
Abstract
Introduction:
Multiple sclerosis (MS) is a chronic inflammatory autoimmune disease that affects nearly 1 million people in the United States and 2.9 million people worldwide. The symptoms vary substantially but can include fatigue, lower extremity weakness, cognitive dysfunction, and mood impairment. The use of music to improve cognition, mood, and movement has been studied in numerous patient populations, yet the implementation for people with MS (PwMS) is understudied. This systematic review evaluates the effect of music-based interventions implemented with PwMS.
Methods:
The search used four electronic databases: PubMed/MEDLINE, CINAHL, PsycINFO, and Web of Science from January 1, 2002 to June 30, 2024. The inclusion criteria were (1) individuals diagnosed with MS, (2) music interventions, and (3) randomized controlled trials, quasi-experimental (nonrandomized controlled trials), and mixed methods studies. Outcomes included anxiety, depression, quality of life, and cognitive and functional (gait, balance, fatigue, dexterity) impairment. The risk of bias was evaluated with the National Institutes of Health Quality Assessment Tool.
Results:
A total of 15 studies were included, representing 623 participants. Most studies were conducted in Europe (n = 9). Ten studies were randomized controlled trials, and the remaining studies were quasi-experimental (case and match controlled). Intervention lengths varied from 1 session (n = 5) to 36 sessions. Most studies used receptive music engagement; the most common application was music listening while walking. Gait parameters and physical fatigue were the most common outcomes. These studies showed improved gait outcomes in music listening and active control groups. However, participants in the music interventions had less physical fatigue with activity. Four studies evaluated active music engagement interventions. Most active interventions were one session and evaluated memory through immediate and delayed recall of words sung to a melody compared with spoken words. In total, 73% of the studies evaluating motor neurological outcomes (gait, dexterity, and balance) had significant between-group improvements. Sixty-two percent of studies evaluating nonmotor neurological outcomes (cognitive functioning, fatigue, mood, and quality of life) showed significant between-group improvements. Methodological quality was assessed as fair or good for all the studies in the review. Safety and adverse event data were reported in 6/15 studies.
Discussion:
Music-based interventions show promise in improving motor and nonmotor outcomes in PwMS. However, the effectiveness of music-based interventions remains uncertain due to inconsistencies in methodologies and outcome measurements. Gaps in the research include active music engagement interventions, the impact of learning to play an instrument on cognition, and the delivery of interventions online and at home.
Registration:
PROSPERO #CRD42022338291.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory autoimmune disease characterized by progressive demyelination of the central nervous system that can lead to a variety of physical and cognitive impairments. 1 The neurodegenerative disease compromises motor, sensory, visual, and autonomic systems and can decrease the quality of life for people living with MS. 2,3 Affecting nearly 1 million people in the United States and 2.9 million people worldwide, the most common symptoms of MS include fatigue, lower extremity weakness, mood impairment, and cognitive dysfunction. 4,5 However, clinical manifestations of the disease vary greatly. 3 The rates of depression in people with MS (PwMS) range from 30% to 40%, while fatigue can be present in up to 85%–95% of people. 6 –8
Cognitive dysfunction can start early in the disease course and affect up to 75% of PwMS. 7,9 The most frequently affected domains are information processing speed and episodic memory. 10 –12 Even though self-reported cognitive dysfunction in PwMS is only moderately correlated with objective measures of cognitive impairment, it negatively affects the quality of life and affects mood and fatigue. 13,14 Many cognitive rehabilitative interventions have been developed to improve cognitive symptoms. A recent Cochrane Review of 44 memory rehabilitation interventions evaluated in randomized controlled trials found that patients who received memory rehabilitation reported better memory functioning and quality of life than those who did not. 13 Approaches to cognitive rehabilitation use restorative and compensatory strategies. Restorative cognitive rehabilitation focuses on improving and rebuilding the MS patient’s cognitive abilities, while compensatory cognitive rehabilitation solely provides management strategies. 13
Motor dysfunction associated with MS can include symptoms of weakness, spasticity, and dysfunction in balance and coordination, resulting in decreased gait speed, walking endurance, step length, and joint motion. 15 –17 Unlike other neurological conditions, no fixed deficit or symptom profile exists. Physical rehabilitation approaches are individualized, flexible, and depend on the individual’s physical limitations. Physical therapists provide exercises to maintain and strengthen physical abilities throughout the disease course. 18
