
Abstract
Objectives:
To detect differences between individualized homeopathic medicinal products (IHMPs) and placebo after 4 months of intervention in patients with chronic low-back pain (LBP).
Design:
Four-month, double-blind, randomized (1:1), placebo-controlled, two parallel arms trial.
Setting:
PG3 and research outpatient department of D. N. De Homoeopathic Medical College & Hospital.
Subjects:
Sixty participants with chronic LBP.
Interventions:
Verum (n = 30; IHMPs plus concomitant care) versus control (n = 30; placebos plus concomitant care).
Outcome Measures:
Primary—Oswestry LBP Disability Questionnaire (ODQ); Secondary—Roland Morris Pain and Disability Questionnaire (RMPDQ); McGill Pain Questionnaire—Short Form (SF-MPQ); measured at baseline, and every month, up to 4 months.
Results:
Group differences achieved significance or near significance in all the specified outcomes—ODQ score (F 1, 58 = 4.331, p = 0.042), RMPDQ score (F 1, 58 = 2.939, p = 0.092), and SF-MPQ total score (F 1, 58 = 6.666, p = 0.012). Rhus toxicodendron (n = 13), Bryonia alba (n = 8), Hypericum perforatum, and Nux vomica (n = 5 each) were the most frequently prescribed medicines. Different repertories were used as per the need of the cases—Kent, Synthesis, Murphy, Pulford, Boericke, Boger Boenninghausen’s Characteristics and Repertory, and Complete. Minor adverse events were reported from either group.
Conclusions:
Thus, homeopathic medicines worked significantly better than placebos in reducing chronic LBP. Independent replications are warranted to substantiate the findings.
Clinical Trial Registration Number:
CTRI/2022/04/041878.
Introduction
A common musculoskeletal condition, low-back pain (LBP) is typically felt between the lower rib cage and the buttocks, with occasional limb pain. In addition to numbness or tingling, weakness in some muscles and a dull or acute sensation akin to an electric shock are common descriptions of leg pain. Based on the cause, LBP is classified into five categories: facet joint, sacroiliac, discogenic, radicular, and spinal stenosis pain. 1 Because a spinal nerve root is frequently involved, people with LBP may feel spine-related leg pain, also known as sciatica or radicular pain. When a nerve is damaged or squeezed far from the spinal column, some patients may have radicular symptoms without lower back pain. It can be acute (a short time, <6 weeks), subacute (a little longer, 6–12 weeks), chronic (a long time, >12 weeks), or specific and nonspecific (90%) in nature. When the pain is caused by a certain disease or structural problem in the spine or when the pain radiates from another part of the body, it is called specific, and when it isn’t possible to identify a particular disease or structural reason to explain the pain, it is called nonspecific. 2 Globally, LBP is the leading cause of disability and the second most common reason for primary care visits, with an annual prevalence of 15%–45%. In 2020, LBP affected 619 million people globally, and it is estimated that the number of cases will increase to 843 million cases by 2050, driven largely by population expansion and aging. 3
In India, the pooled point, annual, and lifetime prevalence of LBP were 48% (95% confidence interval [CI] 40%–56%), 51% (95% CI 45%–58%), and 66% (95% CI 56%–75%), respectively. 4 LBP is a condition that can affect anyone at any age; most people experience it at least once in their lives. 5 The highest number of cases of LBP occurs in the 50–55 age range. 6 LBP is more common in women. 7 It is a significant public health concern that can negatively impact a patient’s quality of life and mental health. 8 LBP can affect a person’s quality of life and mental well-being and is frequently linked to reduced productivity at work and a huge economic burden on individuals and societies. There is evidence from a small number of studies that 90% of patients with acute LBP recover in 4 weeks, while symptoms may persist for 6 weeks. Other research reports that 80% of LBP bouts end in 2 weeks and 90% do so in 6 weeks. 7
Samuel Hahnemann developed the idea of homeopathy, which is predicated on the idea of “similitude” and backed by inductive reasoning as follows: a drug can treat an illness if it causes similar symptoms in healthy individuals. He attempted to treat several illnesses with potentized dilutions of the corresponding elicitors following the theory of “similia similibus curentur” (let likes be treated by likes). Hahnemann prepared medications during his experiments using a wide range of natural ingredients. He noticed that infinite dilutions of these compounds when applied step-by-step and coupled with forceful shaking “succussion” (collectively, potentization) at every dilution step produced a potent action in these solutions. Clinicians such as Dewey, Morrison, and Lilienthal compiled treatments corresponding to symptoms of LBP. Hartmann also provided a list that included Arnica montana, Rhus toxicodendron, and Antimonium tartaricum. 9 –12 Despite the debates and complaints around the lack of results that have been scientifically verified and the notion that homeopathy is predicated on unproven theories that are rarely supported by high-quality scientific data, homeopathy is nevertheless used today. 13
Several homeopathy studies of different designs exist on LBP: double-blind, placebo-controlled, one randomized trial with individualized homeopathic medicinal products (IHMPs), 14,15 three randomized trials with complex homeopathic remedies among which two were safety trials and one with multicentric design, 15 –17 one single-arm study, 18 and one triple-arm randomized trial using injections as well. 19 Different outcome measures and follow-up periods were chosen in different studies, and a mixed response was reported. However, in the scarcity of convincing evidence supporting the efficacy of IHMPs in the treatment of chronic LBP, and as randomized controlled trials (RCTs) are the gold standard for efficacy trials, 20 this trial evaluated the efficacy of IHMPs in randomized and double-blinded design using validated outcome measures.
