA, analysis of variance; DBP, diastolic blood pressure; ESS, Epworth daytime sleepiness scale; HF, high frequency; LF, low frequency; NN50, number of pairs of adjacent NN intervals differing by more than 50 milliseconds in the entire recording; PNN50, percentage of successive NN intervals that differ by more than 50 ms from the total number of NN intervals; RMSSD, root mean square of successive differences between normal heartbeats; RSS, retrospective symptom scale; SBP, systolic blood pressure; SDNN, standard deviation of all N-N intervals; SF12 MCS, short form 12 mental component summary; SF12 PCS, short form 12 physical component summary; VAS, visual analog scale; VLF, very low frequency.
Changes in Study Variables in the Control Group (n = 25)
Repeated measures ANOVA, Bonferroni correction was applied for multiple comparisons.
ANOVA, analysis of variance; ESS, Epworth daytime sleepiness scale; HF, high frequency; LF, low frequency; NN50, number of pairs of adjacent NN intervals differing by more than 50 milliseconds in the entire recording; PNN50, number of pairs of adjacent NN intervals differing by more than 50 milliseconds in the entire recording; RSS, retrospective symptom scale; RMSSD, root mean square of successive differences between normal heartbeats; SDNN, standard deviation of all N-N intervals; SF12 MCS, short form 12 mental component summary; SF12 PCS, short form 12 physical component summary; VAS, visual analog scale; VLF, very low frequency.
Summary of the changes in the outcome measures.
Impact of ARP on Study Variables: Analysis of Generalized Linear Model Analysis
Generalized linear model were used to assess the effectiveness of ARP.
ARP, Arogya Rakshak Panchatantra; BP, blood pressure; ES, effect size, calculated as Hedge’s g; ESS, Epworth daytime sleepiness scale; HF, high frequency; LF, low frequency; NN50, number of pairs of adjacent NN intervals differing by more than 50 milliseconds in the entire recording; PNN50, number of pairs of adjacent NN intervals differing by more than 50 milliseconds in the entire recording; RMSSD, root mean square of successive differences between normal heartbeats; RSS, retrospective symptom scale; SDNN, standard deviation of all NN intervals; SF12 MCS, short form 12 mental component summary; SF12 PCS, short form 12 physical component summary; VLF, very low frequency; VAS, visual analog scale.
Emotional status associated with menstruation across the intervention and control groups
Both intervention and control group participants experienced similar major mood changes, including irritability, anxiety, depression, and anger. Both groups showed a reduction in these symptoms from baseline to the third follow-up cycle, but the difference between the groups was not significant (see Table 5).
Changes in the Emotional Characteristics of Dysmenorrhea Among Intervention and Control Groups
Changes in symptoms across the intervention and control groups
Variability was noted in experienced dysmenorrhea symptoms including headache, fever, weakness, body pain, constipation, cold, and diarrhea. Headache emerged as the most prevalent symptom in both groups, with its prevalence decreasing from 43% to 23% in the intervention group and from 28% to 16% in the control group. Diarrhea was reported by 3% of participants in the intervention group only during the initial month and by 5% of participants in the control group during the third month.
Regarding the symptom days, in the intervention group, the frequency of symptoms decreased from 112 symptom days in cycle 1 to 35 symptom days in cycle 3, whereas in the control group, the frequency decreased from 64 symptom days in cycle 1 to 19 symptom days in cycle 3 (see Fig. 4).