The use of music to improve cognition, mood, and movement has been studied in numerous populations, including chemotherapy-induced cognitive impairment in women with breast cancer, 19 memory, mood, and cognitive functioning in people with Alzheimer’s disease and dementia, 20 and to improve movement in people with Parkinson’s disease. 21 Music perception, listening, and performance specifically engage in a complex cognitive system involving auditory scene analysis, attention, learning and memory, multimodal learning, emotion, and social cognition. 22 In addition, neuroimaging studies have shown that during music listening, perception, and performance systems are coactivated with auditory and motor systems. 23 The connections between these two systems help music cognition create predictions and expectancies associated with music perception and listening, leading to brain patterns and associations. 23
Music interventions can include active and receptive music engagement. In music therapy literature, active engagement is commonly categorized as playing an instrument, writing music, and singing. 24 In contrast, receptive engagement is described as the participant is “a recipient of the music experience, as distinct from being an active music maker.” 25; p. 15 Active and receptive music therapy interventions have improved physiological and psychological symptoms in persons with neurodegenerative diseases. 26 Within this review, we have categorized active music engagement as creating music by playing instruments or singing and receptive music engagement as listening to music while walking, meditating, or dancing.
The purpose of this systematic review is to examine the literature over a 22-year timeframe (2002–2024) that evaluated the effect of music-based interventions implemented with people living with MS. This timeframe was chosen because the insurgence of disease-modifying therapies that began in 2002 with the approval of Interferon-ß. Since 2002, the available treatment options, which have improved the length of life for PwMS, have increased substantially.
27
Understanding the current state of the science will facilitate advancements in future music-based studies for PwMS. This review will address the following questions: What are the characteristics of music-based interventions used for PwMS? How do music-based interventions affect motor (e.g., gait, dexterity, balance) and nonmotor neurological (e.g., cognition, fatigue, psychosocial well-being) outcomes in PwMS? Are there unique differences in outcomes based on active versus receptive music engagement?
Materials and Methods
A systematic review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting. 28 The details of PRISMA are shown in Supplementary Data S1. This systematic review was registered with PROSPERO (registration number: CRD42022338291).
Selection criteria
The inclusion criteria included (1) individuals diagnosed with MS, (2) music interventions, and (3) randomized controlled trials, quasi-experimental (nonrandomized controlled trials), and mixed methods studies. Exclusion criteria included: (1) individuals with forms of clinically isolated syndrome or radiologically isolated syndrome or other neurodegenerative diseases; (2) dissertations/theses, conference abstracts, case studies, qualitative studies, or commentaries. Outcomes included anxiety, depression, quality of life, and cognitive and functional (gait, balance, fatigue, dexterity) impairment. The additional search limitations were that studies were peer-reviewed, in English, and published between January 1, 2002 and June 30, 2024.
Search strategy and information sources
The review was conducted between June 2022 and June 2024 in four electronic databases: PubMed/MEDLINE, CINAHL, PsycINFO, and Web of Science. The following key terms were used in multiple combinations: music interventions, music therapy, MS, psychosocial well-being, mood, depression, anxiety, quality of life, cognition, gait, mobility, dexterity, and balance. To minimize selection bias, the reference lists of the articles obtained were reviewed to identify additional studies for inclusion. When necessary, authors of the publications were contacted to acquire further study details. The retrieval strategies in PubMed are shown in Supplementary Data S2.
Data screening and extraction
Article screening and review occurred in several phases, with an iterative process using the Covidence software. 29 Duplicates were automatically removed by Covidence. In every phase, two reviewers independently coded each article. In the title and abstract review, if a discrepancy occurred or sufficient information was not available in the abstract, the article was moved to the next phase of review. The full-text review phase had three coders (C.P., J.K., A.G.) per article, and one author (C.P.) provided an audit of the final articles for inclusion. Discrepancies at this phase were discussed with the coding team and resolved. Three authors (C.P., A.G., J.K.) extracted information from the studies. The following data were extracted: study characteristics (first author, publication year, and country), methods (study design and sample size), participants’ characteristics (gender, age, MS phenotype, years since diagnosis), intervention and comparison (intervention description, music details, delivery location, intervention facilitator, intervention length), outcome measures, and research results. During extraction, the reviewers were not blinded to authors or journals.
