
Abstract
Objective:
To identify behavior change techniques (BCTs) and the mode of delivery used in yoga interventions across five neurological conditions.
Methods:
This scoping review followed Arksey and O’Malley’s methodological framework for conducting scoping reviews. Medline, CINAHL, EMBASE, PsycINFO, and CENTRAL databases were searched, combining key terms for population and intervention. Covidence software was used for study selection. Template for Intervention Description and Replication checklist was used to report the intervention and study quality was assessed using the Physiotherapy Evidence Database (PEDro) scale. Interventions were coded for BCTs using various taxonomies and delivery approaches were classified using Mode of Delivery Taxonomy Version 0.
Result:
Among 4805 articles screened, 35 met the inclusion criteria. Parkinson’s disease, multiple sclerosis, and stroke were the most prevalent disability types with fewer studies on spinal cord injury and traumatic brain injury. A total of 134 BCTs were identified, 20 out of the 93 BCTs (25%) were from the BCT v1 taxonomy, while 15 additional BCTs were identified from other taxonomies and some BCTs were defined by the authors based on the need for yoga interventions. The most used BCTs included 12.6 body changes (68.57%, n = 24), 4.1 instruction (57.14%, n = 20), 12.5 adding objects (48.57%, n = 17), 1.2 problem solving (37.14%, n = 13), 6.1 demonstration (34.28%, n = 12), 8.1 behavioral practice and rehearsal (31.42%, n = 11), and 8.7 graded tasks (28.57%, n = 10). The most common delivery approach was face-to-face. The median PEDro score was 6 indicating medium study quality.
Conclusion:
Clear reporting of the intervention description and use of BCTs may enhance understanding and ability to replicate yoga interventions. This helps to adapt yoga by changing behaviors using specific BCTs to meet the goals and principles of yoga depending on the target population. The review may help inform future research to examine the effectiveness of specific BCTs on desired outcomes.
Introduction
Globally, neurological conditions are among the leading causes of disability-adjusted life years and the second leading cause of death. These chronic conditions affect individuals across all age groups and are often accompanied by comorbidities, requiring comprehensive and equitable health care solutions. 1 Living with a disability entails continuous adaptation as individuals navigate both the functional challenges of their condition and societal perceptions. 2 These experiences highlight the multifaceted nature of living with neurological conditions. Notably, behavioral factors account for approximately 66.3% of disability-adjusted life years in these conditions, emphasizing the need for effective interventions to address both functional and behavioral dimensions. 1,3 In line with the Global, Regional, and National Burden of Neurological Disorders report, our review focuses on five prevalent neurological conditions such as stroke, parkinson’s disease (PD), multiple sclerosis (MS), spinal cord injury (SCI), and traumatic brain injury (TBI)—that significantly impact mobility, independence, and overall quality of life. By narrowing the scope to these conditions, we aim to provide a focused analysis of yoga interventions, offering valuable insights for clinicians and researchers working with individuals having similar challenges. 1,4 –6
Mind–body interventions, such as yoga, are widely used to improve health in various neurological conditions 7,8 and are reported as the most preferred practice adopted by people with neuro disabilities. 9 –12 Yoga has been defined as a mind–body practice composed of physical postures, breathing, and meditation. 13 However, yoga represents a broad discipline with various types of practice emphasizing different aspects of the mind–body connection. Also, different practitioners use different sets of training and philosophies within each yoga type. 14,15 This diversity carries over to yoga interventions in the literature, making the concept of yoga difficult to understand. The studies often include a combination of components such as postures, meditation, and relaxation which are core elements of Hatha yoga practices. 16 However, the specific details, such as the content and structure of the intervention are often not documented. 17 This makes it challenging to replicate yoga interventions and identify their active ingredients. Most published reviews on yoga in neurological conditions have highlighted a lack of high-quality studies. 8,17,18 Moreover, people with neurological conditions require personalized approaches to implement yoga that consider their abilities and contraindications; therefore, the standard practice of yoga must be adapted to enhance accessibility.
Michie et al. developed a taxonomy named behavior change techniques version 1 (BCTv1) that has been widely used to identify the characteristics of interventions. 19 Incorporating behavior change techniques (BCTs) into an intervention has shown improved clarity and comprehensiveness in describing the intervention. 20 BCTs are defined as an observable, replicable, and irreducible component of an intervention designed to alter or redirect causal processes which regulate behavior. The BCTv1 taxonomy consists of 93 distinct BCTs hierarchically organized into 16 groupings that provide more coherent and standardized labels, definitions, and shared language for reporting complex interventions. 19
Even if yoga interventions were developed without theory or BCT perspectives, they inherently include strategies that aim to change behaviors and their outcomes. 21 In this review, BCTs provide a framework for analyzing yoga interventions. For instance, strategies such as goal setting (e.g., setting goals for practice frequency), feedback (e.g., providing real-time corrections on poses), prompts and cues (e.g., visual or auditory reminders to practice), social support (e.g., group classes or practice partners), and mental rehearsal (e.g., visualization of poses or relaxation) are frequently embedded within yoga interventions. These BCTs can enhance participant engagement, foster adherence, and optimize outcomes in yoga research. Identifying and applying BCTs in yoga interventions allows a more systematic understanding of their mechanisms and effectiveness. This approach enables researchers to move beyond stating that “yoga or the intervention was provided” and instead articulate the techniques used and their potential impact on outcomes. Thus, clear reporting of “what the intervention included and how it was developed and delivered” is essential. Furthermore, intervention reporting should be explicit and use common terminology to facilitate accurate replication of intervention content. 22 To understand the content and formation of yoga interventions in research, we have used various BCT taxonomies to retrospectively characterize the content of identified yoga interventions.
