
Abstract
Introduction:
Pain management clinics differ in treatments offered, and little evidence exists regarding which combinations of therapies result in best outcomes. This study analyzed clinical encounters and pain outcomes data for associations between treatment composition and outcomes.
Methods:
Retrospective observational study of 2,142 predominantly active-duty US service members referred to an interdisciplinary pain management center between 2014 and 2021. Latent class analysis was used to identify treatment groups with distinct outcome patterns during the year following initial assessment. The primary outcome measure was the National Institutes of Health Task Force on Research Standards for Chronic Low-Back Pain impact score.
Results:
Four distinct treatment groups were identified: 1 group engaged in conventional medical therapies alone (n = 726, median 3.5 treatment hours), and 3 groups used a combination of conventional, psychological, rehabilitative, and complementary therapies, with different levels of treatment hours: low (n = 814, median 15.7 h), medium (n = 177, median 40.1 h), and high (n = 425, median 72.5 h). All groups showed significant improvement in pain impact score from baseline up to 9 months but not at 12 months following initial assessment. At the 6-month time point, the group with high multimodal treatment hours had the most improvement in pain impact (−3.1 [95% CI −3.8, −2.4]) compared with the group using only conventional therapies (−1.0 points [95% CI −1.8, −0.1]) or with low multimodal treatment hours (−1.3 points [95% CI −1.9, −0.7]). There were no between-group differences at the 9- or 12-month time points.
Conclusion:
These results suggest that a combination of pain therapy approaches results in greater reduction in pain impact than the use of conventional medical treatment alone for up to 6 months after initiating therapy and that there may be a threshold of treatment hours that must be exceeded to achieve this benefit.
Clinical trial registration:
As this study is not a clinical trial, no registration was required.
Introduction
Five broad categories of treatment approaches are recommended for chronic pain: (1) medications, (2) rehabilitative approaches (e.g., physical and occupational therapies), (3) interventional approaches (e.g., joint injections, epidural steroid injections), (4) behavioral health approaches (e.g., cognitive behavioral therapy [CBT]), and (5) complementary and integrative health (CIH) approaches (e.g., acupuncture and yoga). 1 Available therapies and approaches vary widely from one pain management clinic to another. The conventional medical approach to pain includes both medication guidance and/or management and interventional procedures, and most pain clinics offer these options. Far fewer clinics offer comprehensive pain management programs which include medications, behavioral health, and rehabilitative approaches. 2 –4 Even fewer offer CIH approaches as well. 5 There is little in the current literature that compares the effectiveness of combinations of these approaches. 4,6 –9
To address this gap, this retrospective observational study evaluated patients of an interdisciplinary pain management center that offers all five approaches for chronic pain and evaluated change in pain impact during the 1 year following initial referral. The aim was to determine if specific combinations of therapies are associated with greater improvement in pain impact. The expectation was that greater variety and intensity of therapies would be associated with greater improvement in pain impact compared with treatment involving conventional medical approaches alone.
Design and Intervention
Design and setting
This retrospective observational study used data collected as standard of care at the Madigan Army Medical Center (Madigan) Interdisciplinary Pain Management Center (IPMC). After approval by the Madigan Institutional Review Board (#218052), the study analyzed deidentified medical records and pain assessment data from patients receiving care at the IPMC between 2014 and 2021. The Madigan IPMC, located on Joint Base Lewis-McChord in Tacoma, Washington, provides medication management, interventional procedures, and interdisciplinary pain management programs that include behavioral, rehabilitative, and CIH therapies. The patient population is primarily active-duty service members, with a small percentage (9%) of retired veterans and family members of military beneficiaries. The interdisciplinary pain management programs, however, have limited capacity and are available only to service members on active duty (including activated Guard and Reserve).
Intervention
Active-duty service members referred to the IPMC between 2014 and 2021 attended an orientation that included an overview of the available treatment options. Following the orientation, they underwent a comprehensive medical assessment and a treatment plan was proposed, which could include medications, interventional procedures, group-based CBT for chronic pain, and/or an interdisciplinary pain management program. Physical, occupational, and CIH therapies were offered only as part of an interdisciplinary program and were not available as individual therapies. Service members who completed the standard interdisciplinary pain management program and were continuing to make progress at its conclusion were offered the option of a more intensive program (Fig. 1). All therapies were provided at no cost to IPMC patients.

