
Abstract
Introduction:
The Mindfulness-Based Stress Reduction program for breast cancer survivors (MBSR [BCs]) is a stress-reducing program designed to increase cognitive functioning through four meditational practices. This randomized clinical trial aimed to determine if improvements in cognitive functioning and perceived cognitive abilities achieved from the MBSR(BC) were mediated through increased mindfulness, decreased rumination, and decreased perceived stress.
Methods:
Breast cancer survivors (BCSs) who met inclusion criteria of stage I, II, or III BC and received either chemotherapy (CT) or both CT and radiation were randomized to either the 6-week MBSR(BC), or Breast Cancer Education Support (BCES) program, or to a usual care (UC) regimen. Analysis of covariance was first implemented to identify potential mediators, followed by a formal mediational analysis to evaluate the effects of MBSR(BC) on 6-, 12-, and 26-week outcomes.
Results:
After consent, 212 BCS were randomized to MBSR(BC) (n = 91), BCES (n = 90), or UC (n = 31). The mean age was 56.5 and the majority of the BCS, 73.1%, were White and non-Hispanic. Results showed increases in “observing” as part of mindfulness as a potential mediator of MBSR(BC) effects on impairments on quality of life and logical memory at 6 months relative to UC. No mediation effects were identified for outcomes measured at 6 or 12 weeks and also when MBSR(BC) was compared with the BCES program.
Discussion:
These results partially supported our hypothesis that improvement in cognitive functioning would occur through increased mindfulness. Although few mediating relationships were identified, results showed a relationship between mindfulness and cognitive functioning. Both mediating relationships occurred through increases in “observing,” a subconcept of “mindfulness,” when compared to the MBSR(BC) with UC at 6 months. This study shows that mediators may help “optimize” clinical therapeutic treatment effects, thus contributing to the advancement of science. Trial Registration: ClinicalTrials.gov, www.ClinicalTrials.gov. Registration Number: NCT02786797.
Introduction
Breast cancer is the most common cancer in women, consisting of 32% of all new female cancers projected to be diagnosed in 2024. 1 Although 90% of breast cancer survivors (BCSs) survived more than five years since diagnosis, 1 advanced treatment with chemotherapy (CT) often result in significant psychological, physical, and cognitive problems impacting their quality of life (QoL). Cognitive impairment (CI) may result in deficits in executive functioning, attention, long- and short-term memory, and language fluency, that may persist for years after treatment ends. 2 Specifically, CI impacts the QoL of BCS by decreasing processing speed, 3 attention, 4 and memory. 5,6 These cognitive deficits can persist for months, even years in some cases. 7
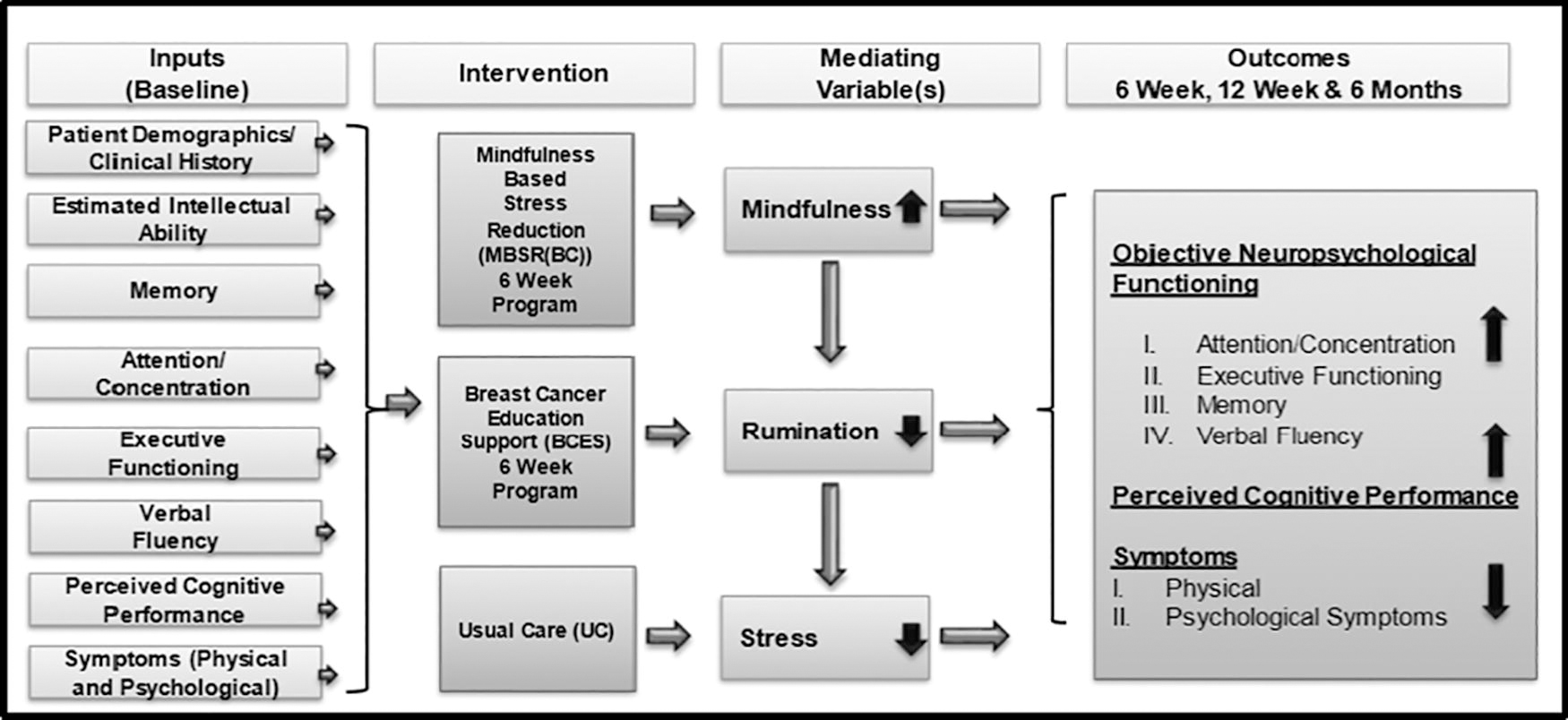
The biobehavioral logic model describes the inputs (symptoms and cognitive functioning) for MBSR(BC), BCES, and usual care regimens, mediators (mindfulness, rumination, and stress) and outcomes (objective and subjective cognitive functioning) and symptoms (physical and psychological). BCES, Breast Cancer Education Support; MBSR(BC), Mindfulness-Based Stress Reduction Program for breast cancer survivors.