Materials and Methods
Objectives
Primary objectives include comparing the Oswestry LBP Disability Questionnaire (ODQ) scores of individuals with chronic LBP who received IHMPs versus a placebo after 4 months of treatment. Secondary objectives include looking for variations between the McGill Pain Questionnaire—Short Form (SF-MPQ) and the Roland Morris Pain and Disability Questionnaire (RMPDQ).
Trial design
D.N. De Homoeopathic Medical College & Hospital’s PG3 and research outpatient departments carried out the double-blind, randomized, placebo-controlled, two-parallel arms trial.
Ethics approval
The Institutional Ethics Committee approved the study protocol (reference number DHC/Eth-45/2018/748/2021; dated October 26, 2021). The Clinical Trials Registry—India received a prospective registration of the trial protocol (trial registration number CTRI/2022/04/041878). Key trial protocol components are available online at https://ctri.nic.in/Clinicaltrials/pmaindet2.php?EncHid=NjgwOTM=&Enc=&userName=CTRI/2022/04/041878 (Supplementary Data S1). The protocol complied with the Good Clinical Practice guidelines and the Declaration of Helsinki. 21 Before enrolment, all patients received a patient information leaflet in the regional vernacular, Bengali, and all participants gave their signed informed permission.
Participants
Participants must have been between the ages of 18 and 65 years, have had a diagnosis of chronic LBP for longer than 3 months (International Classification of Diseases, Tenth Revision, Clinical Modification code M54.5), had mild-to-moderate degenerative changes shown on radiological examinations, and be literate in Bengali, Hindi, or English to be eligible for participation. Patients who refused to give their consent; those with severe degenerative changes; those with abnormalities of the spine; those who had had prior spinal surgery; those with uncontrolled chronic illnesses; those with mental incapacity; patients with compromised immune systems; patients who used drugs; those who were pregnant, reached puberty, or were nursing; and those who were concurrently involved in other clinical trials were all excluded.
Interventions
The subjects were randomized to receive either control (identical-looking placebos + concurrent care) or verum (IHMPs plus concomitant care). Both the initial and follow-up visits were in person. Depending on the unique demands of the patients and situations, IHMPs were prescribed in centesimal potencies (30cH, 200cH, and 1000cH) and customized dosages, one to four doses, once to twice a day as needed. Each participant had a 4-month follow-up period. Infrastructure constraints prevented the arrangement of coded LM (50 millesimal) potencies. The homeopaths could change the prescribed homeopathic medicine or dosing instructions at subsequent visits as per individualized requirements. Weekly phone calls and follow-up visits ensured that recommendations were followed. Every unique prescription was accompanied by repertorization when needed, utilizing the software RADAR (Rapid Aid to Drug Aimed Research [RADAR®], version 10.0.028 [ck], Archibel 2009, Belgium), reviewing Materia medica, and reaching an agreement with three homeopaths. Following the traditional homeopathic principles, medications, potencies, and dosages were changed as needed in subsequent sessions. One of the homeopaths was a master’s degree holder in homeopathy and had taught classical homeopathy for over 20 years. The remaining homeopaths were members of the institution’s postgraduate training program. Every homeopath participating was connected to the state council that applied to them. All three prescribers saw the patients together. Each of them identified their recommended treatment independently and then compared with each other. After mutually agreeing, the final prescriptions were made. In case of any discrepancy, inputs were considered from other senior homeopaths of the institution.
