
Abstract
Purpose:
Children with cancer suffer from physical and psychological symptoms. Integrative medicine modalities (IMMs) for symptom management are increasingly popular, but whether these are acceptable to pediatric hematology–oncology (PHO) providers remains unknown. To address this knowledge gap and guide integrative medicine (IM) program development, a needs assessment was conducted to understand PHO provider knowledge, attitudes, and beliefs regarding IMMs for symptom management in children with hematologic or oncologic disorders.
Methods:
A detailed survey instrument was crafted using primary literature and expert opinion, iteratively reviewed for validity, and piloted tested by health care providers (HCPs). The survey was distributed electronically to patient-facing staff and stratified by clinical role. Survey response data from physicians and advanced practice providers (APPs) underwent descriptive analysis using SAS v.9.4 (Cary, NC).
Results:
A total of 78 PHO physicians and APPs completed this survey (response rate 29.5%). While most PHO physicians and APPs do not feel confident discussing incorporation of IMMs into the care of PHO patients, they are willing to (1) receive additional education in IM and (2) refer to a trusted IM provider. Providers do not believe that families typically disclose use of IMM to HCPs, and many worry about the use of entities such as high-dose vitamins and chiropractic care.
Conclusions:
PHO providers are concerned about the use of specific IMMs in their patients’ care but support massage and mindfulness almost universally. Most PHO clinicians are willing to engage trained IM providers and support strategies that may contribute to improved quality of life for their patients and families.
Introduction
Families of children with cancer experience significant distress with the diagnosis and treatment of a critical illness, and parents uniformly endorse effective symptom management as imperative. 1 –3 Distress throughout the course of illness is not limited to patients, as recent research also links parental distress to a child’s symptom burden. 4 Families may research complementary options to traditional medical therapies to aid in symptom management or attempt to positively influence cancer survival. 5,6 As medical information has become more easily accessible, many parents search for answers independent of their pediatric hematology–oncology (PHO) care team, particularly when curative options are no longer available. 7 Interest in complementary strategies, previously coined “complementary and alternative medicine” (CAM) is not new, and the current focus of this field, now known as integrative medicine (IM) or integrative oncology (IO; for patients with cancer), is to address refractory symptoms and promote healthy behaviors during traditional cancer-directed therapy. 8
Although no national dataset specific to IM use in children with cancer exists, several smaller, heterogeneous North American studies from the year 2000 and later have shown that 36%–84% of pediatric patients with cancer use complementary therapies during treatment. 9 –12 Data captured by the National Health Interview Surveys (NHIS) demonstrate that, of participating families with children aged 4–17 years (N = 17,321 families with N = 10,218 children), 11.6% of children used at least one CAM modality over the previous 12 months. 13 The most common interventions were nonvitamin, nonmineral dietary supplements (5.2%) and movement therapies such as yoga, Tai Chi, or qigong (3.2%). 13 The overall use of complementary modalities was even higher (21.3%) among children diagnosed with chronic pain conditions. 14 The National Health and Nutrition Examination Survey found that 33.2% of children aged 0–18 years use dietary supplements. While multivitamins were the most common, a significant increase in the use of over-the-counter supplements such as omega-3 fatty acids and melatonin was seen over the 10-year period between collection time points (3.7% in 2004 vs. 6.7% in 2014, p < 0.001). 15 It is also documented that children with comorbidities are more likely to use IM modalities (IMM), and IMM use is ubiquitous in adult cancer care. 13,14,16,17 Altogether, it is exceedingly probable that children with cancer are engaging in complementary practices and using bioactive supplements at rates comparable with the general pediatric population and with increased frequency compared with the past.