Evidence for BCS post-CT suggests that MBSR significantly reduces feelings of stress, anxiety, and exhaustion, 8 and reduces fatigue and sleep disturbances. 12 Additionally, MBSR reduces biomarkers of inflammation, 13 salivary cortisol short-term, 14 improves sleep quality, 15 and reduces depression and fatigue in the short term. 16 As a cost-effective, practical, and safe intervention, MBSR is a recommended practice for BCS as part of the daily care routine. 17
Mediators are hypothesized intermediate intervening variables that are proposed to transfer the positive cognitive and stress-reducing effects of meditation as an independent variable onto the dependent variable, or outcome. 19 Testing the mechanisms is vital to identifying how and what changes are needed for the intervention to improve effectiveness, or if the intervention did not meet expectations, 9 and evaluating if the intervention needs modification to improve outcomes. 20 Measuring the proposed mechanism/mediator at multiple time points allows for establishing if a change in the mediator precedes a change in the outcome. 18
Our first hypothesized mediator is “mindfulness.” Two major cognitive processes (awareness and attention) occur in the “healing power” of mindfulness. 21 With an increase in mindfulness, individuals may experience emotions followed by a response or adaptation which may decrease symptoms. 22 Through observing and not making judgments, one can increase emotional acceptance 23,24 ; this allows for tolerating emotional experiences 25,26 and provides time to decrease reactivity and recovery from negative emotions. 27
Our second hypothesized mediator, “rumination,” is viewed as a measure of emotional regulation. 9 Rumination is defined as the tendency of neurotic, repetitive, primarily past thinking related to self-threats toward oneself. 28 Although rumination often results in a habitual mode of depression, mindfulness practice allows one to view rumination as a dysfunctional pattern, and through the practice of increased mindfulness concentration on the present moment, the spiral of negative fears and thoughts is inhibited. 9 Self-regulation of emotions and thoughts 29 reduces rumination and elaboration over the past and/or anticipated distressing experiences. 11,30
Limited research exists on specific mediators and mechanisms of action of MBSR programs on patient outcomes. Evidence reported in a systematic review and meta-analysis shows that MBSR significantly lowered anxiety, depression, fatigue, 31 decreased stress, and greater QoL associated with increased mindfulness as a mediator. 32 Changes in cognition can be due to mediators such as mindfulness, rumination, stress, self-compassion, nonreactivity, nonjudgment, emotional regulation, and much more. 33 A meta-analysis of mediators of over 20 mindfulness-based interventions among all types of patients, 34 showed strong consistent evidence for reduced emotional reactivity as a mediator, and moderately consistent evidence supporting mindfulness, rumination, and worry as mediators. Through improved emotional regulation and mindfulness, MBSR significantly reduced mood disturbances. 33 Through the mediation of altered attention, MBSR significantly altered perception of pain 35 and reduced subjective memory impairments among BCS, 36 thus supporting MBSR for memory difficulties associated with CI.