Each dose was made up of 40 cane sugar globules (no. 40), soaked with one drop of the prescribed medication (kept in 90% v/v ethanol), and was to be taken orally on an empty stomach with a clean tongue. The dosage and frequency of administration were determined by the needs of each case individually. Along with coded medicines (or placebos), the participants were given known (uncoded) placebos until the next planned visit. In addition to being instructed to suck the globules rather than swallow them, patients were also instructed not to handle the globules or to consume any food, liquids, smoke, or brush their teeth for 30 min after taking them. Furthermore, during the trial, the participants were instructed not to consume coffee, mints, or any other food or drink that included medication.
A pharmaceutical accountability log was maintained, recording the dosages administered, globules returned, and compliance with the care recommendations provided. There was no observed variation in compliance across the groups about adhering to the indicated treatment regimens and concomitant care measures. Similar to the verum, placebos were administered to the control group. Four nonmedicated cane sugar globules (no. 40) moistened with rectified spirit constituted the placebo. Standardized management guidelines for yoga, spinal extensor exercises, fomentations, lumbar bracing, and ergonomic adjustments were given to all enrolled patients; regardless of the codes, they were allocated. Four months was the length of the therapy.
The source of all the medications was Dr. Willmar Schwabe India Pvt., Ltd., a company certified by Good Manufacturing Practices in New Delhi, India.
Outcome measures
Primary—ODQ: The ODQ was first developed in 1980 and has been clinically validated as an assessment tool. The most recent version was published in Spine in 2000. It measures therapeutic benefits with a maximum score of 50 (10 sections, 5 points each), and it is easy to administer and score. Every question has a score of 0 for the first statement and a score of 5 for the last statement. The scoring method involves applying the formula 100 × (total scored)/(total potential score). The minimal clinically significant difference (MCID) is 12.8 percentage points, 22 and the minimal detectable change is 10 percentage points. The ODQ is a useful tool for assessing and tracking the effects of interventions on patients’ illnesses. It is administered at baseline and four months during therapy. 23,24
Secondary: RMPDQ: The RMPDQ, initially introduced in 1983, is a 24-item self-report questionnaire about how low-back pain affects functional activities. Each question was worth one point, so scores could range from 0 (no disability) to 24 (severe disability).
25
The questionnaire is short, simple, sensitive, and reliable. It is scored by adding up the number of items the patient has ticked. Greater levels of disability are reflected by higher scores. SF-MPQ: Developed in 1987, the SF-MPQ is a reliable tool for assessing chronic pain in adults. It comprises 15 items—the first 11 sensory and the last 4 affective. All the items are rated on an intensity scale of 0: none, 1: mild, 2: moderate, and 3: severe. The SF-MPQ also includes one item for present pain intensity (0–5) and one item that is a 10 cm visual analog scale (VAS) for average pain. The total pain rating index (PRI) score is obtained by summing the item scores (range 0–45) and converting it into a percentage score by the formula: 100 × (total score)/(total possible score). There are no established critical cut points; a higher score indicates worse pain. A mean improvement in total scores of more than 5 on the 0–45 scale demonstrates a clinically important change.
26,27
Timeline
For a maximum of four months, each outcome was assessed at monthly intervals. The rationale behind choosing a 4-month treatment period was an inconclusive finding of an earlier trial that lasted for 3 months, and further extension of follow-up was recommended. 14
Sample size
The MCID of ODQ in patients with LBP was reported as 12.8. In an earlier study by Prakash et al., in 2022, 14 the mean (± standard deviation [SD]) of ODQ was reported as 31.9 (±12.9) and 33.4 (±11.9) in the verum and control groups, respectively, after 3 months of intervention in patients with lumbar spondylosis. Thus, the target mean in the verum group was set as (33.4–12.8) = 20.6. Accounting for an expected attrition rate of up to 15%, and detecting the target difference of 12.8 between two independent means of ODQ scores after 4 months of intervention through unpaired t test and 1:1 allocation, a study with 2 × 30 patients yielded 97.5% power based on a two-sided significance level of 5%.
Randomization
Participants were randomized equally (1:1) to the verum and control groups to minimize selection bias. An impartial third party used StatTrek centrally to create a list of 60 random numbers by limiting 6 permuted blocks of fixed size 10 while preserving a 1:1 distribution among groups. Participants were thus randomized evenly between the control and verum groups. The block randomization approach can provide a uniform distribution of the important parameters related to the result and homogenize the data by removing variables that are not necessary. To dispense medications, the blinded pharmacist was given this random number chart. A different, independent third party classified identical glass vials with an amber color as “1” or “2,” denoting either identical placebos or medications. The random number chart assigned the vials to each participant in a consecutive manner. After the trial ended and the dataset was frozen, the codes were cracked. Crossover was prohibited since a participant’s code was fixed at the beginning of the 3-month intervention and could not be changed.