IPMC patient flow diagram. Following initial assessment by a medical provider, care may involve medications and/or interventions and/or interdisciplinary programs. Arrows indicate typical flow; patients progress along the path only if it is clinically indicated and they can commit the time required. Patients are prompted to complete PASTOR assessments every 1–3 months while engaged in care. * Total hours for each program are adjusted for 17% of provider nonavailability due to leave, holidays, etc. ACT, acceptance and commitment therapy; IPMC, interdisciplinary pain management center; OT, occupational therapy; PA, physician assistant; PASTOR, pain assessment screening tool and outcomes registry; PT, physical therapy.
Measures
Data were drawn from the Pain Assessment Screening Tool and Outcomes Registry (PASTOR), a computer-based survey of standard outcome measures used in US military pain specialty clinics. 10 All IPMC patients were asked to complete PASTOR at the time of their initial IPMC visit and every 1 to 3 months for up to 1 year. PASTOR includes several validated scales that were included in the present analysis.
The primary outcome measure for this analysis was the pain impact score (PIS) from the National Institutes of Health Task Force on Research Standards for Chronic Low-Back Pain. The PIS is a composite score of pain intensity, pain interference, and functional status and was computed using three scales: (1) average pain intensity during the previous 7 days as assessed by the Defense and Veterans Pain Rating Scale, a validated scale with scores ranging from 0 (“no pain”) to 10 (“as bad as it could be, nothing else matters”); 11 (2) Patient-Reported Outcomes Measurement Information System (PROMIS) Pain Interference, 12 which assesses interference of pain in physical, psychological, and social functioning; and (3) reverse PROMIS Physical Function, 13 which assesses physical function in daily activities. The PIS has a range of 8 (least impact) to 50 (worst impact) and an estimated minimal clinically important difference of a decrease of 3 points. 14 Scores of 26 and lower are proposed as “mild,” 27 to 34 as “moderate,” and 35 or higher as “severe.” 15 All PROMIS scales are reported in T-scores, with a range of 0 to 100 (mean = 50, SD = 10), and have been validated in both clinical and nonclinical samples. 16 –22
The study also compared baseline PROMIS measures of anxiety, depression, sleep-related impairment, and fatigue between treatment groups. 17,18,20 Higher scores in these scales indicate worse symptoms or status, with a score range of 55 to 59 designated as “mild,” 60 to 69 as “moderate,” and 70 or higher as “severe.” 17 PROMIS satisfaction with social roles was also assessed, for which higher scores indicate greater satisfaction. 21 Computer-adaptive testing formats were used for all PROMIS measures. Patient demographics including age, biological sex, military status, education, and income level were also assessed.
Data analysis
Stata/BE v.17 (StataCorp LLC) was the primary software used for data analysis. The distributions of treatment hours and PIS (primary outcome) during the year following initial intake were assessed. For the analysis, patient encounters were assigned to the treatment categories based on the discipline of providers: (1) conventional medical appointments (medical evaluations, prescriptions, and procedures); (2) clinical pharmacology; (3) nurse case management; (4) nursing education; (5) psychology (primarily CBT); (6) rehabilitative approaches (i.e., physical and occupational therapies); and (7) CIH therapies (chiropractic, acupuncture, yoga, and massage). For each patient, total treatment hours were calculated by summing the duration in minutes for all encounters within the treatment category. Appointment duration was imputed where missing from the mean appointment duration for the treatment category. Due to skewed distributions, variables for total treatment hours were categorized into three categories: (1) none/low, (2) medium, or (3) high treatment hours. The none/low category included patients with no treatment in the discipline and a median split was used to create the medium and high groups. The exception was medical treatment which was split by thirds based on the variable’s distribution as almost all patients had medical encounters in the IPMC.
Latent GOLD v.6 (Statistical Innovations) was used to conduct latent class analysis to group patients by the duration of treatment received in various disciplines, using the posterior probabilities from the model. 23 Baseline characteristics were then compared between patients assigned to each latent class (i.e., treatment group). Finally, a mixed regression model was conducted to model the change in PIS across time for patients assigned to different treatment groups. A quadratic term was added to the model to allow for nonlinear change across time. Response rates were calculated from the PIS scores predicted for patients via the regression model at selected time points.