The National Center for Complementary and Integrative Health (NCCIH) now organizes IMM into four groups as follows: (1) nutritional (special diets, dietary supplements, herbs, probiotics); (2) psychological (meditation, hypnosis, music, and relaxation therapies); (3) physical (acupuncture, massage, physical manipulation); and (4) combination modalities that may span psychological and physical categories (yoga, Tai Chi, dance therapy). 18 Oncology providers are skeptical about the use of IMM in the care of patients with cancer due to lack of efficacy evidence and the potential negative impact on cancer-directed therapies. 19,20 The American Society of Clinical Oncology (ASCO) and the Society of Integrative Oncology have recently developed and published several IO guidelines, yet these materials were developed with adult cancer care in mind. 21 –24 Foundational data incorporated into these cancer guidelines come from adult patients with cancer, primarily those with breast cancer diagnoses, and recommendations are specific to adults being treated for cancer and/or adult cancer survivors. While this work is foundational for IO, it cannot be integrated into pediatric cancer care without similar data in childhood cancer cohorts. Increased concern exists surrounding dietary supplements and herbal medications (nutritional modalities) that may lead to overlapping toxicity with traditional cancer therapies. 20,25,26 As the field expands, education for PHO providers in IMM may improve provider uptake of beneficial practices, particularly those that are less likely to overlap with traditional therapies, such as psychological, physical, or combination modalities, thereby improving patient quality of life. The goal of this needs assessment is to ascertain current pediatric oncology health care practitioner (HCP) knowledge and beliefs about IMM use in the PHO population. The authors sought to determine educational needs related to integrative care for PHO providers and collect data regarding providers’ concerns about IMM use to facilitate thoughtful IM program development. 27
Methods
Provider data were collected via electronic survey response. The institutional review board declared this project exempt.
A comprehensive review of the literature confirmed a lack of validated instruments to assess knowledge and attitudes toward IMM in PHO physicians. Metrics from prior studies 28 were combined with newly developed pediatric- and oncology-specific questions to create a cross-sectional survey instrument assessing provider knowledge, attitudes, and beliefs about IMM use for PHO patients. The instrument was reviewed by experts in the fields of PHO and IM and subsequently piloted tested by 17 HCPs of varied backgrounds for content and face validity. The instrument was iteratively edited based on HCP feedback. The finalized questions were electronically formatted in the DataSTAT electronic survey platform.
Surveys were delivered electronically to physicians (MD/DO, attending, and fellows) and advanced practice providers with clinical privileges (APPs; nurse practitioners and physician assistants) at St. Jude Children’s Research Hospital, a large pediatric-specific cancer institute in the United States. A cross-sectional survey was distributed in spring of 2021, and survey reminders were sent 2 and 4 weeks after initial distribution. The data platform closed 2 weeks after the final reminder giving all eligible participants equivalent time to participate in this convenience sample.
Survey responses were collected and summarized by descriptive statistics. Associations between selected questions were calculated using chi-square or Fisher’s exact tests. Adjustment for multiple tests required false discovery rate correction. Statistical analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC). Statistical analysis using chi-squared testing assured that the physician and APP cohorts were not different in terms of their personal use of integrative modalities, beliefs about IM education, or communication with patients surrounding integrative therapies. As such, physicians and APPs were analyzed as one cohort (Supplementary Table S1). Missing data were coded and tabulated as “missing” rather than any attempt to impute date.
Results
Seventy-eight of 264 (29.5%) invited physicians (n = 45, 57.7%) and APPs (n = 33, 42.3%) completed the survey, all of whom specialized in the care of children with hematology–oncology diagnoses. Most participants spend at least half of their time in direct patient care (74.4%). Their average age was 45 years (median 41, Q1–Q3 36–53 years, range 30–82 years), and most self-identified as female (67.9%) and White (82.1%). Christian religions were commonly identified (64.1%) and most participants rated themselves “moderately” to “very” spiritual (70.5%). Finally, 66.7% of participants used IMM for their own health and wellness, the most common modalities reported were massage (55.1%), vitamin/mineral supplementation (48.7%), yoga (29.5%), aromatherapy (25.6%), and meditation (24.4%). Complete participant demographics are presented in Table 1.
Pediatric Hematology–Oncology Provider Self-Reported Demographics
IMM, integrative medicine modality.
Less than a quarter of participants (24.0%) described feeling confident in their ability to answer patient and family questions surrounding IMM (2.7% very confident; 21.3% confident; Fig. 1A). When asked about their willingness to have an IM-trained provider discuss integrative therapies with their patients, most participants answered positively, highlighting a need for clinicians with dual training in IM for PHO patients (91.4%; (28.4% always; 35.1% often; 28.4% sometimes); Table 2).