Blinding
Throughout the experiment, everyone involved—participants, treating physicians, pharmacists, outcome assessors, and data entry operators—remained blinded. By asking the participants which group they thought they were in, the blinding was verified both before and after the study. After the final prescription was decided, the case files were shared only with the research assistants. The blinded pharmacist’s responsibility was to retain allocated codes using the random number table while distributing the prescribed drugs from the vials with codes. The medications were written down, sealed in an opaque packet, and given to the pharmacist rather than being revealed to the participants.
Allocation concealment
Screening, enrolment, and serial number assignment to participants were carried out by blinded postgraduate trainees and registration counter workers. The blinded homeopaths interviewed the blinded individuals afterward to determine the prescription. By keeping the treating physicians and trial recruiters unaware of the random number sequence, allocation concealment was accomplished.
Statistical methods
The intention-to-treat strategy was used in the statistical analysis, meaning that all included patients were included in the final analyses. Regression means from a linear regression model were imputed to determine missing values. Shapiro–Wilk tests, Q-Q plots, and histograms were used to analyze the data distribution; no discernible deviation from normalcy was found. The mean and 95% CIs from descriptive statistics were used to display the intragroup changes. The basic descriptive statistics, both continuous and categorical, were presented using various metrics, such as mean, percentages, absolute values, and SDs. Continuous data are displayed as median (IQR) and mean ± SD. Two-way repeated measure analysis of variance (ANOVA) was used to examine group differences while accounting for time–effect interactions. Furthermore, the mean estimates derived individually for each month were compared using unpaired t tests. The reason for this is that ANOVA reduces inflated Type I errors brought on by multiple testing better than t tests do. Cohen’s d (little effect, 0.01–0.059; moderate effect, 0.06–0.137; and large impact, >0.138) and partial eta-squared (great effect, 0.8; medium effect, 0.5; and little influence, 0.2) were used to report the effect sizes. A statistically significant result was defined as a two-tailed p-value of less than 0.05. The data were analyzed using the Statistical Package for Social Sciences (version 23.0; IBM Corp., IBM SPSS Statistics for Windows, Armonk, NY, USA).
Adverse events
The investigators instructed the patients to record treatment-emergent adverse events, serious adverse events (SAE), 28 unexpected adverse events, adverse drug reactions, and suspected adverse reactions during the experiment. They were also instructed to report over the phone or in person any unpleasant aggravations (medical, homeopathic, or disease symptoms). Some (uncoded) IHMPs were used as “rescue remedies,” apparently unrelated to the trial, to treat acute diseases. These were “short-acting” remedies selected based on the “acute totality” of the patients; thus, it was unlikely that they would affect the trial-specific medicinal effects, 8,29 even though the additional homeopathic treatment might have confused the trial-specific medications. The patients were treated by the same clinicians who prescribed their study therapy. The patient would stay in their primary allocated group (either placebo or verum), but the prescribed medication could change. After the acute phases of the sickness subsided, the treating physicians gave the patients another assessment. Depending on the patient’s symptomatology and what the doctors thought was appropriate for the patient’s circumstances, either the same trial medicine with the same code was given again or new medications were given.
Trial reporting
The Consolidated Statement for Reporting Trials 30 and Reporting Data on Homeopathic Treatment 31 were followed in the reporting of this trial (Supplementary Data S1 and S3).
Results
Participant flow
According to the previously mentioned inclusion and exclusion criteria, 92 patients suffering from chronic LBP were screened, 32 were excluded due to various reasons (listed in Fig. 1); 60 met the eligibility criteria and they were enrolled into either placebo (n = 30) or verum (n = 30) groups. During the 4-month follow-up, some of the participants discontinued; 2 cases in the IHMPs group and 3 cases in the placebo group; the reasons for withdrawal were long distance and availing other treatment options. All the 60 randomized participants were included in the final analysis (Fig. 1).