Results
Model fit statistics for the latent class analysis are presented in Table 1. The Bayesian and Akaike information criteria, Vuong-Lo-Mendell-Rubin, and bootstrapped likelihood ratio tests all showed improvement in model fit with each additional class added. It was determined from the model fit likelihood ratio test that the 4-class model was the most parsimonious model that adequately fit the data. All models assessed met or exceeded the 80% cutoff for adequate entropy.
Model Fit Statistics by Number of Classes
The lowest number of latent classes with a p-value >0.05 is considered the best fit. In this case, the best fit was the model with 4 classes.
Entropy at an omnibus index of >0.8 indicates good classification.
AIC, akaike information criterion; BIC, bayesian information criterion; LL, log likelihood; LR, likelihood ratio; N, number of parameters; VLMR LR, vuong–Lo–Mendell–Rubin likelihood ratio test.
Figure 2 displays the range of treatment hours by discipline for patients assigned to treatment groups based on the 4-class model. Overall, the 4 groups fell into the following patterns: conventional medical care (e.g., medical evaluation, medications, and/or interventional procedures) versus 3 levels (low, medium, and high) of multimodal care that included conventional, behavioral, rehabilitative, and CIH approaches. For the conventional and multimodal low, medium, and high groups, the median treatment hours were 4, 18, 43, and 74 and the median number of encounters were 5, 24, 55, and 90. Patients in the conventional care group had a median of 4 medical encounters (2.5 treatment hours) and a median of zero encounters/hours for any other treatment category. Patients in the 3 multimodal classes all received a similar amount of conventional care (3–4 encounters/2-2.5 h). In addition, patients in the low multimodal treatment group had lower median amounts of psychology (2 encounters/2 h), rehabilitative (4 encounters/2.5 h), and CIH therapies (8 encounters/3.75 h). Patients in the medium multimodal treatment group had a higher median amount of psychology (8 encounters/8 h), rehabilitative (21 encounters/15.1 h), and CIH therapies (21 encounters/15.5 h). Patients in the high multimodal treatment group had slightly higher total median hours of psychology (9 encounters/9 h) and CIH therapies (25 encounters/16 h) than the medium multimodal treatment group, and notably higher median hours of rehabilitative approaches (42 encounters/35.5 h). Case management hours were low for all 4 groups (median of 0 or 1 encounters/hours), except for the high multimodal treatment group, which had a median of 6 encounters/4 h of case management. Median nursing education encounters/hours were 0 for all groups except for the high multimodal treatment group, which had 1 encounter/0.75 h of education. The specific amounts of CIH encounters/hours varied by the low, medium, and high multimodal groups as follows: acupuncture: 1/1, 6/5.4, 10/9.5; chiropractic: 4/1.8, 6/2.3, 10/3.5, massage: 0/0, 3/3, 0/0; yoga: 0/0, 4/4, 2/2.