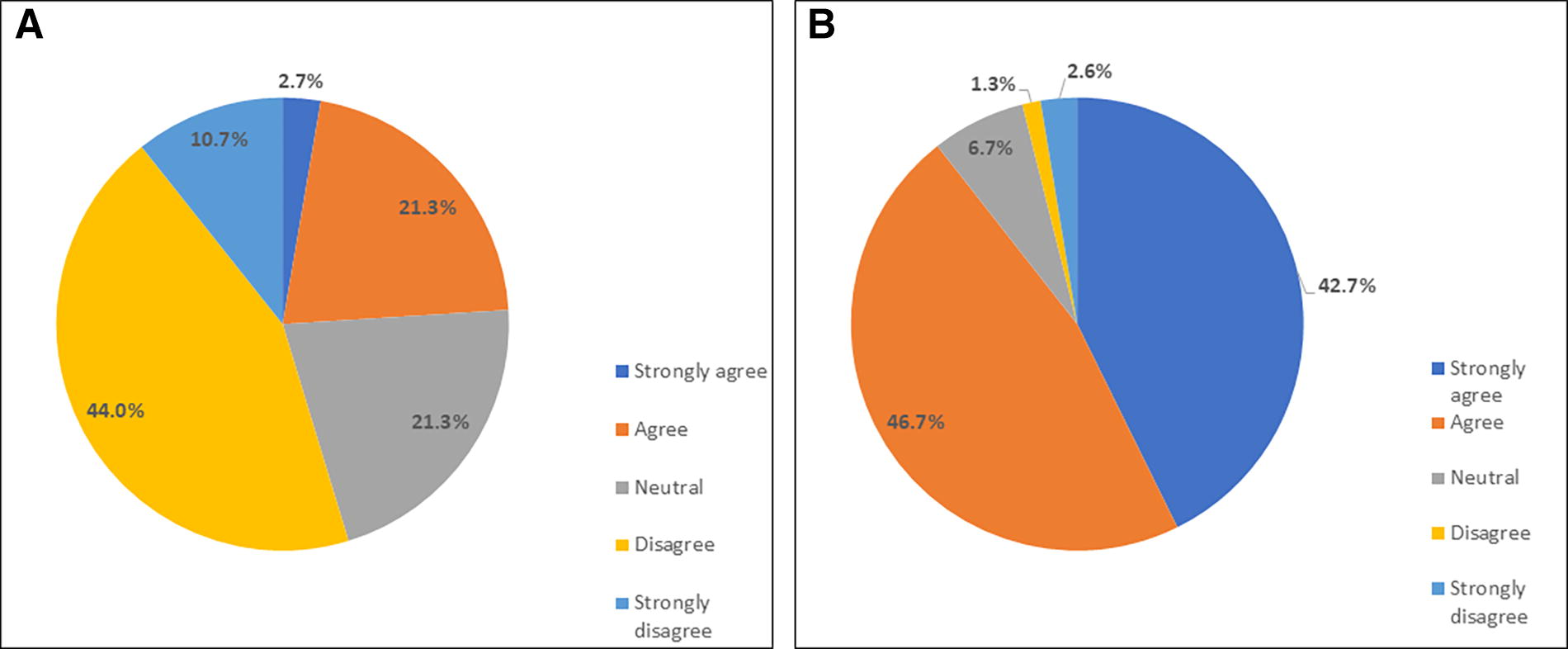
Pediatric hematology–oncology (PHO) provider beliefs about integrative medicine education. Figure 1A shows PHO providers’ self-rated confidence in speaking with patients and families about integrative medicine modalities. Figure 1B shows provider beliefs about integrative medicine education for themselves.
Pediatric Hematology–Oncology Provider Knowledge and Beliefs Surrounding Integrative Medicine Modality for Their Patients
Missing data n = 3 (N = 75 responses).
Missing data n = 4 (N = 74 responses).