Our previous R21 grant hypothesized that the mechanism by which MBSR(BC) was effective occurred through reductions in fear of recurrence. 37 By increases in mindfulness practice and decreases in fear of recurrence, the MBSR(BC) may modulate the hypothalamic pituitary adrenal axis and sympathetic and parasympathetic nervous system responses resulting in reduced physical, psychological, and biological markers of stress, increased QoL, and cellular immune function. 37 In this R21 MBSR(BC) study, a reduction in fear of recurrence and improvement in physical functioning mediated the improvement in perceived stress and fatigue. 37 Mediating results in a larger R01 Symptom Cluster Trial, among BCS in the MBSR(BC) showed fear of recurrence and perceived stress, and not mindfulness, mediated reductions in anxiety and fatigue at 6 and 12 weeks. 10
This current study as the second aim of an R01 CA199160-01 cognitive clinical trial, examined the effects of the MSBR(BC) compared to the Breast Cancer Education Support (BCES) program or usual care (UC) in ameliorating CI among BCS who received CT or CT and radiation. The specific mediation aim was to “determine if improvements in objective neuropsychological functioning and perceived cognitive abilities achieved from the MBSR(BC) were mediated through increased mindfulness, decreased rumination, and decreased perceived stress.” Our biobehavioral logic model (Fig. 1) describes inputs (symptoms and cognitive functions), mediators (mindfulness, rumination, and stress), outcomes (objective and subjective cognitive functioning), and symptoms (physical and psychological).
Methods
Approvals
This trial protocol was approved by the institutional review board at the University of South Florida, which also serves as the ethics committee for the University of South Florida, AdventHealth in Tampa, FL, and Sarasota Memorial Hospital, Sarasota Florida, and Moffitt Cancer Center Scientific Review Committee.
Design
Using a three-armed randomized design, BCS were randomly assigned in a 1:1:1 ratio to either: (1) the 6-week MBSR(BC); (2) the 6-week BCES program; or (3) UC. The biobehavioral logic model is displayed in Figure 1 explaining mediators and outcomes. Those blinded to the intervention assignments were the principal investigator and assessors.
Study sample
Intervention procedures
Data collection
Data collection intervals included four assessment time points: (1) baseline; (2) 6 weeks after intervention completion; (3) 12 weeks; (4) and 26 weeks. Expectations for MBSR(BC), BCES, and UC were provided at orientation along with obtaining informed consent. Administration of objective neuropsychological assessments and subjective cognitive, stress, and mediator surveys, clinical history, and demographic data followed orientation, 6-week, 12-week, and 26-week postassessment. MBSR(BC) and BCES participants completed an additional survey (daily diary) one time per week during the 26 weeks of data collection.
Standard socioeconomic demographic data including age, gender, ethnicity, highest level of education completed, marital status, income status, and employment status were collected. Clinical history data were collected on the cancer site, date and type of diagnosis, treatment, lifestyle health behaviors, and medications.
Analysis plan
Analysis of covariance (ANCOVA) was initially used to examine the relationships between the MBSR(BC) intervention and potential mediators at 6 and 12 weeks (early effects) as well as 6 months (late effects). The ANCOVA models included adjustments for the baseline value of the mediator evaluated.