Assessment of quality
Three authors (C.P., A.G., J.K.) independently assessed the quality of the studies included in the review using one of the National Institutes of Health (NIH) Quality Assessment Tools. 30 In 2013, the NIH developed a set of quality assessment tools tailored to specific study designs to review study’s internal validity. The NIH Assessment of Controlled Intervention Studies tool was used for this review.
Statistical analysis
There was considerable heterogeneity in the included studies, mainly due to differences in MS phenotypes, control treatments, and outcome measures, which made it difficult to perform a meta-analysis. Accordingly, descriptive statistics were used to describe the sample, and qualitative descriptive analysis was used to report the outcomes. All relative data were synthesized in tables.
Results
Study and participant characteristics
In total, 326 citations were reviewed (Fig. 1). After abstract review, 34 studies were retrieved for full-text review. An example of a reason a study met the eligibility criteria but was eliminated is if the analysis was of duplicate data and outcomes. 31 After the full screening process, 15 articles were included for final review. 32 –46 All studies were conducted in Europe (Italy = 3, Belgium = 3, Austria = 2, and Turkey = 1) or North America (United States = 5). One study had a sample from the United States and Germany. Over half of the studies (9/14) were conducted within the past 5 years. The total sample size across studies in this review was 623 (range = 10–101). Of the studies that reported MS phenotypes (n = 8), 61% of participants had relapsing-remitting disease. Table 1 provides more detail about the participant demographics. A summary of each study's purpose, design, measured outcomes, and findings can be found in Table 2. Notably, 10 of the studies were randomized controlled trials. The remaining studies were controlled trials, but allocation was not randomized.
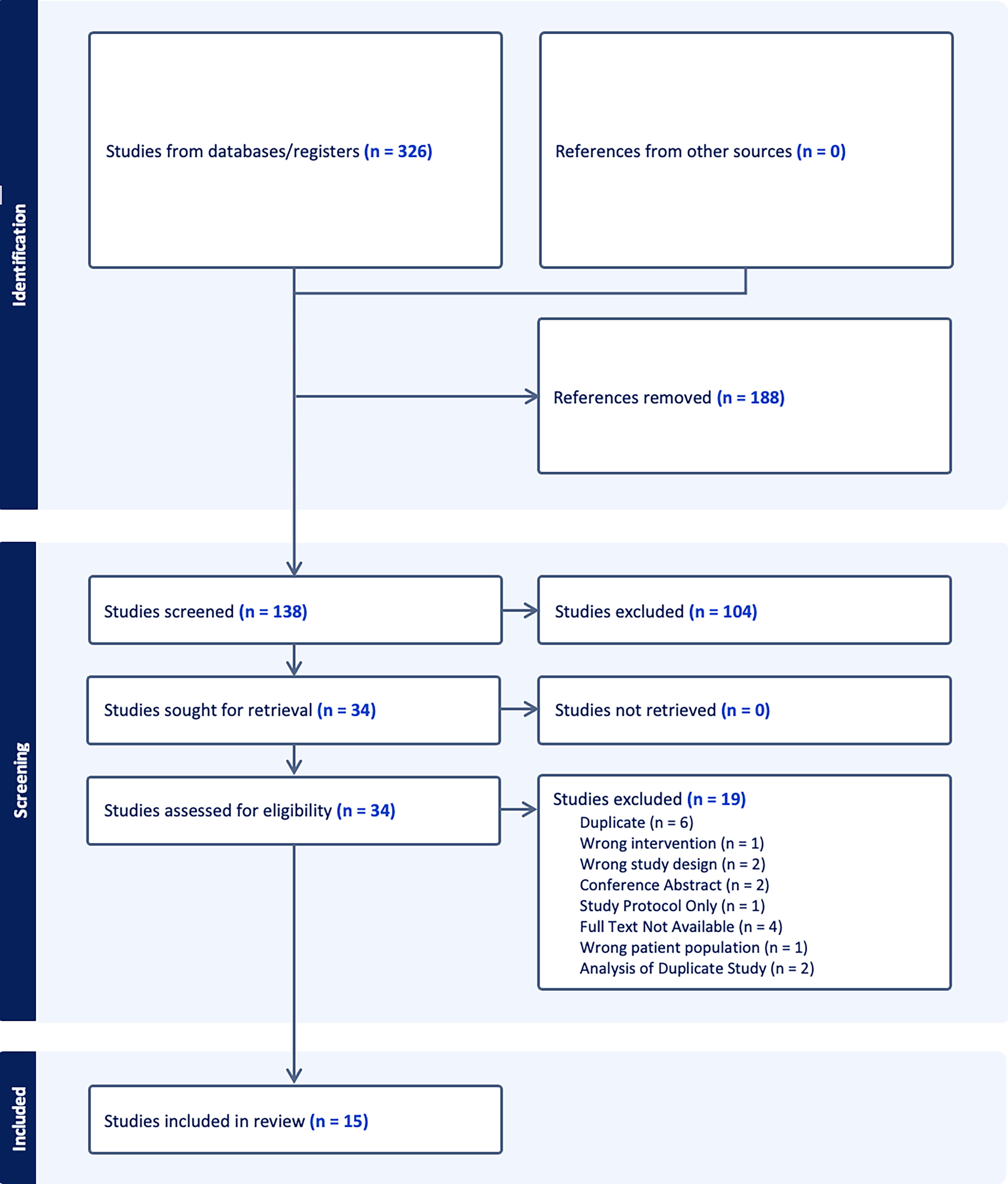
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Diagram.
Demographics
EG, experimental group; CG, control group; PP, primary progressive; RR, relapsing remitting; SP, secondary progressive.
Music Interventions for People with Multiple Sclerosis
AG, art group; DG, dance group; EG, experimental group; MI, motor imagery; QoL, quality of life; RCT, randomized controlled trial.
Intervention characteristics
Many studies in this review (n = 9) implemented music interventions to improve motor neurological outcomes such as gait, strength, spasticity, balance, and motor-auditory synchronization. Furthermore, 11 studies evaluated an intervention that used receptive musical engagement, such as music listening with or without activity. The length of interventions ranged from a single session to 60 min, 3 days a week for 12 weeks. Most session lengths were