Methods
The structure of the scoping review followed the methodological framework outlined by Arksey and O’Malley. 23 We have followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist, and the protocol is registered on the open science framework (osf.io/3sz9b). The PRISMA-ScR highlights key elements such as defining the scope of the review, systematically charting the data, and presenting results in a structured manner to enhance clarity and reproducibility.
Stage 1: Identify the research question
Primary objectives: (1) To identify the BCTs used in yoga interventions across five neurological conditions: stroke, PD, MS, SCI, and TBI. Identification of BCTs will be according to BCTv1 and other relevant taxonomies such as Coventry, Aberdeen, and London–Refined taxonomy, which provides context for understanding BCTs related to health and well-being, enhancing the precision of their identification in this review. (2) To identify the mode of delivery of yoga interventions using Mode of Delivery Taxonomy Version 0 (MoDTv0). Secondary objectives: (3) To summarize the effectiveness of identified BCTs used in yoga interventions on physical, psychological, and psychosocial outcomes in people with neurological conditions. (4) To identify research gaps and suggestions for future research.
Stage 2: Identify relevant studies
Search strategy
Systematic searches were conducted using Medline, EMBASE, PsycINFO, CINAHL, and CENTRAL. The search strategy for Medline was used as a reference to identify related terms in other databases. For example, population-related terms included “cerebrovascular disorder*,” “cerebrovascular disease*,” “cerebrovascular accident*,” “stroke,” or “cerebral infarction*,” while intervention-related terms included “yoga*,” “mind-body*,” or “mindfulness.” The complete search strategies for all other databases have been included in the supplementary materials for reference. We also added the broader term “mindfulness” in our search, as some authors equate it to yoga. The search was conducted as per the guidelines for constructing a search strategy 24 in consultation with an experienced subject librarian. It was completed in February 2022 and revised in November 2023. Keywords (e.g., yoga physical therapy) from published yoga studies were also considered to ensure the inclusion of relevant articles. Only English language publications were used; no other limits for study design, year of publication, or study setting were applied to broaden our search. As published yoga often focuses on postures and meditation, interventions that included both were the principal focus of this review. Reference lists from identified articles, ResearchGate, and other journals not indexed on PubMed or Ovid were also searched.
Stage 3: Study selection
Eligibility criteria: Population, intervention, comparison, outcome, and study design are provided in Table 1. After conducting the searches, articles were imported into the Covidence software, which includes a two-stage screening process to assess the relevance of identified articles. Authors independently screened titles and abstracts of retrieved articles to determine eligibility. During the screening process, some articles labeled as “yoga” in the title described interventions like mindfulness-based stress reduction, which sometimes made it unclear whether the intervention was actually yoga. To ensure no relevant studies were overlooked, we carefully reviewed each article to verify that only those specifically involving yoga interventions were included in the final analysis. This corresponds with the iterative nature of scoping reviews. 23 Articles that satisfied first-stage screening were retained for second-stage screening where authors independently screened full-text articles. Upon completion of the screening process after each stage, any discrepancies were resolved via discussion with senior authors.
Eligibility Criteria
MS, multiple sclerosis; PD, Parkinson’s disease; SCI, spinal cord injury; TBI, traumatic brain injury.