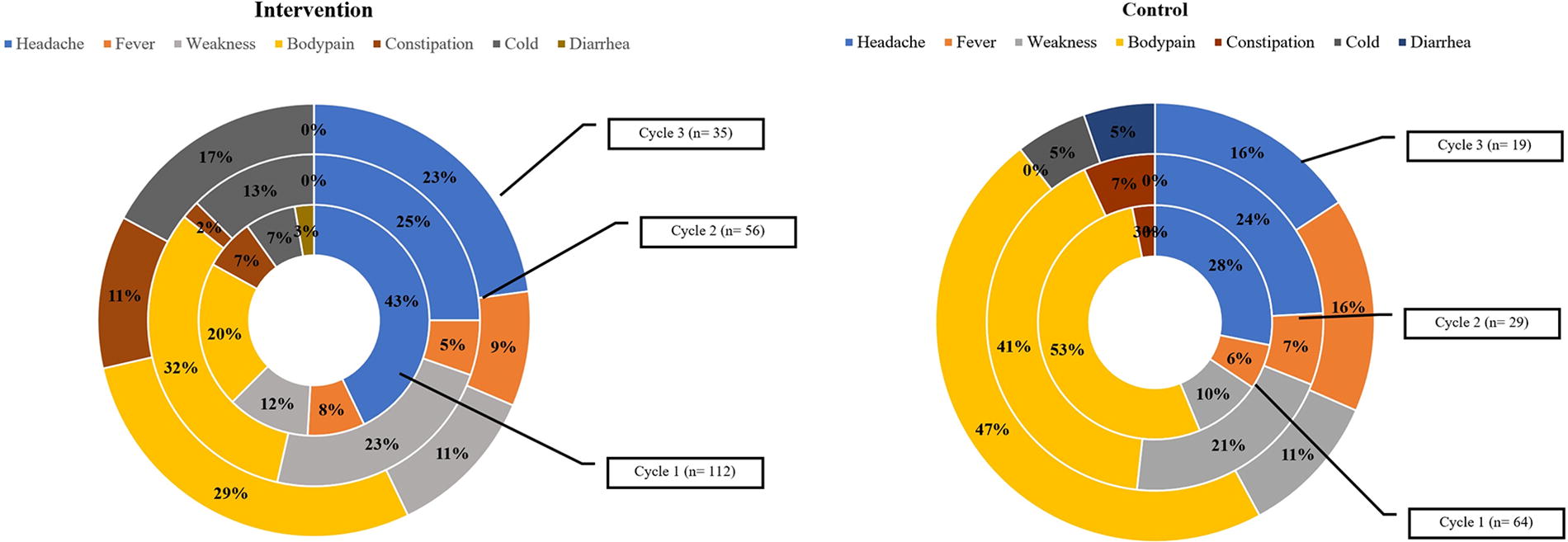
Comparison of symptoms of dysmenorrhea among the intervention and control group participants.
Adherence to ARP
The average adherence percentage was computed to be 77% in the intervention group.
Calorie intake reported across groups
There was no significant difference observed in terms of total calorie intake between the groups. However, calorie consumption increased over the intervention period in the experimental group. This trend in calorie intake is depicted in Figure 5.
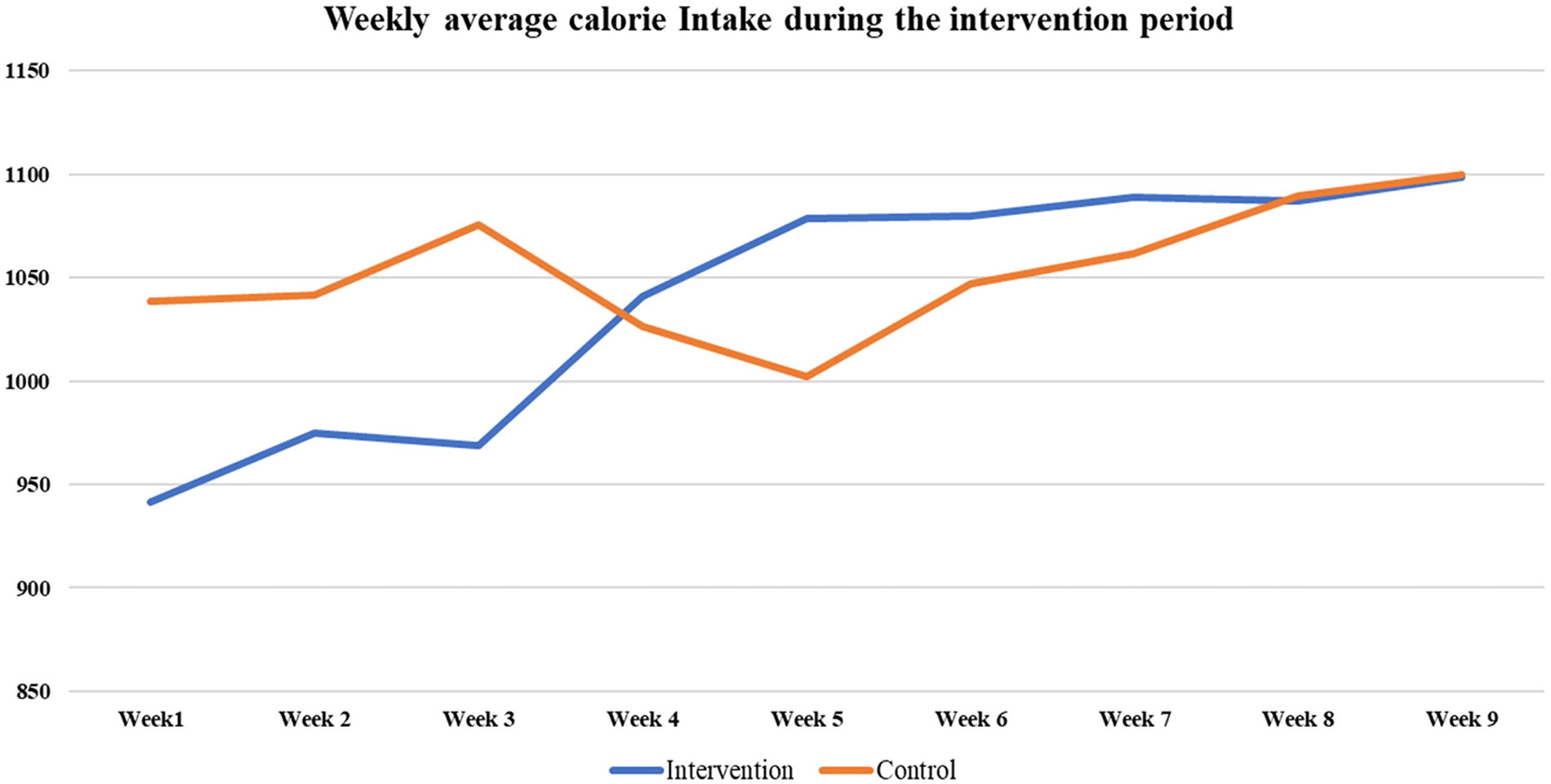
Weekly average calorie intake during the intervention period.
Safety
Although participants in both groups reported mild symptoms, none of the participants reported any serious adverse events (see Table 6).
Safety Data Across the Study Group During the Trial Period
Number of events reported by the study participants during the study period. Participants reporting similar symptoms on each day or more than one symptom on the same day are considered separate events.
Discussion
In our study involving 51 participants, we examined the long-term effects of ARP on dysmenorrhea. Our main findings revealed improvements in selected HRV components as well as significant reduction in menstrual distress and pain evaluated through RSS and VAS, respectively. This is likely attributed to the potential impact of ARP in reducing inflammation and modulating the autonomic functions. Exercise, prayer, fasting, increased water intake, and less frequent eating all activate anti-inflammatory mechanisms, resulting in lower levels of prostaglandins, interleukin-6, CRP, and cortisol. 11,17,18,19,20 Additionally, these interventions promote the release of endogenous opioids, enhance pain tolerance thresholds, and improve uterine blood flow, all of which may contribute to these improvements. 11,15,27,28
Dysmenorrhea and other pain conditions are associated with heightened sympathetic activity, decreased vagal parasympathetic activity, and low HRV. 29 In our study, we observed improvements only in the HF component of HRV in the intervention group, suggesting increased parasympathetic activity. However, there were no improvements in other domains of HRV, which prevents the authors from making any conclusive statements about the role of ARP in modulating autonomic functions. Earlier studies suggest a significant negative correlation between HRV and inflammatory markers. 30,31 Nevertheless, our study contributes to the growing body of evidence supporting the potential role of ARP might play in restoring homeostasis and emphasizes the importance of incorporating such lifestyle principles in managing PD.