Mediation analyses were performed to evaluate mechanisms underlying positive effects achieved from the MBSR(BC) relative to the BCES program and UC regimen. The analyses involved two pairwise group comparisons: MBSR(BC) versus BCES and MBSR(BC) versus UC. The mediation analyses were conducted in MPlus version 8, 56 using methods described by Preacher, 1958. 57 Full information maximum likelihood estimation was used under the assumption of missingness at random and p-values were calculated based on a bootstrap distribution with 5,000 iterations. Full information maximum likelihood estimation is widely used to handle missing data; the advantages of this method include flexibility and the avoidance of ad hoc methods. 58
Direct, indirect, and total effects were calculated according to Hicks and Tingly, 2011. 59 With this method, estimates of the total effects of the intervention on outcome variables, and indirect effects attributed to a potential mediator, were estimated. Analyses were conducted for outcomes at 6 weeks, 12 weeks, and 6 months. For the outcomes at 6 weeks, change in the mediator variables from baseline to 6 weeks was used as the mediator. For the outcomes at 12 weeks and 6 months, change in the mediator variables from baseline to 6 and 12 weeks was used as the mediator, respectively. The sequential assumption common in mediation analysis 60 was not tested because the treatment was randomized. Statistical significance was evaluated at p < 0.05 (two-sided). Statistical analyses were performed according to the protocol. As specified in the Aim 1 paper, the study was powered to detect a clinically meaningful effect size (between groups) of (d) 0.50 or greater at 80% statistical power for the main effect of MBSR(BC) on the Stroop test. 61 All participants were included in the Aim 2 analysis.
Results
Analyses at each time point were based on all available repeated. The majority of the BCS, 73.1%, were white and non-Hispanic, with a mean age of 56.5. Seventy-eight percent of BCS underwent CT along with radiation, while 23% only had CT in their treatment regimen. There were statistically significant differences observed at baseline between the three groups in hours worked per week, in the medical history of hysterectomy or oophorectomy, and treatment with anthracycline CT. The Consolidated Standards of Reporting Trials (CONSORT) flowchart depicting recruitment and enrollment is provided in the Aim 1 article. 61
Subjective Cognition: Means and Standard Deviations by Treatment Group and Timepoint
Statistical significance was tested separately at 6, 12, and 26 weeks. a = MBSR group scored significantly different than BCES group at p < 0.05; b = MBSR group scored significantly different than Control at p < 0.05.
BCES, Breast Cancer Education Support; FACT, Functional Assessment of Cancer Therapy; MBSR, Mindfulness-Based Stress Reduction Program.
Objective Cognition: Means and Standard Deviations by Treatment Group and Timepoint
Statistical significance was tested separately at 6, 12, and 26 weeks controlling for baseline levels. a = MBSR group scored significantly different than BCES group at p < 0.05; b = MBSR group scored significantly different than Control at p < 0.05.
BVMT, Brief Visuospatial Memory Test; COWA, Controlled Oral Word Association; HVLT, Hopkins Verbal Learning Test; MBSR, Mindfulness-Based Stress Reduction Program; SD, standard deviation; WMS, Wechsler Memory Scale; WAIS, Wechsler Adult Intelligence Scale.
Symptom Responses: Means and Standard Deviations by Treatment Group and Timepoint
Statistical significance was tested separately at 6, 12, and 26 weeks controlling for baseline levels. a = MBSR group scored significantly different than BCES group at p < 0.05; b = MBSR group scored significantly different than Control at p < 0.05.
BCES, Breast Cancer Education Support; MBSR, Mindfulness-Based Stress Reduction Program; PROMIS, Patient-Reported Outcomes Measurement Information System; SD, standard deviation.