Stage 4: Data charting
This scoping review used the Template for Intervention Description and Replication (TIDieR) checklist, which provided a framework for describing the intervention, and other pertinent information (e.g., materials used, the person delivering the intervention, fidelity of delivery, and scope for tailoring). 25 Study design, sociodemographic information of the sample, outcome measures, type of yoga, and type of control or intervention group were extracted. When possible, effect size and p-value (95% confidence interval) were extracted and if effect sizes were not provided, they were calculated. We also calculated PEDro scores to assess the quality of the included studies. The PEDro scale consists of 10 criteria that evaluate methodological quality, including randomization, blinding, and statistical analysis. A score of ≥6 indicates good quality, with higher scores reflecting stronger rigor. Scores below 6 suggest potential design or reporting limitations. 26
Coding for BCTs
BCTv1 was the primary taxonomy used to identify BCTs. 19 However, during the coding process, we identified that some techniques were not fully captured by BCTv1. Considering the broad area of behavior change and the shortcomings identified in using BCTv1, 27 and to ensure a more comprehensive approach, we also referred to other behavior change taxonomies developed by Michie et al. 21,28,29 Additionally, we expanded our search for additional BCTs by exploring the literature (searching studies and existing research for relevant BCTs), theoretical constructs that explain how behavior change happens (e.g., self-determination theory), and routes to behavior change classification that utilize three key elements—motivation, action planning, and prompts/cues that drive and sustain behavior change. 30 Finally, when BCTs related to published yoga descriptions were not found through the approaches we used, or when there were gaps in the current yoga interventions, we defined and included additional techniques in our article. This broader approach allowed us to capture a wider range of BCTs essential for understanding and identifying BCTs in yoga interventions.
Authors H.P. and A.D. completed the BCT online training on www.bct-taxonomy.com. Both reviewers, H.P. and A.D., adhered to all coding assumptions listed in BCTv1. When a disagreement arose, the FAQ section on the BCT website was consulted and discussed to code the BCTs in the given intervention. H.P. and A.D. coded and compared the initial 10% of articles and discussed any discrepancies with senior authors W.B.M. and K.L.B. All the articles were then coded independently by H.P. and A.D. BCTs were identified based on the information provided in the articles and then BCTs were coded using the text present in the intervention descriptions of included articles. Additional Supplementary Data S1 and references provided by the authors were considered in case of missing intervention descriptions.
To summarize the effectiveness of yoga for physical, psychological, and psychosocial outcomes, effect sizes were extracted when possible. Given the small sample sizes, Hedge’s g was used as an effect size measure as it provided a better estimate of the variance. 31 Alternatively, if effect size was not reported, Hedge’s g effect sizes were calculated (using comprehensive meta-analysis software) when enough data were presented. Corresponding authors were contacted via email to get missing data or additional information needed to calculate the effect sizes. Effect sizes were computed by entering means and standard deviations for the yoga and control groups. If this information was not available, we used alternative, comparable methods available in the software (e.g., mean change scores, confidence interval and Cohen’s d, difference in means and standard error). If we could not calculate the effect size because of a lack of data availability or when articles reported median values, we extracted the p-values to estimate the effectiveness of yoga. Intention to treat data was used when available and only for articles with complete intervention data, Hedge’s g was calculated based on the number of participants whose post-treatment data were available (and not the enrolled participants).