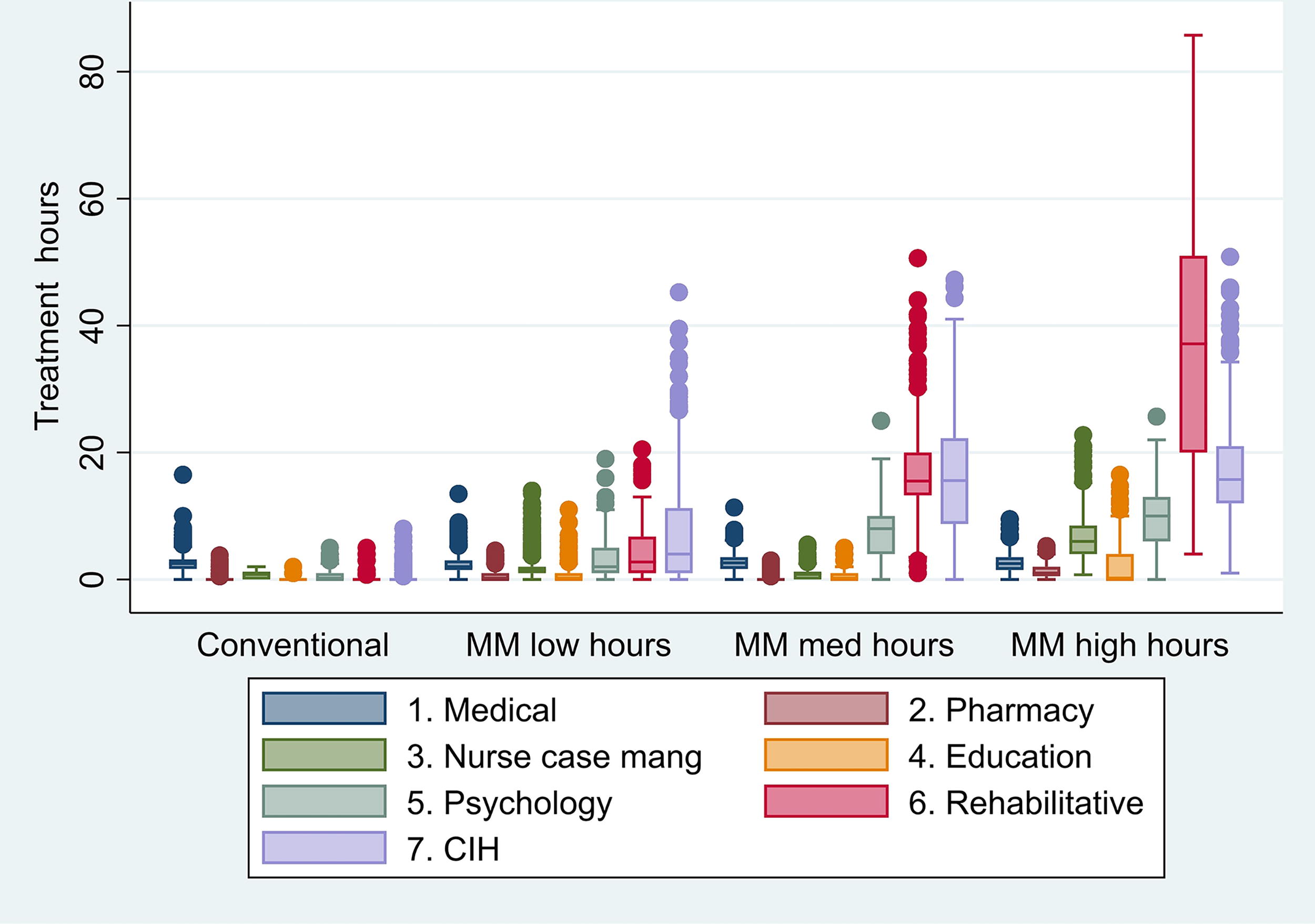
Treatment hours by discipline for patients assigned to the four latent classes. CIH, complementary and integrative health; med, medium; mang, management; MM, multimodal.
At baseline, there were many demographic differences between patients grouped by latent class (Table 2 and Table 3). Compared to the three multimodal treatment groups, the conventional medical treatment group had a higher percentage of patients who were older than 35 years and had a higher military rank, higher education (past high school), an income of $50,000 or more, and pain that did not limit their work hours. The conventional treatment group also had a higher percentage of patients who had retired from active service. Compared to the other groups, the medium multimodal treatment group had a higher percentage of patients whose education was limited to high school and who identified as non-Hispanic White. The predominant pain type was musculoskeletal with a between-group range of 84.5% to 91.1%. Differences in the baseline self-report PASTOR assessments showed that patients in the conventional medical treatment group had zero to 0.3 points lower mean pain intensity scores and slightly better (1.0–3.7 points) mean scores on all PROMIS measures, than those in the other treatment groups.
Patient Demographic and Clinical Characteristics by Latent Class (Treatment Group)
Conventional medical treatment includes medical evaluation, medications, and/or interventional procedures.
Multimodal treatment includes a combination of conventional medical treatment with psychological, rehabilitative, and complementary and integrative health therapies.
Group diff = p-value of omnibus test for group differences. Bolded values indicate statistical significance at the p < .05 level.
Pain type determined by International Classification of Diseases (ICD) – 9th or 10th revisions diagnoses codes used for initial IPMC encounter by a medical provider (physician, nurse practitioner or physician assistant).
Classified as “musculoskeletal” type if: 1. 1st coded diagnosis by a medical provider was a musculoskeletal code (ICD-9 710-739 or ICD-10 M00-M99 ranges), or 2. 1st coded diagnoses was a “pain, not elsewhere classified” (NEC) code (ICD-9 338.* or ICD-10 G89*) or “pain, unspecified” (ICD10 R52*) code and 2nd coded diagnosis was a musculoskeletal code.