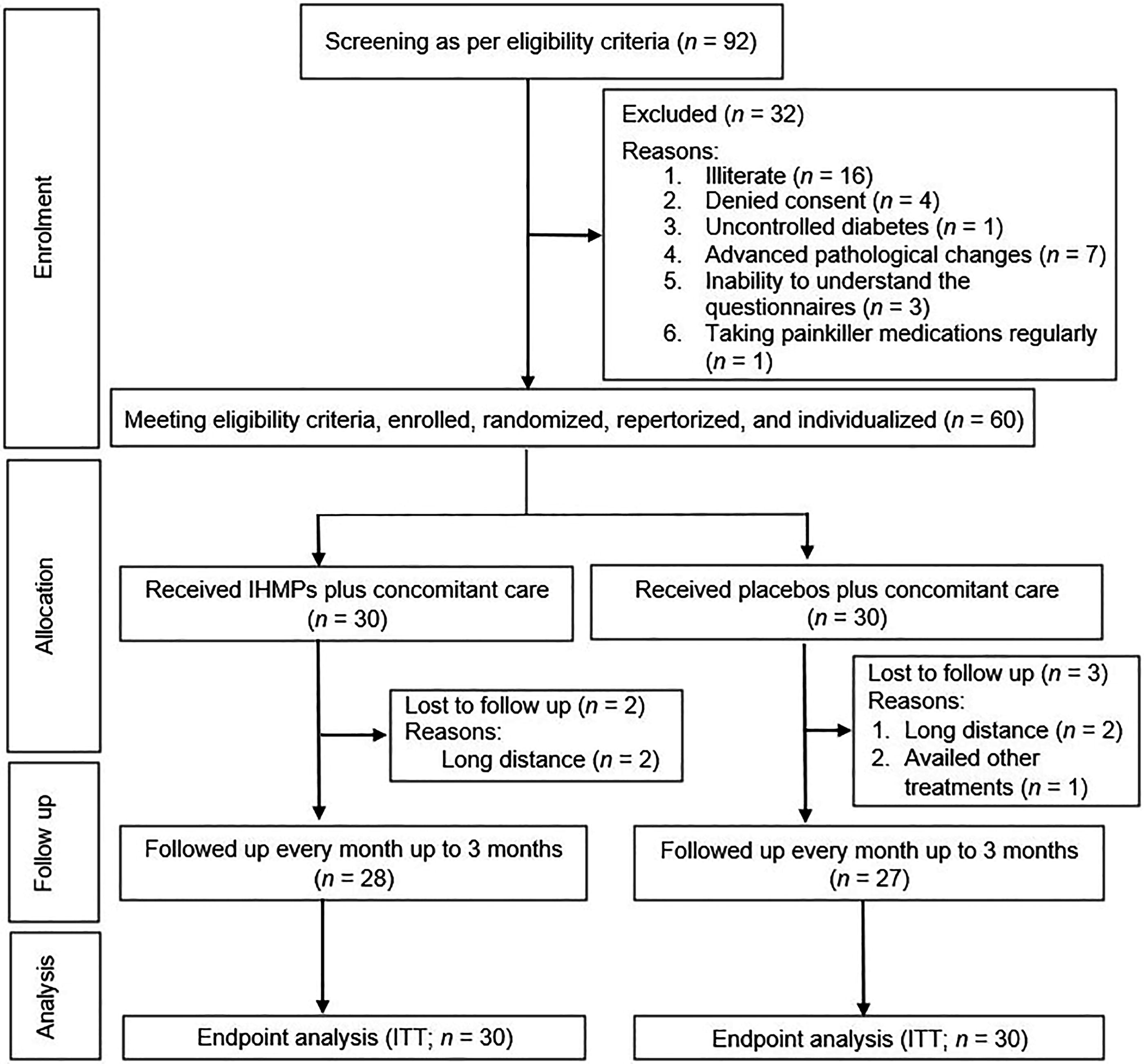
CONSORT study flow diagram.
Recruitment
This study had an 18-month recruitment phase from April 18, 2022, to October 18, 2022, followed by a 4-month intervention and follow-up phase. Follow-up of the last enrolled patient was completed by February 21, 2023.
Baseline data
The distribution of the 12 baseline confounders has been presented using descriptive statistics as follows: age, body mass index, blood pressure, duration of suffering, sex, comorbidities, residence, diagnosis, treatment availed, employment, education, and socioeconomic status (Table 1).
Comparison of the Sociodemographic Characteristics Between Groups at Baseline (n = 60)
Continuous data presented as mean ± standard deviation.
Categorical data presented as absolute values (percentages).
IHMPs, individualized homeopathic medicinal products.
Numbers analyzed
All randomized 60 participants were subjected to the final analysis.
Outcomes
The between-group difference in ODQ total score was statistically significant (ANOVA: F 1, 58 = 4.331, p = 0.042, partial η 2 = 0.089; t test: mean difference −7.8, 95% CI −10.8 to −4.9, p < 0.001, d = 1.368). The ODQ total scores of both groups improved in a clinically significant magnitude (verum: 20.9 vs. placebo: 9.0). The magnitude of the difference in improvement between the two groups was statistically significant (−7.8, 95% CI −10.8 to −4.9), not significant clinically (MCID 12.8) Table 2.