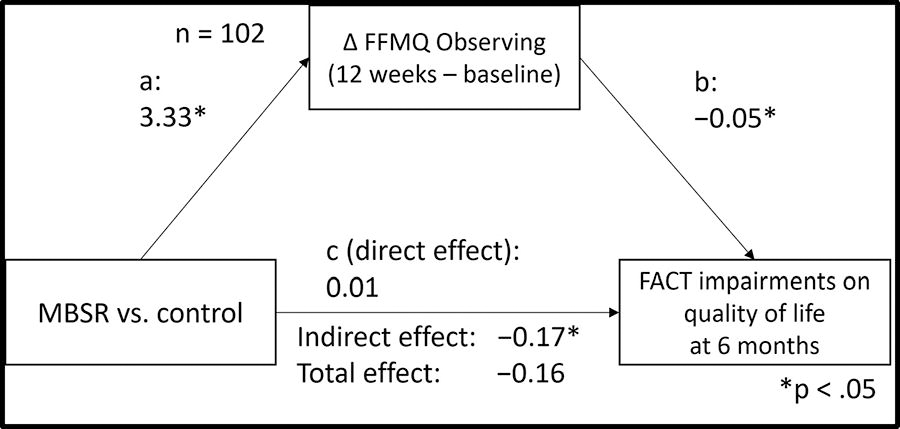
The role of FFMQ (observing) as a mediator for the effect of MBSR(BC) on FACT impairments on quality of life relative to UC at 6 months. FFMQ, Five Facet Mindfulness Questionnaire; MBSR(BC), Mindfulness-Based Stress Reduction Program for breast cancer survivors; FACT, Functional Assessment of Cancer Therapy; UC, usual care.

The role of FFMQ (observing) as a mediator for the effect of MBSR(BC) on logical memory relative to UC at 6 months. MBSR(BC), Mindfulness-Based Stress Reduction Program for breast cancer survivors; FFMQ, Five Facet Mindfulness Questionnaire; UC, usual care.
Relative to the UC group, the MBSR(BC) group showed more increase in the “observing” subscale from baseline to 12 weeks (a = 3.33, SE = 0.95, p < 0.01), which was in turn related to lower levels of “Impairments on QoL” at 6 months (b = −0.05, SE = 0.02, p = 0.02). This resulted in an indirect effect of (ind = −0.17, SE = 0.09, p = 0.04). However, the total effect was not significant (tot = −0.16, SE = 0.23, p = 0.48), indicating that participants in the MBSR(BC) group showed lower levels of “Impairments on QoL” at 6 months relative to the UC group only if they increased in “observing” from baseline to 12 weeks.
With the WMS logical memory score as the outcome, the MBSR(BC) group showed more increase than the UC group in the “Observing” subscale from baseline to 12 weeks (a = 3.36, SE = 0.96, p < 0.001), which was in turn related to higher levels of “logical memory” at 6 months (b = 0.19, SE = 0.07, p < 0.01). This resulted in an indirect effect of (ind = 0.64, SE = 0.29, p = 0.026). However, the total effect was not significant (tot = −1.00, SE = 0.66, p = 0.134), indicating that participants in the MBSR(BC) group showed higher levels of logical memory at 6 months relative to the UC group only if they increased in “Observing” from baseline to 12 weeks. No significant indirect effects were found for other outcomes and mediators at 6 weeks, 12 weeks, and 6 months and when comparing the MBSR(BC) group with the BCES group.
Discussion
The goal of this mediation research was to provide new knowledge and evidence identifying potential mechanisms of action for the MBSR(BC) intervention among BCS who completed CT or CT and radiation treatment. After initial analyses of early (baseline to 6 and 12 weeks, respectively) and late (baseline to 6 months) intervention effects of MBSR(BC) relative to the BCES program or a UC regimen, results pointed to increases in observing as part of mindfulness as a potential mediator of MBSR(BC) effects on impairments on QoL and logical memory at 6 months relative to UC. The MBSR(BC) group did not differ from UC in terms of impairments on QoL at 6 months; however, the mediation effects indicated that the MBSR(BC) was associated with an increase in observing from baseline to 12 weeks relative to UC, which was in turn associated with lower levels of impairments on QoL at 6 months. Unexpectedly, the MBSR(BC) group scored lower on a test of logical memory relative to UC at 6 months. However, the mediation effect indicated that the MBSR(BC) was associated with an increase in observing from baseline to 12 weeks relative to UC, which was in turn associated with higher levels of logical memory at 6 months. Rumination, perceived stress, and subconcepts of mindfulness other than observing were not identified as mediators. No mediation mechanisms were identified for outcomes at 6 and 12 weeks. Also, no mediation mechanisms were identified for differences between the MBSR(BC) and the BCES program. Potential bias was a consideration in this study. Randomization, corrected for selection bias and performance bias related to prior use of techniques similar to MBSR was assessed at baseline. Results showed all three groups were similar in their experience. Detection bias was corrected by randomization that minimized differences in characteristics. Additionally, attrition bias was corrected by including all data from four time points in the analyses, even if not complete.