Classified as “nervous system condition” if: 1. 1st coded diagnosis was a “nervous system condition” code (ICD-9 323* – 359* or ICD-10 G01 - H99) excluding a “pain, NEC” (338* or G89*) code, or 2. 1st coded diagnosis was a “pain, NEC” code or “pain, unspecified” (ICD10 R52) code and 2nd coded diagnosis was a “nervous system condition” code, excluding a “pain, NEC” or a “pain, unspecified” code.
Classified as “other” if Both 1st and 2nd coded diagnoses were codes not meeting above criteria for “musculoskeletal” or “nervous system condition.”
Classified as “missing” if: No diagnosis was coded by a medical provider for any IPMC encounters for that patient.
Asterisk at end of ICD code indicates that the 3 digit ICD code may be followed by a decimal point and any combination of numerals for each category of diagnoses.
Mean Baseline Self-Report PASTOR Scores by Latent Class (Treatment Group)
The omnibus test for group differences was significant for all measures at p < 0.01.
Conventional medical treatment includes medical evaluation, medications, and/or interventional procedures.
Multimodal treatment includes a combination of conventional medical treatment with psychological, rehabilitative, and complementary and integrative health therapies.
Figures 3 and 4 show the changes in PIS over time in the different treatment groups. All groups showed significant improvement in PIS compared to baseline up until the 9-month time point, but not at the 1-year time point. The high multimodal treatment group showed significantly greater improvement in PIS at 6 months compared to the conventional and low multimodal treatment groups, but by the 9-month time point, there were no significant differences between groups. The percent of responders (meaning those whose PIS decreased by at least 3 points) calculated from the mixed regression model, was largest in the high multimodal treatment group at 3 and 6 months and largest in the medium multimodal treatment group at 9 and 12 months. Changes in the components of the PIS were also assessed. Pain interference improved for all groups through 9 months. The high multimodal group improved more than the conventional and low multimodal group through 9 months (−1.5 [−2.6, −0.5]). and (−1.3 [−2.3, −0.3]). Physical function improved significantly for the high multimodal group only through 6 months and significantly more than the low multimodal group (6 months: 0.9 [0.3, 1.6]). Pain intensity improved through 9 months for all groups and through 12 months for the medium multimodal group, which showed significant improvement compared to conventional treatment at one year (−0.7 [−1.5, −0.05]).