unique, yet five studies delivered the music-based intervention in only one session. Most interventions were delivered in the health facility or community center (n = 11), and only three were delivered within the participant’s home. The interventions were primarily delivered by research team members (n = 9). The remaining interventions were self-administered or delivered by a music therapist. More intervention characteristics are described in Table 3.
Music Intervention Components
CD, compact disc; LCD, liquid crystal display; NMT, neurological music therapy.
Interventions to improve motor neurological outcomes
Most motor neurological music interventions focused on improving gait. 32,35,37,38,41,45 Within the gait-driven interventions, rhythmic auditory stimulation (RAS), allowing for entrainment between the motor rhythm (recurrent footsteps) and auditory rhythm (recurrent beats or pulses), was most evaluated. RAS was operationalized in a variety of ways. Conklyn et al. 32 had participants listen to songs that had a tempo 10% above the participant’s spontaneous cadence. Maggio et al. 35 used a sound library created by music therapists that contained different metronome sounds and music that was adapted to the participant’s current and potential pace and then integrated the music with visual feedback to help the participant monitor their gait. Moumdjian et al. 38 evaluated walking to music and metronome at increasing tempos (0%, 2%, 4%, 6%, 8%, and 10% of the participant’s regular walking cadence), while Seebacher et al. 40,41 examined home-based music-cued motor imagery using motivating instrumental music with melodies and harmonies.
Other interventions targeting neurological motor outcomes were a “Movement to Music” intervention that incorporated multiple movement routines that targeted specific fitness components and were tailored to a tempo that matched the participant’s functional level, 45 a choreography-based dance therapy class implementing three different choreographies that increased in rhythm and difficulty, 44 and musical keyboard exercises to improve hand dexterity and function. 33
Interventions to improve nonmotor neurological outcomes
The nonmotor neurological interventions aimed to improve cognitive impairment, cognitive fatigue, and psychosocial well-being. Three of the five interventions in this category were delivered in a single session. The single-session interventions utilized music as a mnemonic device to improve memory outcomes on the Auditory-Verbal Learning Test. However, different approaches to this technique were examined. For example, Moore et al. 36 delivered the memory words to participants sung to the familiar song, “Skip to My Lou.” In comparison, Thaut et al. 42,43 had the 15 words from a memory test sung to participants in an originally composed melody that was unfamiliar to participants.