Missing data n = 9 (N = 69 responses).
Missing data n = 6 (N = 72 responses).
IMMs, integrative medicine modalities.
Overwhelmingly, participants believe there should be more educational opportunities for HCPs on IMM use in the care of PHO patients (85.9% strongly agree/agree; Fig. 1B). For each of the following suggested topics, over half of participants were interested in receiving formal education pertinent to PHO patient populations: medical cannabis (61.3%), herbal supplements (56.0%), medical acupuncture (56.0%), meditation practices (56.0%), and massage (53.3%) (Table 2). Only two participants (n = 2.7%) noted that they would not be interested in learning about any integrative topics (Table 2).
PHO providers believe that IMM may benefit their patients by improving quality of life or relieving symptoms (Fig. 2A). Barriers to IMM use identified by PHO clinicians included lack of IMM providers specifically trained to care for PHO patients, concerns about safety of IMM, and beliefs that either they themselves or their patients are not interested in IMM (Fig. 2B). Providers endorsed concern about internet sites and/or “alternative” health care providers offering potentially harmful services to patients due to lack of education about the immunocompromised nature of the PHO patient population (Table 2).
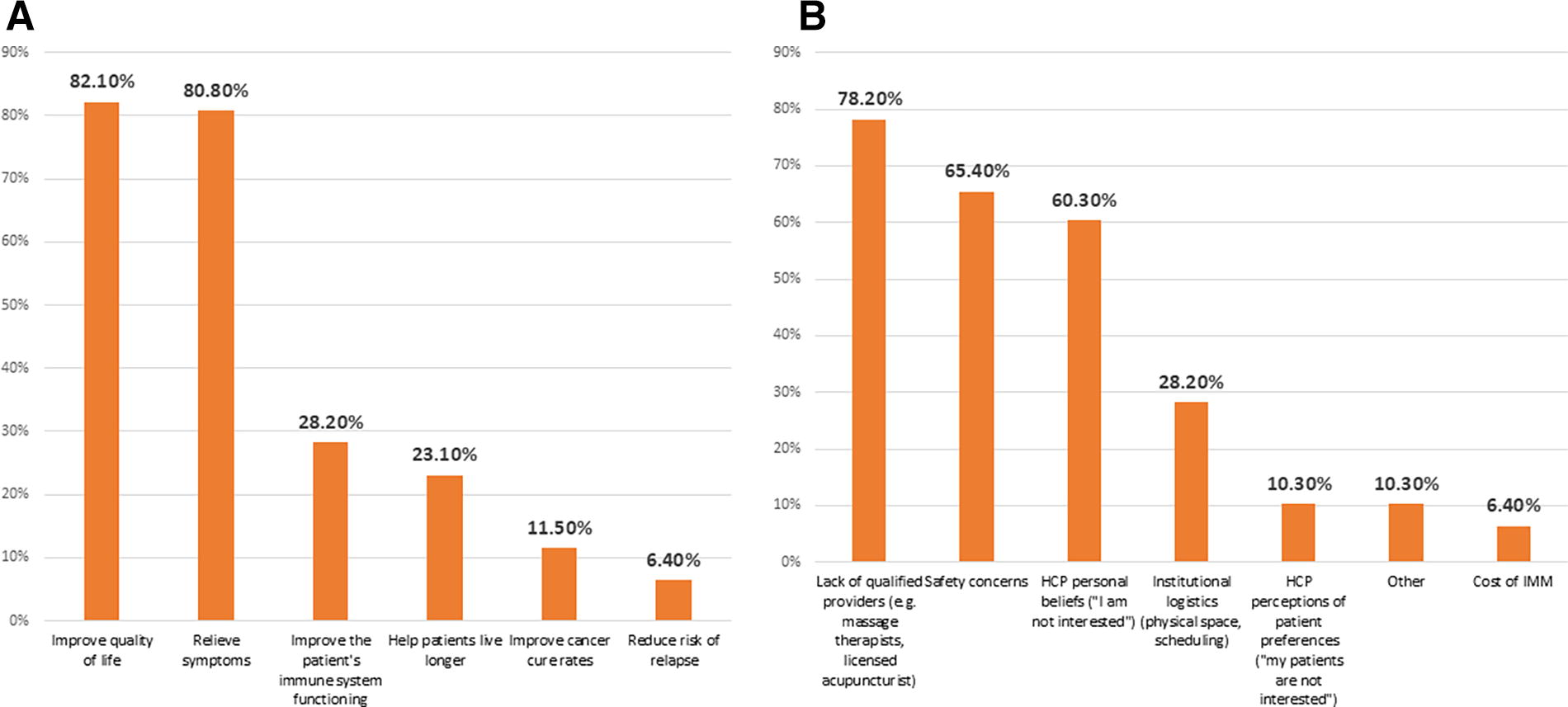
Pediatric hematology–oncology (PHO) provider beliefs about integrative medicine for patients. Figure 2A shows PHO provider-identified benefits for integrative medicine modalities (IMMs) for their patients, while Figure 2B documents recognized barriers to IMM for their patients.