Stage 5: Collating, summarizing, and reporting the results
BCTs were identified and narratively synthesized to describe the intervention. The BCTs and mode of delivery formed the results of this scoping review. We used the NVivo software 2018 version to code the BCTs. Intercoder agreement between the two coders was calculated in NVivo which allows us to correctly identify the important words that highlight a given BCT and to support the validity of our coding. We calculated the kappa statistics for the agreement between the coders.
Results
Selection process
The search strategy returned 4805 articles from Medline, EMBASE, CINHAL, PsycINFO, and CENTRAL databases. After the removal of duplicates, 3915 articles remained. First-stage screening eliminated 3796 articles, leaving 119 articles. Second-stage screening resulted in 41 studies being left. Out of the 41 studies, six articles were secondary articles, using the same intervention as previous articles, 32 –37 thus leaving a total of 35 articles included in this review (Fig. 1).
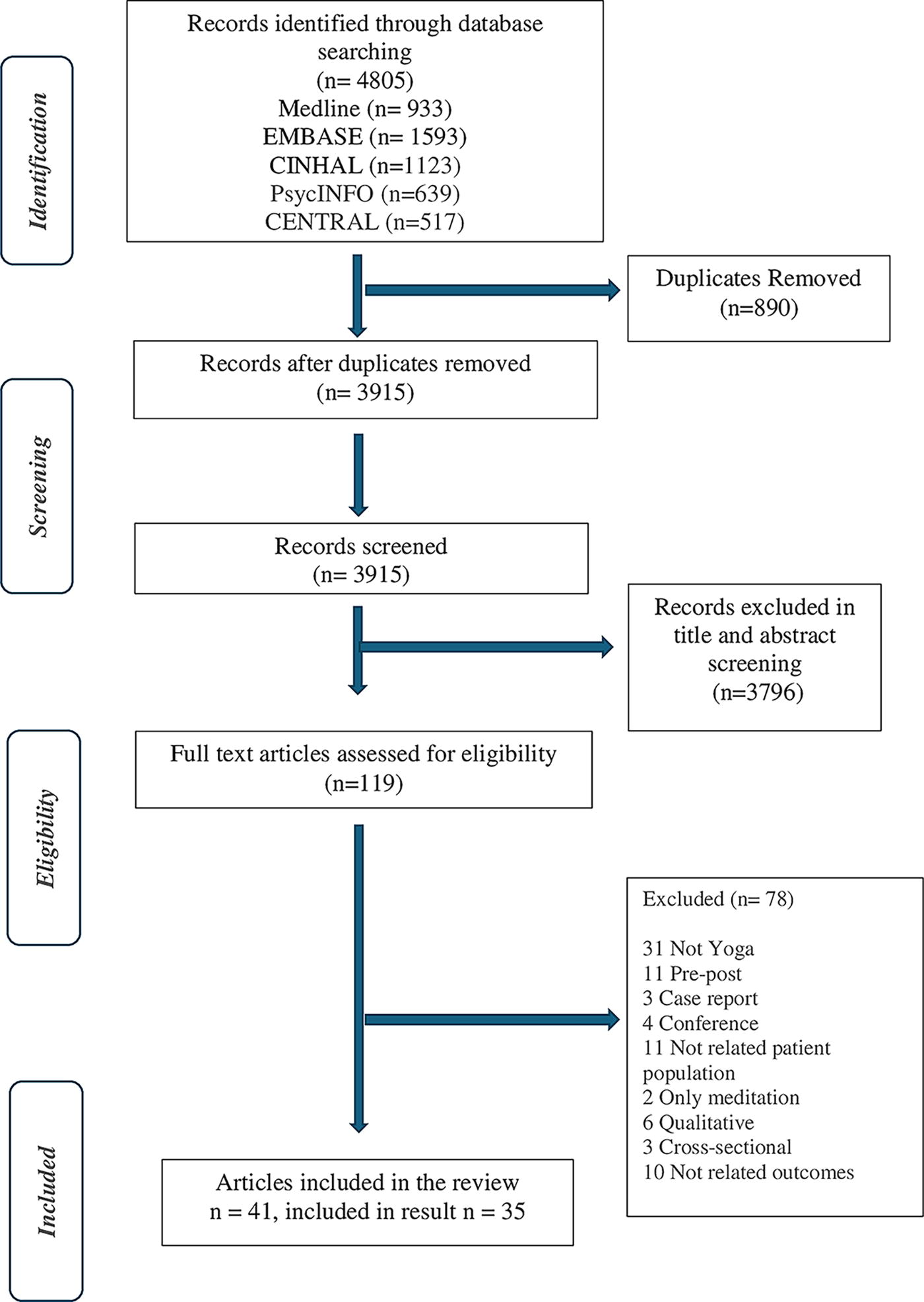
Outlines the PRISMA flowchart. PRISMA, preferred reporting items for systematic reviews and meta-analyses.
Study characteristics
Among the 35 articles, MS
38
–52
was the most commonly studied population with 15 articles, followed by PD
53
–62
with 10 articles, and stroke
63
–68
with 6 articles. Traumatic conditions such as SCI
69,70
and TBI
71,72
were the least identified commonly studied neurological conditions and consisted of two articles each. From a geographical standpoint, studies were conducted in the United States (n = 13),
38,50,53
–55,57,59
–63,71,72
followed by Iran (n = 6),
40,43
–45,48,52
South Australia (n = 3),
49,64,65
India (n = 2),
58,70
China (n = 3),
47,66,67
Canada (n = 1),
69
Ireland (n = 1),
41
Hongkong (n = 1),
56
UK (n = 1),
46
Slovenia (n = 1),
39
Russia (n = 1),
51
Taiwan (n = 1),
37
and Brazil (n = 1).
42
Hatha yoga was the most commonly reported type of yoga (n = 13),
39,40,43
–48,50,52,55,56,60
followed by Iyengar (n = 5),
38,51,53,62,69
Hatha and Vinyasa combined (n = 2),
57,61
Hatha and Satyananda combined (n = 2),
64,65
Therapeutic yoga (n = 2),
63,67
Chair yoga (n = 1),
49
Gentle yoga (n = 1),
71
Kaivalya yoga (n = 1),
42
and Power Vinyasa yoga (n = 1).
54
Seven studies did not report the type of yoga.
41,58,59,66,68,70,72
Out of 35 articles, 2 articles were completely home-based programs (HBP),
45,58
while 5 articles incorporated HBP in addition to delivery in a facility.
38,43,53,56,63
Intervention duration was not mentioned in the two articles.
39,55
Only one article reported on fidelity measures, using audio recordings.
56
Three articles reported retention measures at 3
41,56
and 6 months
61
(Table 2—study characteristics, Supplementary Data S1
Study Characteristics
AG, active group; CG, control group; EDSS pyr, expanded disability status score–pyramidal; EDSS, expanded disability status score; FI: fitness-instructor; GNDS, Guy’s Neurological Disability Scale; H&Y, Hoehn and Yahr; M2M, movement to music; PPMS, primary progressive multiple sclerosis; PRMS, primary relapsing-remitting multiple sclerosis; PT, physiotherapy; RRMS, relapsing-remitting multiple sclerosis; SIQR, semi-interquartile range; SPMS, secondary progressive multiple sclerosis; TBI, traumatic brain injury; WLC, waitlist control; YG, yoga group.