Two other studies evaluated the use of music therapy to improve cognition, mood, and quality of life. Impellizzeri et al. 34 used two different neurological music therapy techniques, “Associative Mood and Memory Training” and “Music in Psychosocial Training and Counseling.” Sessions included guided music listening, musical role-playing, expressive improvisation or singing, and composition exercises. Schmid et al. 39 implemented active music therapy, which involved participants and therapists actively engaging in music with instruments and singing. Participants also had the choice not to actively engage and instead listen to the music played by the therapist.
Interventions to improve both motor and nonmotor neurological outcomes
Two studies evaluated an intervention developed to improve both motor (gait/balance) and nonmotor (cognition/mood/quality of life) primary outcomes. 36,46 In Moumdjian et al., 38 participants were asked to step on seven different tiles presented in a specific sequence. Further, three different feedback modalities (melodic, sound, and visual) were used while the participants stepped on the tiles. Once they could correctly perform the sequence three times in a row, they were given a 3-min break. After the break, participants were asked to repeat the learned sequence three times in a row. Once successful, they were shown a distractor sequence, asked to perform the distractor twice, and then asked to perform the originally learned sequence immediately and 15 min later. Baştürk et al. 46 implemented one-on-one line dancing which includes a warm-up, line dancing, cool-down, and breaks as needed, under the supervision of an experienced physiotherapist. The dance routine was designed to improve balance, posture, and gait, and was taught progressively to manage fatigue. Sessions involved practicing individual steps, and then integrating them into a complete choreography set to music. Exercise intensity was adjusted based on heart rate and participant fatigue.
Intervention outcomes
Most of the studies had small sample sizes (≤40; n = 9), which may have resulted in underpowered studies impacting the evaluation of intervention efficacy. A summary of the most common outcome measures used, and a notation of statistically significant change (improvement, deterioration, or no change) was organized by active versus receptive musical engagement and displayed in Table 4.
Motor and Nonmotor Neurological Outcomes
AC, active control; HC, healthy control.
↑Significant improvement; –No significant change; ↓Significant deterioration; *Between group improvements; §Experimental group improvements.
Motor neurological outcomes
A total of 11 studies evaluated motor neurological outcomes such as gait, dexterity, and balance. 32,33,35,37,38,40,41,43,45,46 Eight of these 11 studies showed significant between-group improvements. 32,33,37,38,40,41,45,46 Overall, gait was the most frequently tested (n = 8) 32,35,37,38,40,41,45 and improved outcome (n = 6). 32,37,38,40,41,45 A variety of gait parameters were measured including the 6-min walk test (n = 4), the timed up and go test (n = 2), the 5 times sit-to-stand test (n = 2), the timed 25 ft walk test (n = 5), the spatiotemporal gait parameters (n = 2), and auditory-motor coupling synchronization (n = 1). Other improved outcomes were dexterity, 33,44 balance, 35,44 –46 physical functioning, 33 and strength. 33,44
Receptive music listening paired with walking was the most common music application and showed the most significant gains, with six out of eight studies showing between-group improvements (gait and balance). 32,37,38,40,41,45 The other two studies evaluating dance and movement-to-music interventions showed significant improvements in gait and balance within the groups, but no significant differences between the groups. 35,44 Overall, only 4 of the 10 studies reported effect sizes to help evaluate the potential impact and clinical effect on gait parameters. Effect sizes were given for timed up and go test (d = 0.7), 45 timed 25 ft walk test (η2 ranged from 0.143 to 0.581; d = 0.59), 32,40,41 and the 6-min walk test (η2 ranged from 0.112 to 0.596; d = 0.6). 40,41,45
Nonmotor neurological outcomes
Eight of the 13 studies that evaluated nonmotor neurological outcomes showed significant between-group improvements. 35,37,38,40 –43 Overall, cognitive functioning, physical fatigue, and quality of life were the most tested outcomes. The most improved outcomes were cognitive fatigue (75%) 37,38,40 and physical fatigue (50%). 37,38,41 Quality of life was measured in seven studies; however, between-group improvements were seen in only two studies. 40,46 Similarly, cognitive function was evaluated in seven studies, yet only two studies found between-group improvements. 42,43 Only one of the five studies that evaluated the impact of interventions on depression showed improvement. 38 Despite the lack of statistical significance, a large effect size (d = 0.83) was observed in the post-intervention scores in one study. 46
There was heterogeneity among the instruments used to measure many of the nonmotor neurological outcomes. Specifically, five different instruments were used to measure the quality of life (MS Impact Scale, Short-Form Health Survey [SF-36], Euro-5D-3L, MS Quality of Life, and the Hamburg Quality of Life Questionnaire in MS), four instruments to measure physical fatigue (PROMIS Short-Form 8a, Modified Fatigue Impact Scale, Fatigue Severity Scale, and a visual analog rating scale), three different instruments were used to measure cognitive functioning (Brief Repeatable Battery of Neuropsychological Tests in MS, Rey’s Auditory-Verbal Learning Test, and a description of cognitive performance during an experimental task), and two instruments to measure cognitive fatigue (cognitive fatigability index taken from the Paced Auditory Serial Addition Test and a visual analog rating scale).