Surveyed practitioners believe that patients and families typically do not disclose use of IMM to health care professionals (15.1% of HCPs believe patients “always” or “often” disclose, Fig. 3A) and that the primary reasons for family nondisclosure are concern about HCP approval (71.8%) and lack of questioning by HCP regarding IMM use (57.7%; Fig. 3B). Many HCPs (37.8%) note that discussions surrounding IMM use with patients and families are often (>75% of the time) initiated by the family rather than the provider (Table 2). Most HCPs (88.0%) noted discussing the use of herbal medications with 25% or less of their patients and reported that this conversation was almost always initiated by the family (Table 2). Participating HCPs universally acknowledged the importance of knowing about herbal medications or supplement use by patients (97.3% strongly agree/agree), but 62.8% of participants reported not knowing if the institution has a formal policy about herbal medications, and 16.7% answered this question incorrectly (Table 2).

Health care provider beliefs about patient perspectives toward integrative medicine modality (IMM) use. Figure 3A, B shows provider’s beliefs about patient disclosure of IMM use and potential reasons for nondisclosure. Figure 3C shows provider beliefs about sources of IMM for patient and families. Figure 3D details provider beliefs about patient/family motivations for IMM use.
HCPs believe that most patients and families receive information about IMM primarily from friends/family, social media, internet sites, and parents of other children with cancer (Fig. 3C). Only one respondent reported a belief that the primary oncology team is a major source of information for patients and families about IMM (Fig. 3C). Participants note that family interest in IMM use for their child is motivated by the desire to try every available option (67.9%), improve their child’s quality of life (55.1%), or maintain control (47.4%) or hope (32.1%). Few participants felt that the use of IMM is rooted in dissatisfaction with conventional cancer care (11.5%). Over 25% of providers believe patients may endorse integrative modalities for cancer cure (Fig. 3D).
Participants were asked about IMM of interest in the PHO community, and whether they believe that a particular modality was worrisome for PHO patients or could potentially improve a patient’s quality of life. The most “worrisome” practices to an HCP were multivitamins with dosages exceeding recommended daily allowance values (70.6% worrisome), chiropractic care (52.9% worrisome), and use of essential oils (either via simple inhalation (36.8%), diffused (38.2%), or topical (30.9%)). Interestingly, over half of participants noted that chiropractic care could improve patients’ quality of life despite being labeled “worrisome” by 52.9% (Table 3). Other practices that were noted to potentially improve patient quality of life were yoga, massage therapy, meditation training, and biofeedback, none of which was highly “worrisome” to clinicians. Clinician’s worry and perceived potential impact on quality of life for all queried complementary modalities are presented in Table 3. Finally, participants were asked if they would support the development of IMM for PHO patients. Yoga classes (95.7%), massage therapy services (92.7%), meditation training (92.7%), biofeedback (76.8%), and acupuncture (73.9%) were all highly supported (Table 2).
Pediatric Hematology–Oncology Clinicians’ Worries Regarding Integrative Therapy Use in Their Patients
N = 68 (n = 10 missing).
N = 69 (n = 9 missing).