Objective 1: BCTs extraction using BCT taxonomies
A total of 134 BCTs were identified using only the BCTv1 taxonomy. Given that most articles had waitlist control groups, BCTs could not be coded separately for the control and intervention groups. 73 Thus, only the yoga group was coded for BCTs. Twenty out of 93 BCTs (21%) in BCTv1 were coded. The intercoder agreement between the two coders was excellent (kappa >0.75). For one article, 61 the intervention description was obtained from a separate article that was hand-selected from the reference list. 74 For another study, a protocol was cited that reported details about the yoga intervention, but it was not retrievable. Instead, the intervention description available in the main article was used. 38 The theory coding scheme 75 was not explored in this review as only one article 56 among the included articles mentioned the use of theory.
The most commonly used BCTs included 12.6 body changes (e.g., altering body structure) (68.57%, n = 24); 4.1 instruction on how to perform a behavior (e.g., how to do yoga) (57.14%, n = 20); 12.5 adding objects to the environment (e.g., adding props) (48.57%, n = 17); 1.2 problem solving (e.g., providing strategies to solve a problem) (37.14%, n = 13); 6.1 demonstration of the behavior (e.g., showing how to perform) (34.28%, n = 12); 8.1 behavioral practice and rehearsal (e.g., practicing/rehearsing yoga repeatedly) (31.42%, n = 11); and 8.7 graded tasks (e.g., progression of postures) (28.57%, n = 10). At least one BCT was identified in 10 out of the 16 possible BCT constructs listed in BCTv1, although no BCTs were identified in 2; feedback and monitoring, 6; Comparison of behaviors; 9 comparison of outcomes; 10 reward and threat; 14 scheduled consequences; and 16 covert learning hierarchies. Table 3 shows the most common BCTs from BCTv1.
Most Common Identified Behavior Change Techniques Using Behavior Change Techniques Version 1
BCTs, behavior change techniques.
Additionally identified BCTs
In total, we defined three additional BCTs named “positive emotions,” “providing knowledge of intervention principles,” and “conscious awareness of body.” The currently available BCTv1 taxonomy mentioned that it may add “positive emotion” as a BCT in future literature. 19 We also identified interventions where the BCT “positive emotions” could have been coded. “Positive emotions” are defined as an approach to “advise on ways to mentally recall good/pleasant memories to facilitate mood.” “Providing knowledge of intervention principles” is defined as “providing information on the rationale behind the intervention and how it can help with the underlying symptoms/impairments within the defined population.” “Conscious awareness of body” is defined as “identifying the state of each body part with regulated breathing and allowing the mind to work in harmony without thinking of external objects.” Furthermore, Dixon et al. defined motivational techniques as “techniques that change the conscious desire to do the target behavior by making beliefs or feelings about the behavior more favorable and less favorable towards the unwanted behavior.” 30 This definition was used to code articles that used motivational strategies. Table 4 provides all the identified BCTs.
Identified Behavior Change Techniques Using Behavior Change Techniques Version 1 and Additional Behavior Change Techniques
Objective 2: Mode of yoga intervention delivery
The MoDTv0 provides a classification system for behavior change interventions, organized into a four-level structure with 65 unique modes under 15 upper-level classes and various sublevels. We used this system to identify the delivery methods used in yoga interventions. As per the MoDTv0 taxonomy, 35 articles used a “face-to-face” mode of delivery, while two articles used an online-based mode. 49,52 Both of these modes are classified under sublevel 2 of the upper-level “Informational Mode of Delivery” category. 76 This upper-level category represents broader modes of intervention delivery, with sublevels such as “Human Interactional Mode” (real-time interaction), which is further divided into “Face-to-Face” and “At a Distance” (e.g., online-based). This classification helped us to identify how yoga interventions are delivered, which can guide future designs, expand reach, and improve accessibility.