Active and receptive musical engagement
Six of the 14 studies evaluated at least partial active musical engagement. 33,34,36,39,41,43 Half of the six studies evaluated using a musical instrument, 33,34,39 and the other half used singing to remember words during neuropsychological testing. 36,42,43 This form of engagement was only implemented once and occurred during the testing period. Memory improved in two of the studies. 42,43 Alternatively, the three studies that utilized partial or complete musical instrument engagement were delivered over 8–24 sessions. Only one study evaluating keyboard playing showed significant between-group improvements (physical functioning). 33
The other nine studies implemented receptive musical engagement. 32,35,37,38,40,41,44 –46 All the interventions included physical activity such as music with movement, 40,41,45 walking, 32,35,37 dancing, 44,46 and stepping. 38 While two studies 37,38 implemented the intervention once, seven studies delivered multiple sessions at least 2 weeks and up to 12 weeks. Gait improved in all eight studies assessed after the intervention, with six of these studies showing significant between-group improvements.
Safety and adverse events
Six studies 32,34,38,40,41,44 reported safety and adverse events data. No participants were harmed in the studies, and if a participant could not perform one of the tests because of safety concerns, data were not collected. Two studies reported falls. Seebacher et al. noted that one participant fell without being injured and after a short break the participant was able to repeat the test twice without falling. 40 Conklyn et al. reported that one fall occurred during the entire duration of the study, but it was not during the intervention. 32
Risk of bias and quality assessment
Using the NIH Quality Assessment Tool of Controlled Intervention Studies, 15 studies were reviewed for study quality (Table 5). 30 A total of 14 questions were answered to evaluate the potential for bias. Overall ratings of poor (0–4 out of 14 questions), fair (5–9 out of 14 questions), or good (10–14 out of 14 questions) were assessed. The methodological quality was assessed as fair or good for all the studies in the review. There were several strengths of the studies, including low dropout rates (n = 14), use of valid and reliable study measures (n = 15), a priori specification of outcomes and groups (n = 15), and all randomized controlled trials used intention-to-treat analysis. Limitations of the studies included small sample sizes (range = 10–40, n = 9), lack of blinding of participants and interventionists (n = 15), lack of blinding researchers to participant group assignment (n = 11), and lack of reporting sufficient sample size to detect a difference in outcomes (n = 12).
Quality Appraisal
CD, cannot determine; NA, not applicable; NR, not reported.
Quality was rated poor (0–4 out of 14 questions), fair (5–9 out of 14 questions), or good (10–14 out of 14 questions).
Discussion
The purpose of this systematic review was to identify and synthesize evidence on the effectiveness of music interventions for people living with MS. Specifically, this review sought to delineate the differences between active and receptive music interventions on motor and nonmotor neurological outcomes. The review included 15 studies published over 22 years and predominantly conducted in Europe and North America. The studies varied in design, sample size, intervention type, and outcome measures, which allowed for a comprehensive evaluation of the current evidence on music interventions in MS yet limited the ability to compare the findings directly.