The between-group differences in RMPDQ total scores were statistically nonsignificant overall using two-way repeated measure ANOVA (F 1, 58 = 2.939, p = 0.092, partial η 2 = 0.048) although significant after 4 months using an unpaired t test (mean difference −1.2, 95% CI −2.0 to −0.5, p = 0.001, d = 0.893) Table 3.
In terms of the SF-MPQ, the between-group difference in SF-MPQ total score was statistically significant (ANOVA: F 1, 58 = 6.666, p = 0.012, partial η 2 = 0.103; t test: mean difference −1.9, 95% CI −3.1 to −0.8, p = 0.001, d = 0.870). Between-group mean differences in the PRI% sensory dimension score revealed significance (F 1, 58 = 4.244, p = 0.044, partial η 2 = 0.068; t test: mean difference −1.8, 95% CI −2.8 to −0.7, p = 0.001, d = 0.903); however, the difference in PRI% affective dimension score was nonsignificant (F 1, 58 = 1.016, p = 0.318, partial η 2 = 0.017; t test: mean difference −0.1, 95% CI −0.3 to 0.1, p = 0.450, d = 0.263) Table 4.
Comparison of the Oswestry Low-Back Pain Disability Questionnaire Total Score Between Groups at Baseline and at Different Time Points (n = 60)
aUnpaired t tests; t 58, t score at 58 degrees of freedom; p a, intergroup differences detected by unpaired t tests; p b, intergroup differences detected by two-way repeated measure ANOVA models.
*p < 0.05, **p < 0.01; ***p < 0.001.
ANOVA, analysis of variance; CI, confidence interval; IHMPs, individualized homeopathic medicinal products; ODQ, Oswestry Low Back Pain Disability Questionnaire; SD, standard deviation; SEM, standard error of mean.
Comparison of the Roland Morris Pain and Disability Questionnaire Total Score Between Groups at Baseline and at Different Time Points (n = 60)
aUnpaired t tests; t 58, t score at 58 degrees of freedom; p a, intergroup differences detected by unpaired t tests; p b, intergroup differences detected by two-way repeated measure ANOVA models.
*p < 0.05, **p < 0.01.
ANOVA, analysis of variance; CI, confidence interval; IHMPs, individualized homeopathic medicinal products; RMPDQ, Roland Morris Pain and Disability Questionnaire; SD, standard deviation; SEM, standard error of mean.
Comparison of the McGill Pain Questionnaire—Short Form at Baseline and at Different Time Points (n = 60)
aUnpaired t tests; t 58, t score at 58 degrees of freedom; P a, intergroup differences detected by unpaired t tests; P b, intergroup differences detected by two-way repeated measure ANOVA models.
*p < 0.05, **p < 0.01.
ANOVA, analysis of variance; CI, confidence interval; IHMPs, individualized homeopathic medicinal products; SF-MPQ, McGill Pain Questionnaire—Short Form; SD, standard deviation; SEM, standard error of mean.
Medicines used
Twenty-one different medicines were prescribed at baseline—Rhus toxicodendron (n = 13), Bryonia alba (n = 8), Hypericum perforatum, and Nux vomica (n = 5 each) being the most frequently prescribed remedies (Table 5; Supplementary Data S4). Three potencies were used as follows: 30cH (n = 11, 18.3%), 200cH (n = 46, 76.7%), and 1000cH (n = 3, 5%) (Table 6).
Prescribed Medicines in the Two Groups at Baseline (n = 60)
Chi-squared or Fisher’s exact tests applied; p < 0.05 two-tailed considered as statistically significant.
IHMPs, individualized homeopathic medicinal products.
Prescribed Potencies in the Two Groups at Baseline (n = 60)
Chi-squared or Fisher’s exact tests applied; p < 0.05 two-tailed considered as statistically significant.
IHMPs, individualized homeopathic medicinal products.
Repertories used
Different repertories were used for the selection of the remedies as per the need of the cases—Kent (n = 16), Synthesis (n = 8), Murphy, Pulford, and Boericke (n = 2 each), Boger Boenninghausen’s Characteristics and Repertory (BBCR) (n = 11), and Complete (n = 14) (Table 7). Various homeopathic repertorization methods were used as follows: Kent’s 2nd, 3rd, and 4th methods, Boger’s method, Boericke’s method, and thumb–finger method (Table 8).