The improvements in objective neuropsychological functioning, such as logical memory, and perceived cognitive abilities in the MBSR(BC) group are consistent with current literature on increased mindfulness as a mediator. 9 Increased mindfulness is achieved through awareness and attention, or the observation of one’s internal and external world, this was emphasized in the MBSR(BC).
The reduction of “impairments on QoL” was indirectly affected, or mediated, by mindfulness. Participants only showed a reduction in Impairments in QoL relative to UC if they showed an increase in “Observing” from baseline. Similarly, participants only showed an increased logical memory after 6 months if they showed an increase in mindfulness “Observing” from baseline.
The MBSR(BC) group showed reduced perceived stress at 12 weeks relative to BCES. Lower rumination, higher describing, observing, and awareness were observed in the MBSR(BC) group relative to UC, but only observing as a part of mindfulness was determined to have an indirect mediation effect upon outcomes of impairments of QoL. Previous findings indicate the reduction in pain may be related to an altered perception of pain, 35 and the reduction in fatigue may be related to increased mindfulness 31 ; however, we were unable to find a mediator related to the reduction of pain. The mediating relationships through the mechanisms of “observing” as related to mindfulness have only been tested among BCS and may be generalizable to the understanding and further knowledge development of the mediation effects of MBSR(BC) on other types of cancer survivors or among individuals with chronic health conditions.
Related to our hypotheses, only two mediating relationships were identified related to cognitive functioning—both were through increases in mindfulness through the mechanism, of “observing” a subconcept of mindfulness when comparing the MBSR(BC) with UC at 6 months. Related to our model, although our results did not find rumination and stress as having a mediating relationship, the results showed that the MBSR(BC) group had lower rumination, higher describing, observing, and awareness relative to UC, with only “observing” as a subconcept of mindfulness showed an indirect mediation effect upon outcomes of “Impairments of QoL.” By testing the mechanisms of the program, this study also contributes to the improvement and advancement of nonpharmacological treatment for cancer survivors showing that it may “optimize” the clinical therapeutic treatment effects of MBSR on multiple distressing symptoms. It was also interesting that mediation effects were found at 26 weeks, but not earlier. This may indicate that a sufficient number of time points is needed to determine the shape and temporal sequencing of change.
Data Sharing Statement
Data will be made available to faculty researchers at universities in the United States through a data sharing agreement and to approved members of the scientific community 3 years after the final grant completion date. This dissemination plan will undergo yearly review. Pending results, effective intervention materials, and programs will be shared through a website or national repository.
Footnotes
Authors’ Contributions
C.A.L. initiated the development of the program research objectives, designed the programs, and applied for funding as the principal investigator in the study. G.H., K.E.K., R.R.R., and H.M. were responsible for the methodology and data curation. M.S.M. and E.B. contributed to the delivery of the mindfulness intervention, while C.C.S.R. contributed to the delivery of the BCS educational program. K.A.D. was the site principal investigator for Moffitt Cancer Center. T.F. was the site coordinator for Sarasota Memorial Health Care System and J.M.L. was the site principal investigator for Sarasota Memorial Health Care System. C.C. and J.K. assisted with identifying patients for study recruitment. C.A.L. was the creator of the protocol article with contributions from R.R.R. and J.Y.P. All authors including, J.R.W., S.M., A.J., S.T., S.N., M.K., L.S.P., R.C., D.P., and E.H. contributed to multiple revisions of the article and approved the final edited version to be published.
Author Disclosure Statement
No competing financial interests exist.
Funding Statement
This work is funded by the National Cancer Institute Grant Number NCT02786797. Award Number 1 R01 CA199160-01 from the National Cancer Institute supported the project described. This research contained within this publication was supported in part by the Survey Methods Core Facility at the H. Lee Moffitt Cancer Center & Research Institute. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health. This trial protocol was approved by the institutional review board at the University of South Florida, which also serves as the ethics committee for the University of South Florida, AdventHealth in Tampa, FL, Sarasota Memorial Hospital, Sarasota Florida, and Moffitt Cancer Center Scientific Review Committee to ensure the ethical treatment of participants.