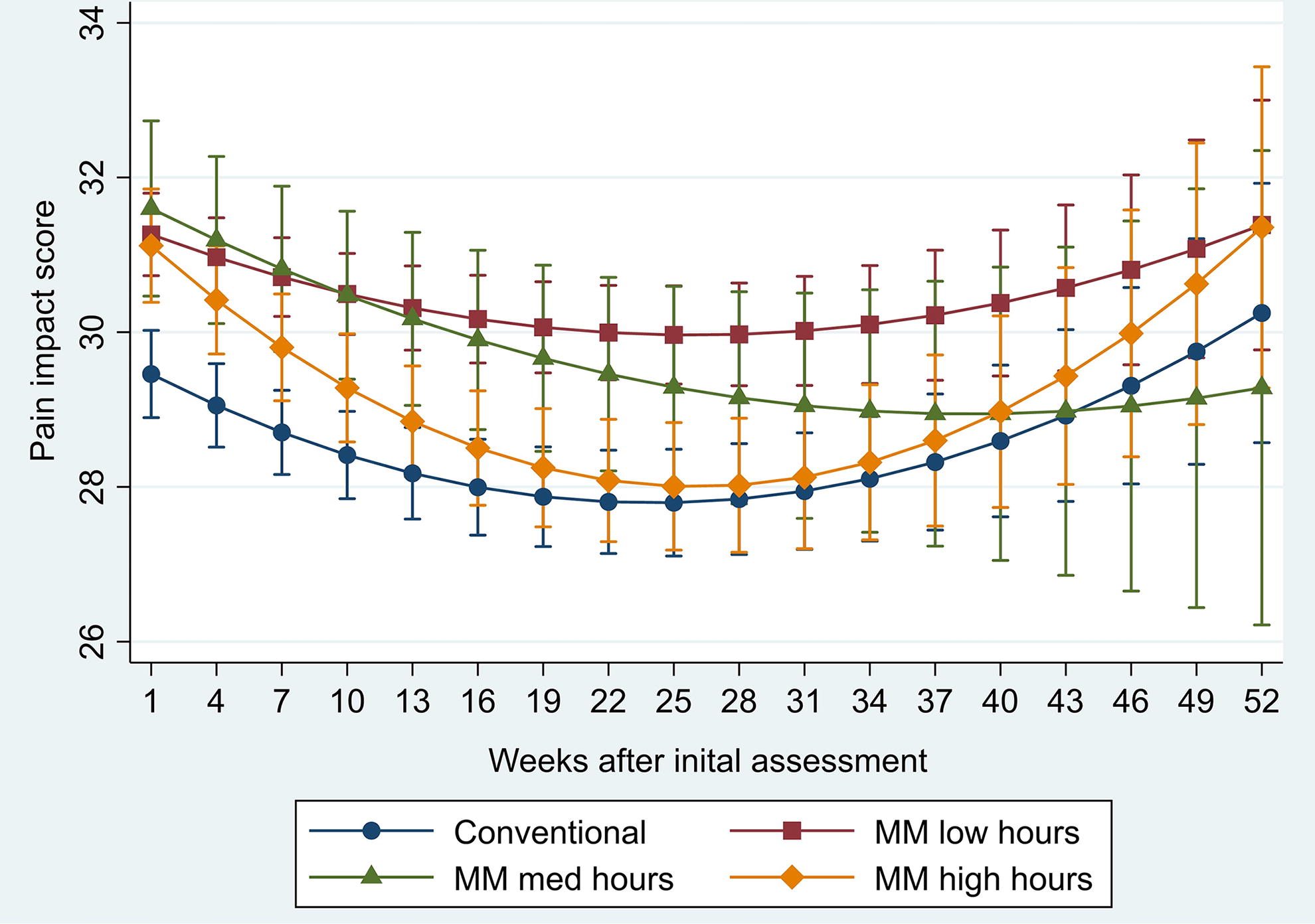
Predicted pain impact score by week following initial IPMC assessment for patients receiving different levels of treatment. IPMC, interdisciplinary pain management clinic; med, medium; MM, multimodal treatment.

Change in pain impact score from baseline by latent class (treatment group) and time point, with associated response rate and significant between-group differences. Response, decrease in pain impact score of at least 3 points from baseline. *p < .05; **p < .01; ***p < .001. Asterisks next to bars on graph represent significant change from baseline score for that group. Asterisks next brackets represent significant differences in change from baseline between groups. M, multimodal care; PIS, pain impact score.
Discussion
The key finding from this analysis was that multimodal pain care resulted in greater improvement in mean pain impact than conventional medical therapies alone, but only when multimodal treatment hours were high. When considering the variation in PIS trends over time (Fig. 3) in the context of IPMC patient flow (Fig. 1), it appears likely that in general, the group of patients receiving conventional therapies alone were those who were not recommended for, or declined to enroll in, interdisciplinary pain management. It is notable that this group had demographic characteristics consistent with a lower risk of having chronic pain (higher income, more educated) and pain that was not high impact (did not limit work hours and lower impact score). The groups with low and medium multimodal treatment hours likely represent patients who enrolled in the standard interdisciplinary pain management program with lower and higher levels of engagement, respectively, while the group with high multimodal treatment hours was likely those who engaged in both the standard interdisciplinary pain management program and the more intensive interdisciplinary program that followed. In other words, treatment response was likely influenced by both the combination of treatments offered and patients’ willingness and/or ability to fully engage in the offered treatments. Treatment response may also reflect clinical differences in patients who completed more or less intensive treatment. Short-term response rates were highest in the multimodal medium and high groups (33% and 53% at 6 months) but only appear to be sustained for the medium multimodal group at 12 months (39% vs. 22%). The trend of sustained improvement in the medium but not high multimodal groups may reflect a patient population in intensive treatment with more difficult to treat chronic pain.