Used Repertories in the Two Groups at Baseline (n = 60)
Chi-squared or Fisher’s exact tests applied; p < 0.05 two-tailed considered as statistically significant.
IHMPs, individualized homeopathic medicinal products; BBCR: Boger Boenninghausen’s Characteristics and Repertory.
Repertorization Methods Used in the Two Groups at Baseline (n = 60)
Chi-squared or Fisher’s exact tests applied; p < 0.05 two-tailed considered as statistically significant.
IHMPs, individualized homeopathic medicinal products.
Adverse events
Throughout the study, only two adverse events were reported as follows: one case of diarrhea in the verum and one case of COVID-19 vaccine-induced pain in the control group. The former was prescribed Aloe socotrina 30cH, 4 doses a day for 2 days, and the latter with Ledum palustre 30cH, 4 doses, twice a day.
Discussion
In this double-blind randomized placebo-controlled trial, 60 participants with chronic LBP were treated for 4 months. Primary outcomes (ODQ) and secondary outcomes (RMPDQ and SF-MPQ) were measured at baseline and every month for up to 4 months. The IHMPs group displayed statistically significant improvements compared with the placebo group. Group differences achieved significance or near significance in all the specified outcomes; however, the group differences were statistically significant, but clinically not. Within-group changes were both statistically and clinically significant in both groups, indicating the presence of substantial placebo effects. Rhus toxicodendron, B. alba, H. perforatum, and Nux vomica were the most frequently prescribed medicines. Different repertories and repertorization methods were used as per the needs of the cases. No harm or SAEs were reported from either of the groups. Rigorous and larger trials are warranted to arrive at any recommendations conclusively.
The study’s main strengths encompassed a robust design involving randomization, double-blinding, allocation concealment, and multiple and repeatedly measured outcomes for rigorous analysis. Its prospective enrolment approach, protocol transparency, and adherence to ethical guidelines were evident. Patients were well informed in their local language, provided written informed consent, and ethical clearance was obtained. Different repertories were used in this as per the need of the case. The systematic conversion of data into an analyzable master chart facilitated organized extraction and statistical analysis. Validated outcome measures eliminated bias, with objective primary and subjective secondary outcomes. Treatment adhered to homeopathic principles, emphasizing individualization and symptom totality. Prescription of IHMPs, follow-ups, and the selection or change of dosage adhered to the state-of-the-art and classical principles of homeopathy and was strengthened further by adopting the consensus method of prescribing among three homeopathic physicians in each visit.
The study’s weaknesses include its short 4-month duration, reliance on self-administered measures prone to subjective bias, potential placebo responses due to rigorous case-taking, and the drawbacks of placebo-controlled RCTs such as incurred costs, limited generalizability, and potential loss to follow-up. The placebo effect, debated but clinically relevant, could stem from psychological or neurobiologic mechanisms, and placebo responses might reflect disease progression, symptom fluctuations, response bias, and concurrent treatments. While addressing the placebo effect is crucial for estimating intervention effects, placebo controls are vital for internal validity in clinical trials. 10
Earlier RCTs of IHMPs against placebos yielded diverse outcomes. In a 6-week double-blind RCT with 30 patients aged 45–75 years in South Africa, Morris et al. examined a combination of homeopathic complex and physiotherapy for osteoarthritis-related chronic LBP. 11 The complex included A. montana, B. alba, Causticum, Kalmia latifolia, Rhus toxicodendron, and Calcarea fluorica in 6cH potencies. The primary measurement was pain VAS, and secondary outcomes included ODQ, lumbar ROM, and pain medication usage. The treated group showed significant improvements in pain, daily function, and range of motion (ROM) compared with the control group. In a German RCT with 228 participants, Beer et al. evaluated the effectiveness of the homeopathic drug Lymphdiaral Basistropfen against placebos for chronic LBP. 12 Participants received the drug or placebo thrice daily for 105 days alongside naturopathic treatment, resulting in successful chronic LBP reduction with the homeopathic drug combination. The study by Pach et al. with 150 patients from German clinics employed a triple-arm, double-blind RCT to assess local injections of anthroposophic preparation Disci/Rhus toxicodendron compositum (verum) versus placebo injections and no treatment. The verum was more effective than no treatment, but not distinct from placebo in pain intensity reduction. 13 Stam et al.’s multicenter U.K. RCT evaluated homeopathic gel Spiroflor SRL against Cremor Capsici Compositus FNA in 161 acute LBP patients. Both treatments were equally effective, with SRL showing better safety. 14 In another double-blind RCT by Prakash et al. involving 49 patients with lumbar spondylosis, pain improvement was greater in the IHMPs group than placebo, but statistical significance was limited due to insufficient participants. However, certain subscales of secondary outcomes revealed significance at various time points. 10 Their trial was a replica of that of Prakash et al., with two exceptions as follows: (1) extended follow-up duration from 3 months to 4 months and (2) more precise selection of medicines through exhaustive use of repertories. When the results of this currently reported trial and that of Prakash et al. were pooled together in a random effect forest plot meta-analytic model, the mean difference favored IHMPs against placebos; −4.84 (95% CI −9.46, −0.23), z = 2.06, p = 0.04, τ2 = 4.16, I 2 = 33% (Fig. 2). Unlike these trials, the present study explored the efficacy of IHMPs for chronic LBP via a double-blind, randomized, placebo-controlled approach. With a sample size of 60, the study surpassed Morris’ and Prakash’s study sizes but was smaller than others. Unlike relying solely on pain VAS, the focus included symptom severity and LBP’s impact on quality of life through ODQ and RMPDQ assessments.