Objective 3: Identified BCTs and effects on outcomes (Supplementary Data S2)
Only four out of the 35 articles reported effect size (Cohen’s d). 55,59 and only two articles reported Hedge’s g. 50,54 Our analysis showed that articles that used some or all commonly identified BCTs in this study resulted in small to medium effects in physical/motor outcomes such as Unified Parkinson’s disease rating scale I and II, 53,55,61,62 range of motion (ROM) and muscle length, strength in upper and lower extremities, 34,53 and balance (MiniBESTest). 55 In addition, there is a medium to large effect seen in balance (Berg balance and MiniBESTest) and mobility (10 min U and M walk test). 34,54 However, they did not lead to much effect in psychosocial outcomes such as depression, 33,61,64 anxiety, 64 and quality of life. 34,38,61 –63
When less commonly identified BCTs such as habit formation, framing/reframing, and reduce negative emotions were used in combination with any of the commonly identified BCTs, greater improvements in depression, anxiety, memory, and social support were noted. 65 Similarly, the use of the BCT framing/reframing in addition to any common BCTs showed medium effect sizes, particularly for anxiety, depression, perceived hardship, perceived equanimity, and disease-specific health-related quality of life. 56 The BCT prompts/cues in addition to any common BCTs showed a medium effect on balance (Tinetti balance assessment) and kinesthesia outcomes. 59
Articles with no identified BCTs had either no statistically significant 39 or small difference in their respective outcomes. 66 –68 One study showed improvements (p < 0.05) in the modified Barthel index, which measures the level of assistance a person requires with daily activities and offers valuable insight into their functional independence. However, whether these improvements are statistically significant is unclear as no further data are provided. 66 In addition, their PEDro scores are very low. 39,66 –68 Additionally, the use of other BCTs such as monitoring devices (heart rate monitor) showed a medium effect size in 6MWT but did not improve sit-to-stand and PROMIS-fatigue and pain outcomes. 46 The use of BCT “Information about social and emotional consequences” led to medium effects on Acceptance and Action Questionnaire (improved psychological flexibility) and small to medium effect on depression, and self-compassion. 69 However, the study PEDro score is very low.
Objective 4: Gaps in yoga research for people with neurological conditions
Despite the growing interest in yoga as an intervention for individuals with neurological conditions, several gaps remain in the research. One such gap is the limited use of theoretical frameworks to guide the development of yoga interventions. Only one article used the theoretical context (self-transcendence) to develop the yoga intervention. 56 Additionally, two articles did not report the duration of yoga 39,55 and only one article mentioned the type of sampling used. 56 Moreover, one study failed to mention the intensity and frequency of the intervention. 67 In most articles, yoga interventions were adapted for the study intervention by either a yoga instructor, a neurologist, or both or from a literature review. One article did not specify who developed the intervention. 44 These gaps highlight the need for more comprehensive and standardized reporting in future research. The studies included in this review generally had smaller sample sizes. No major adverse events related to yoga were reported. The common reasons for higher attrition rates were transportation issues, time constraints, personal or family health concerns, and weather-related factors. 35,38,59,61 Last, the quality of studies as per the PEDro score was fair to good quality, with a median score of 6.
Discussion
This review highlights the potential of incorporating BCTs into yoga interventions to enhance their content and delivery for individuals with neurological conditions. Due to the complex nature of yoga, identifying BCTs provides valuable insights into intervention components, helping to determine which techniques work best for specific outcomes. The use of BCTs can promote a clearer understanding of how interventions work or fail and when modifications are necessary to optimize their impact. 29 While the complexity of BCTs can make it challenging to measure their impact, particularly when used in combination, they also present challenges, such as difficulties in standardizing interventions across diverse populations, variations in implementation, and potential misalignment with individual needs. Despite these challenges, BCTs promote consistency, transparency, and replicability in interventions. By supporting the use of BCTs in yoga, we do not intend to alter the core principles, philosophies, or implications of yoga but to provide a framework for delivering effective interventions. Our goal is not to impose rigid BCTs across all interventions but to emphasize the importance of selecting appropriate BCTs that align with the specific needs of the population and the desired outcomes.
Included articles have developed yoga interventions by focusing more on the physical aspects. This includes BCTs such as “body changes” by altering body structure, “instruction” on how to do yoga, and “adding objects to the environment” in terms of adding yoga props. This could explain the medium to large effects seen in physical outcomes. Similarly, articles that have used BCTs such as “framing/reframing” and “reduce negative emotions” showed greater changes in mental health outcomes but only small effects on physical outcomes. 56 When creating interventions, it is crucial to address physical, psychological, and social aspects to ensure positive impacts on these areas of well-being.
In terms of physical outcomes, there was increased ROM and strength in the hip and ankle, which may have led to improvements in mobility. 34,53,54 Furthermore, rigidity was reported to have improved. Only two studies reported on SCI and TBI, which makes the effectiveness of BCTs on yoga in this population uncertain. Within the stroke population, although clinical improvement was noted in outcomes such as anxiety and depression, there was limited improvement overall. 64,65
For the five different neurological populations reported, each condition has a different pathophysiology and may require tailored interventions. For example, yoga interventions for SCI and TBI need trauma-sensitive themes. Consideration of the stage of the disease is also important, especially for PD (e.g., trunk involvement, medication side effects) and MS as the protocol may depend on the participant’s abilities. Having said that, adapting yoga as per the defined population may prevent future studies from just following the general/preexisting format in yoga research. We anticipate that our defined BCTs in this review could be helpful in future studies, allowing for the provision of yoga knowledge specific to a defined population, and facilitating better behaviors and outcomes.