These findings are consistent with a comparative effectiveness analysis that found that despite beginning with worse baseline pain status, patients who engaged in at least three visits with a clinical psychologist embedded in a multidisciplinary pain management program had similar improvements in pain outcomes and greater global impression of change 1 year later compared to patients who engaged in medication, injection, and/or physical rehabilitation treatments without psychological care. 8
This study’s findings are also consistent with an Agency for Health Care Research and Quality (AHRQ) evidence review of comprehensive pain management programs (defined in that review as clinics operating separately from a primary care setting that provide medication review and/or management, psychological support, and physical reconditioning) that was published in 2021. 4 That review found that when compared to pharmacologic therapy alone, comprehensive pain management programs yielded moderate improvement in pain and function immediately posttreatment and small functional benefit at short-term follow-ups (up to but not exceeding 6 months). 4 The AHRQ review also showed a small additional benefit in both pain and function at intermediate-term follow-ups (6–12 months) and a small additional benefit in function at long-term follow-ups (12 months or longer). 4
The current study findings are consistent with an earlier analysis of Madigan IPMC PASTOR data collected between 2014 and 2018. 24 That earlier study used generalized additive models to show that at 3 to 6 months after IPMC referral, PIS had improved significantly from baseline only in patients who had engaged in at least 30 total IPMC treatment hours, while progressively greater improvement was seen in patients with up to 90 treatment hours. 24 However, patients who had received 90 to 120 treatment hours showed progressively less improvement, and those with the highest number of treatment hours reported no improvement over baseline.
The current study’s finding of an association between higher treatment hours and greater benefit differs from a 2020 AHRQ evidence review of nonpharmacologic pain therapies that included multidisciplinary pain management programs for chronic low-back pain (defined in that review as programs including biopsychosocial components delivered by at least two disciplines). The 2020 review found that at short- and intermediate-term follow-ups, high-intensity multidisciplinary programs (i.e., 20 or more treatment hours per week or at least 80 h total) were not significantly more effective than less intense programs in improving pain and/or function. 6
Overall, these results suggest that efforts to determine if one approach is superior to another will require clinical trials that randomize patients to either conventional therapies alone or to low, medium, or high hours of multimodal therapies. The results of such trials can then provide evidence to bolster clinical recommendations to patients who may be interested in one path versus another (i.e., conventional therapies alone versus multimodal approaches), as well as to encourage patients enrolled in multimodal treatment programs to commit to their treatment plan. Future research should also seek to identify predictors of sustained treatment response to guide selection of patients for interdisciplinary programs who are most likely to maintain clinically significant improvement.
Limitations
This analysis was limited by its observational, retrospective nature. Patients were not randomized to treatments, and potential confounders may have influenced which care was offered and the level of care completed. Because there was no way to mask treatment assignment, patient expectations could have influenced their reported response.
Results collected at time points remote from intake may be less reliable due to fewer patients completing PASTOR assessments at later time points. Also, previous data analyzed by this research team determined that slightly over one-third (33.6%) of Army service members referred to the Madigan IPMC had begun or completed the military medical disability process within 1 year of referral. 25 Long-term treatment effects may be overestimated by the exclusion of those medically discharged from active service.
PASTOR assessments included both mid-treatment and posttreatment responses, which limit the ability to draw conclusions about the temporal/causal relationship between treatment hours and PIS change. Finally, results may be biased due to misclassification error when using the posterior probabilities of the latent class model to assign patients to groups. However, bias in the classify-analyze approach attenuates estimates, likely resulting in more conservative associations between treatment hours and pain impact. 26
Conclusions
This study’s findings suggest that a combination of conventional medical treatments with multimodal pain management approaches results in better short-term outcomes than medical treatments alone. An association was found between higher numbers of multimodal treatment hours and greater improvement in pain impact for up to 6 months following referral for pain treatment. However, by the 9- and 12-month time points, mean pain impact was not significantly different between the groups with low, medium, and high treatment hours, which suggests that greater dosage and variety of treatment approaches alone do not assure better outcomes. Methods to supplement treatment to achieve longer-term effects should be investigated.
Footnotes
Acknowledgments
The authors wish to extend their appreciation to Norma Bowling of Kennell and Associates, in support of the Defense Health Agency’s Enterprise Intelligence and Data Solutions Program Management Office, for her data management support. Kyra Freestar of Bridge Creek Editing provided professional editing support.
Authors’ Contributions
L.A.B., D.M.F., A.Z.D., and A.D.S. determined the study methodology and chose the variables to include. L.A.B. analyzed the data. L.A.B., D.M.F., A.Z.D., J.C.F., S.H.S., and A.D.S. wrote and edited the article. All authors reviewed and approved the article before submission.
Disclaimer
The views expressed are those of the authors and do not reflect the official policy of the Department of the Army, Department of Defense, National Institutes of Health, or the US Government. The investigators adhered to the policies for protection of human subjects as prescribed in 45 CFR 46.
Author Disclosure Statement
The authors have no conflict of interest to report.
Funding Information
This work was supported by the National Institute of Health (award number