Forest plot random effect model.
In this study, the authors adopted a flexible approach for selecting repertories to address chronic LBP, ensuring that no single repertory was unduly favored. For instance, Kent’s Repertory was used when cases presented with characteristic mental, physical, and particular symptoms, and various repertorization methods were applied. The Synthesis Repertory came into play when additional factors such as family history, personal history, causation, or general modalities were involved. For example, a family history of asthma, aggravation during the new moon or full moon, or LBP after forceps or instrumental delivery were readily available in the Synthesis Repertory as rubrics or sub-rubrics. The Complete Repertory was employed for cases with mental symptoms (e.g., irritable pain during, doubtful recovery) and modalities (e.g., amelioration with hot applications) since it contains more medicines than Kent’s Repertory. The BBCR was preferred when the doctrine of complete symptoms, causation, and specific modalities were crucial but absent in other repertories (e.g., LBP aggravated by ascending stairs). Several cases were repertorized based on very peculiar and rare modalities related to LBP, given the limited 4-month study period. For example, Murphy’s Repertory was chosen when significant sensations like stiffness with LBP were not addressed by Kent’s repertory. Finally, for cases featuring clinical symptoms of LBP with limited mental and physical general symptoms, Boericke’s or Pulford’s repertory was selected based on specific symptoms like warm applications benefiting pain or relief from prolonged standing, respectively. This comprehensive approach ensured that each case was assessed with the most appropriate repertory, taking into account its distinct characteristics and symptoms.
Homeopathy proponents posit that LBP embodies a multimiasmatic nature. From the case records, this study identified sycotic miasm predominating in sensations and modalities, alongside psoric features, notably in mental and physical general symptoms. Overall, the research underscored LBP as a multimiasmatic ailment with a psoric predominance. While homeopathy’s foundation rests on individualization, certain remedies have recurrently proved relevant. Scholars like Dewey, Morrison, and Lilienthal cataloged remedies aligning with LBP symptoms. Similarly, Hartmann presented a roster, including A. tartaricum, Rhus toxicodendron, and A. montana. Notably, the study’s medications shared similarities with those advocated by Dewey, Morrison, Lilienthal, and Hartmann. 9 –12
Implications and future research suggest the need for larger RCTs using polarity analysis and cluster symptom approach conducted over a longer duration at multiple centers. In addition, exploring the effectiveness of 50 millesimal potencies of the indicated remedies should be considered for further investigation.
Conclusions
The inference drawn from the present work on chronic LBP revealed the efficacy of IHMPs in reducing pain along with disability measured with ODQ, RMPDQ, and SF-MPQ scores. Clinically significant improvements were observed in both groups. Group differences achieved statistical significance or near significance in all the specified outcomes; however, MCID could not be achieved. Larger and more definitive trials are warranted.
Footnotes
Acknowledgment
The authors are also grateful to other fellow postgraduate trainees, staff, pharmacists, and patients for their constant support and sincere participation in the study.
Authors’ Contributions
S.M.: Clinical study and data acquisition. Su.S.: Concept and literature search. S.G., R.K.P., Sa.S., Su.S., S.N., and Sk.M.A.: Clinical study and data acquisition and validation. S.R.: Clinical study and data acquisition and validation. A.S. and I.H.: Clinical study and data acquisition. P.G.: Design, concept, and literature search. M.K. and Su.S.: Design, data interpretation, statistical analysis, and preparation of the article. All the authors reviewed and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The project received no external funding. The institution has no role to play in the analysis of the study results and publication of the article.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.