BCTs derived from theoretical constructs, such as goal setting, self-monitoring, action planning, and feedback on behavior, displayed greater transformations in promoting behavior change. 77,78 Such constructs often initiate motivation and are increasingly considered integral to motivation change. 79 Despite the many benefits that implementation of these BCTs has, none of these BCTs were identified in the included articles. Goal setting is recognized as a crucial construct to enhance physical activity across populations. 80 Incorporating goal setting in the intervention design allows the patient to be actively involved in framing their goals. 81 The construct “feedback” is also highly used in various BCTs. It has been rationalized as a vital strategy not only in behavior change theories, leading to operant conditioning, 82 but also as a major focus of motor learning theory used in neurorehabilitation. 83 Action planning prepares the participants by discussing when, where, and how to act with an intended goal. 84
Self-regulation, an important concept in behavior change 78 is any effort to actively control behavior. It involves the processes of self-monitoring, self-evaluation, and self-reinforcement by inhibiting dominant and automatic behaviors that conflict with long-term goals. 85,86 The use of self-monitoring techniques has been found to have a positive effect on physical activity behavior in adults, 87 people with disabilities 88 and in self-management for people with SCI. 89 Yoga philosophies have roots in self-regulation principles; however, none of the included articles used self-regulation techniques. Another major component of self-regulation involves building self-efficacy. BCTs encompass self-efficacy elements such as verbal persuasion about capability and self-talk. However, these specific techniques were also not identified in the included articles.
Intervention delivery is another important consideration when designing interventions. If skill improvement is a desired intervention goal, it may be necessary to utilize a more collaborative approach, such as use of “structured role play” in the intervention delivery. Currently, all interventions are delivered by health care professionals or yoga instructors; however, peer-delivered interventions have shown wide acceptance in people with neurotrauma. 90 Thus, a peer-led credible source, which is considered a construct of BCTs, may act as a precursor to developing effective interventions.
Some of the articles included in this study contain superficial and general descriptions which made identifying BCTs challenging and limited our coding ability. For example, most interventions reported implementing modifications or tailoring without further reasoning. However, since modifying or tailoring are not considered distinct techniques, 29 we did not code them. If an intervention explicitly mentioned modifying or tailoring exercises to enhance a given task (e.g., posture) and provided justification, was coded as problem solving. Most studies implicitly described the delivery of the intervention in a group setting but provided no further detail or reasoning behind the group formation. It would have been useful to know whether the group intervention was framed to provide social support, to involve more people with similar needs, etc. Because this information was not specified, we were unable to code them under the BCT social support. Finally, interventions reported meditation and breathing but no explicit information was provided, restricting our ability to code BCTs.
Interventions reported in certain studies used similar terminology, but with varied interpretations, leading to inconsistent coding of BCTs. For example, two studies. 53,64 briefly reported the use of visualization techniques. Without detailed descriptions, it was challenging to determine the specific BCT involved. It may qualify for three different BCTs, that is, mental rehearsal of successful performance, imaginary punishment, or imaginary rewards. Moreover, one study 59 depicted visualization techniques using two distinct principles, action observation and motor imagery. However, no details were provided to identify the related BCTs. This lack of clarity may explain why some articles had medium effects on physical outcomes 59 when using mental rehearsal along with other BCTs, while some articles had small effects on psychosocial outcomes. 64,65
Two studies 45,56 mentioned supervision as a part of the intervention; however, they lacked details about using feedback or prompts/cues while supervising. This made it challenging to determine whether it was feedback on behavior or simply supervision without feedback. Furthermore, various studies, mentioned earlier, included home-based yoga programs; however, only one study explicitly addressed incorporating yoga practice into regular lifestyle practice. 65 As a result, only generalization of target behavior was coded for the former, while habit formation and generalization of target behavior were coded for the latter. Graded task was identified in 11 studies 45,46,53 –58,63,64,74 ; however, its implementation varied. For example, one article 58 increased the number of repetitions but not the difficulty of the postures. Other articles adopted a progressive increase in the level of difficulty over one 54 or multiple classes. 53,57,63 One study reported the intervention followed a standardized progression, but the definition of this standardization was unclear. 55
Through combining the concepts of yoga philosophies and behavioral theories we defined three new BCTs relevant and useful to yoga interventions. It is important to properly explain and distinguish these BCTs from the current BCTv1 taxonomy so that they can be utilized effectively. “Positive emotions” are distinct from mental rehearsal of successful performance and reduce negative emotions as they focus on identifying pleasant emotions and memories rather than imagining successfully completing the behavior. Recognizing the importance of positive emotions is a helpful component in achieving set goals. While goal-setting strategies focus on the process of setting a goal, the emotions involved during that process play a vital role in successfully reaching the set goal, as emotional barriers can impede the progress. Therefore, it is essential to consider the emotional well-being of individuals, as mental health disorders are common after neurological disabilities. 91 Furthermore, like other BCTs in BCTv1, “positive emotions” could be split into identifying positive emotions as behavior, or positive emotions as outcome. However, we could not code positive emotions as an outcome, as articles do not have appropriate outcomes. “Providing knowledge of intervention principles” is different from BCTs such as information about health consequences and information about emotional consequences as it rather provides rationale behind the intervention (how specific type of yoga could help them), and how it directly benefits the participant, while the informational BCTs pertain more toward explaining the consequences of the general target behavior or outcome. Finally, “Conscious awareness of body” is distinct from body changes as it is not simply relaxation training. It focuses more on the kinesthetic awareness of the relevant body parts with their regulated breathing. This BCT aims to embody the basic principles of yoga and allow the mind and body to work in harmony.