Over half of the interventions used receptive music engagement to improve gait parameters. Three of these studies had a healthy or active control group (i.e., adapted yoga, metronome, and noncued or verbally cued motor imagery). 37,40,41 In these studies, all groups improved gait, but the music arms were superior because physical fatigue also improved. Exercise interventions have been shown to improve physical and cognitive outcomes in PwMS. 47,48 However, participation in physical activity is lower in PwMS compared with the general population. 49 High levels of physical fatigue are a barrier affecting physical activity levels. 50 One explanation for this difference is that music is a natural motivator and provides a distraction. Further, by engaging the rhythmic auditory system, physical activity may require less perceived effort. Numerous studies have shown that listening to music can improve mood, motivation, arousal, and perceived effort. 51 This finding has potentially high clinical relevance, may fill a significant gap in improving gait and physical function in PwMS, and warrants further research.
In contrast to motor outcomes, the impact of music interventions on nonmotor neurological domains varied across studies. Improvements in mood and quality of life were less consistently observed across studies, suggesting that although music interventions may influence these domains positively, the effects may vary based on intervention type and participant characteristics. Receptive and active music interventions demonstrated positive effects on cognitive functioning, albeit with varying degrees of improvement compared with active controls. Although most music intervention arms improved, there was no difference compared with the active control. Notably, these interventions were limited in frequency and duration compared with receptive music interventions. For example, Thaut et al. 42,43 used sung words compared with spoken words to improve verbal memory, but active music engagement only occurred during the testing. Clinically, these findings suggest that music interventions can potentially enhance cognitive abilities in individuals with MS, but more research is needed to examine the effect of music-based interventions on cognition.
Similar gaps exist in the research examining the use of music interventions in other neurological conditions that cause cognitive impairment. 52 A recent scoping review found that playing a musical instrument correlated with positive cognitive abilities in older adults. 53 Playing a musical instrument involves intricate coordination and communication between multiple sensory systems (visual, auditory, tactile) and motor functions. 54,55 As one visually looks at notes and translates them into physical actions, they simultaneously receive feedback from the auditory system to correct specific fine motor functions or keep the current status. The ability to engage these systems and coordinate motor, sensory, and cognitive domains to create audible, logical, and accurate sound may induce new cortical pathways and rewiring, inducing neuroplasticity. 24 This rewiring in the brain created by repeated musical practice may create alternate pathways and structures that may help PwMS compensate for deficits caused by the demyelinating disease. Overall, a significant gap exists in examining the use of music interventions to improve cognition for PwMS. More research is needed to understand the application to daily living and the long-lasting effects on day-to-day cognitive impairment.
This systematic review identified substantial variability in intervention characteristics, including the type and duration of music interventions. Interventions ranged from simple music listening sessions to more complex activities such as learning words sung to melodies or engaging in musical instrument play. This variability highlights the versatility of music as a therapeutic tool in addressing a wide range of impairments associated with MS. However, most interventions were delivered in clinical settings rather than at home, potentially limiting accessibility for individuals with mobility challenges. Future studies should explore the feasibility and efficacy of home-based music interventions to enhance adherence and long-term engagement among patients with MS.
Limitations
Several limitations of the systematic review should be noted, including the heterogeneity of control groups and outcomes as well as small sample sizes that caused many studies to be underpowered. This variability complicates direct comparisons between studies and limits the generalizability of findings. Additionally, the review was limited to studies published in English, potentially introducing language bias, and only included published studies, which may introduce publication bias.
Conclusion
While the potential of music-based interventions in improving both motor and nonmotor outcomes in individuals with MS is promising, the evidence base is still in its early stages. The adaptability of music interventions, whether through active engagement like playing instruments or receptive engagement like listening to music, allows for personalized approaches tailored to individual patient needs and preferences. This systematic review underscores the need for larger-scale studies with rigorous methodologies to establish the efficacy, optimal delivery methods, and long-term effects of music interventions in MS. Future research should explore the impact of active music engagement on mood and cognitive function, evaluate home-based interventions, and investigate the neuroplastic effects of music-making activities. By addressing these gaps, researchers and clinicians can advance rehabilitation strategies that enhance the quality of life and functional outcomes for people living with MS.
Footnotes
Authors’ Contributions
C.P.: Conceptualization, methodology, formal analysis, and writing—original draft; J.K.: Formal analysis and writing—review and editing; A.G.: Formal analysis; A.M.S.: Writing—review and editing.
Data Availability
Data collection forms, data extracted from included studies, and data used analysis are available upon request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study did not receive funding.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.