Emotional well-being is known to have a reciprocal relationship with dysmenorrhea. 1 In India, cultural and social taboos surrounding menstruation can further exacerbate negative emotions in females. 32 Participants reported mood changes such as irritability, anxiety, depression, and anger associated with dysmenorrhea. Both groups experienced a reduction in these emotions, likely due to breaking the taboo by discussing menstruation-related feelings. This underscores the need for emotional counseling alongside interventions like ARP for effective management.
In our study, we did not observe any serious adverse events, which suggests that the intervention is safe. However, as detailed in Table 5, some participants reported moderate adverse events such as headaches, common colds, body pain, diarrhea, constipation, fever, and weakness. These symptoms were transient, indicating that ARP could be considered a safe lifestyle approach for managing PD.
Additionally, our calculated average adherence percentage, at 77%, aligns well with or even exceeds adherence rates observed in previous clinical trials. 33,34 Adherence rates in this study were self-reported, potentially impacting reliability. Nonetheless, the findings suggest that behavior change strategies, including ARP, may be a feasible approach for managing PD. Despite weekly fasting in the intervention group, average calorie intake was similar between groups, with a gradual increase observed only in the intervention group. This trend might reflect improvements in appetite and digestion, as PD often causes symptoms like appetite loss, diarrhea, bloating, nausea, and vomiting that reduce calorie intake. Further research is needed to confirm this hypothesis.
Participants in the intervention group exhibited a higher frequency of symptoms as compared to the control group, particularly headaches, which aligns with the naturopathy concept of a “healing crisis.” This concept suggests that during detoxification (internal cleansing), the body may manifest various symptoms. 35 This can be explained by the “Jarisch-Herxheimer Reaction,” which illustrates how symptoms can emerge when lipoproteins and cytokines are released into the bloodstream at the onset of antibiotic treatment for infections. 36 It is hypothesized that our intervention similarly activated detoxification mechanisms, causing symptoms like headaches, diarrhea, fever, and body pain. Further research is needed to understand this phenomenon fully.
No significant improvements were found in quality of life or daytime sleepiness between the groups. Despite improvements in menstrual distress and HRV, the lack of significant findings may be due to the small sample size, the short intervention duration (two months), or the use of general measurement tools (SF-12 QOLQ and ESS) that may not adequately capture dysmenorrhea-specific dimensions. Further studies with larger samples, longer interventions, and condition-specific tools are needed to confirm these findings.
Limitations of the study
This study has several limitations, including the absence of inflammatory blood markers and data on prior ARP exposure, which could act as confounding factors. The lack of blinding may have introduced response and bias errors, while the homogeneous population and person-to-person recruitment limit generalizability and suggest potential selection bias. Due to limited evidence on ARP, we used the effect size measure of a previous study (using physical activity) for our sample size estimation. This could have impacted the power of our study sample. Additionally, the reliance on self-reported VAS lacks specificity. Future research should address these limitations by incorporating larger, more diverse samples, extending intervention duration, using dysmenorrhea-specific tools, evaluating cost-effectiveness, and exploring optimal ARP implementation strategies. Despite these limitations, health care providers may consider ARP for managing PD due to its observed benefits.
Conclusion
This study suggests that traditional lifestyle principles like ARP may help reduce symptoms of PD. Further research is needed to explore the long-term benefits and cost-effectiveness of ARP.
Footnotes
Authors’ Contributions
Conceptualization: P.M.K.N., K.S., and H.S. Data collection, management, analysis, and interpretation of data: P.B.K., K.S., P.B., J.M., and P.M.K.N. Writing—original draft: P.M.K.N., K.S., and P.B.K. Writing—review and editing: P.M.K.N., H.S., G.T., and P.B.K.
Informed Consent
Informed consent was obtained from all individuals included in this study before enrollment.
Ethical Approval
The study protocol was approved by the Institutional Ethics Committee of Sant Hirdaram Medical College of Naturopathy and Yogic Sciences via F.No:12/SHMCNYS-IEC/P22/2022–2023.
Author Disclosure Statement
The authors state no conflict of interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.