A study by Young et al. 46 used external safety heart rate monitors during the intervention. This was consistent with the BCT defined by Knittle et al. 79 and therefore we coded it under “use of external monitors.” Additionally, we used the MAP classification for behavior change to explore techniques that can be used in yoga interventions. It is based on the dual processing model, explaining two major routes of action for most BCTs: the reflective and associative pathways. 92 The reflective pathway contains techniques that influence motivation and transform motivation into action, such as those described by the interactions between constructs in social cognitive theories. The associative pathway integrates prompts or cues to influence a behavior. Dixon et al. further elaborated upon this model, proposing three elements—motivation (reflective, preintentional), action regulation (reflective postintentional), and prompts and cues (associative). 30 When designing interventions such as yoga that require a behavior change, it is important to consider elements of both reflective and associative pathways.
In terms of gaps in the yoga research, we found a lack of effect size measures reported in the articles. Including effect sizes would facilitate better comparison of results across studies. Additionally, the small sample sizes in the studies we reviewed limit the generalizability of our findings, a challenge also observed in mindfulness studies. 18,93 As yoga research is still evolving, larger multicenter RCTs are needed to strengthen the evidence and improve the generalizability of future results. We also observed potential risks, such as one article included postures such as headstands for MS patients, which could lead to a possible risk of injury. 44 Furthermore, mindfulness is a broad term with varied subtypes, so providing the underlying principle used in mindfulness interventions can facilitate the understanding of this term. We found that there was a lack of consistency in the literature when mentioning the type of yoga used. Some studies 41,44,47,48,51,66,68 used the term “yoga exercise”; however, yoga and exercise are two different interventions with different effects. Only one article reported their yoga protocol guided by a theory of self-transcendence 56 ; however, it is theory-guided rather than theory-applied intervention. 94
Limitations
While broad terms were used in our search, we did not search gray literature sources and only included English language publications. This may have created a language bias and narrowed our scope of the literature. Some of the identified BCTs throughout this literature may be inaccurately assumed or may not correspond to the intention of the original authors, which is also a limitation of BCT coding. Last, research is very heterogeneous, which does not lend itself to systematic reviews or meta-analyses.
Conclusion
Our review highlights the importance of identifying and incorporating BCTs into yoga interventions for individuals with neurological conditions. By providing recommendations for the effective integration of BCTs, we aim to improve intervention outcomes. A key challenge in current yoga interventions is the lack of detailed descriptions regarding their type, delivery mode, and program structure. Identifying BCTs can address these gaps by offering a framework for designing more effective and consistent interventions. We recommend providing clearer intervention details to facilitate understanding, enhance replication, and improve the overall study of yoga’s impact.
Footnotes
Acknowledgment
The authors would like to acknowledge and thank their subject librarian Charlotte Beck for guiding them in searching and refining the search strategies.
Authors’ Contributions
Conceptualization: H.P., K.L.B., W.B.M., and W.C.M. developed the initial research idea and the overall research goals. Methodology: H.P., K.L.B., W.B.M., and W.C.M. designed the methodology used in the study. Software: H.P. and A.D. handled and updated the documents on the software (Covidence and Open Science Framework) needed for the research. Validation: H.P., K.L.B., and A.D. verified the results through data checks. A.D. helped H.P. in the screening of the articles and identifying BCTs. Formal analysis: H.P. applied statistical methods to analyze the study data. Investigation: H.P. did the investigation. Resources: H.P. and W.C.M. provided the necessary materials, equipment, and other resources for the study. Data curation: H.P., K.L.B., A.D., W.B.M., and W.C.M. managed and maintained the research data, ensuring its integrity and accessibility. Writing—original draft: H.P. prepared the initial draft of the article. Writing—review and editing: W.C.M., K.L.B., and W.B.M. critically reviewed and revised the article for important intellectual content. Visualization: H.P. created the figures and visual elements of the article. Supervision: W.C.M., K.L.B., and W.B.M. provided oversight and mentorship throughout the research project. Project administration: W.C.M., K.L.B., W.B.M., and H.P. coordinated the project activities and managed the overall execution of the research plan.
Author Disclosure Statement
The authors report there are no competing interests to declare.
Funding Information
This study received no funding.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.