Data not collected.
QOL, quality of life; RDA, recommended daily allowance.
Approximately two out of three PHO providers noted uptake of at least one IMM in their own self-care (Table 1). Providers who use IMM were more interested in learning about IMM for their patients (p = 0.003; Table 4) and more likely to refer their patients for IM consultation (p = 0.002;Table 4).
Associations Between Health Care Provider Personal Use of Integrative Medicine and Beliefs
Two missing data points were excluded (N = 75).
Fisher’s exact test.
IM, integrative medicine.
Discussion
Key findings: In this cross-sectional study of PHO providers, clinicians overwhelmingly noted that they had minimal, if any formal, evidence-based education in IMM, and were open to both increasing personal knowledge of IMM and referral access to an IM subspecialty provider. Participants noted they worry about patient disclosure of IMM use during cancer therapy, but many do not ask about or document use of IMM in the medical record. Finally, participants do recognize that IMM may help improve their patient’s quality of life through symptom mitigation. In fact, there was universal support for the development of yoga and massage therapy for patients.
IM cares for the whole person using evidence-informed modalities that complement conventional medicine. IO is the use of integrative principles for patients with cancer throughout the disease trajectory. 8 “Integrative” is the preferred term for complementary health practices used concurrently with conventional Western medical treatment, whereas “alternative” treatments are used in lieu of traditional medical therapy. 18 Previous literature has grouped modalities under the blanket term “complementary and alternative medicine” (CAM); however, most “alternative” strategies are not supported by IM-trained physicians, as they eschew conventional therapy by definition. Therefore, direct comparison of current practices with previous studies in PHO populations is fraught with inaccuracies due to the heterogeneity of patient, disease, modality, as well as nomenclature and definitions. 29 CAM practices, dietary supplements in particular, have not been traditionally supported in the PHO population due to patient age, side effects, and health compromise from cancer therapy, lack of accurate dosing, and increased risk due to potential immunocompromise. 30 Concerns about IMM may be partially attributed to the historically murky and overlapping definition of CAM, while low-risk IMM (such as massage or yoga) may be more palatable to providers caring for children with cancer. Underlying health beliefs of PHO HCPs may influence the care they recommend as data are lacking for many IMMs, particularly in children, and even more so in children with cancer. 31
In general, IMMs falling into psychological, physical, or combination practices are unlikely to interact with traditional cancer therapy and may be easier to integrate into PHO care, as noted above. Alternatively, the use of nutritional or dietary supplements may be of higher concern to providers. When asked specifically about IMM by definitional category, most PHO clinicians found physical, psychological, and combination practices less worrisome and potentially beneficial in terms of patient quality of life. This suggests that the development of programs focusing on these specific interventions might be supported. Compelling reasons for HCP education in IMM include patients and family interest, and growing evidence of potential benefits for symptom management during cancer therapy and beyond. 29,32 –37
PHO clinicians overwhelmingly noted that they had minimal, if any formal, evidence-based education in IMM. Unfortunately, this has not improved since the last published study of PHO physicians in the United States in 2009. 30 Previous work has detailed that medical schools in the United States spend little time educating student doctors about IMM. Students receive, on average, 2 h of education focused on integrative interventions during medical school. 18 Some medical schools offer elective courses in complementary and integrative medicine, yet few focus on the evaluation of medical literature, and most are < 20 h. 38 Until recently, most IM resident- or fellowship-level educational programs focused on IMM for adult patients. 39,40 In surveys of adult and pediatric physicians, providers linked a lack of opportunity and unmet educational needs to decreased confidence in conducting evidence-based discussions with patients. 41,42 Importantly, participants in this study recognized educational needs, were interested in learning to counsel patients, and noted openness to IM specialty referral. Together, these findings speak to the need for both general IM education for HCPs and subspecialty IO training for PHO clinicians.
Participants believe that most patients do not disclose IM use and reported that they rarely ask about or document use. At minimum, it behooves PHO clinicians to ask about the use of IMM, in particular those that fall into the NCCIH “nutritional” category, due to concern for interaction with disease-directed therapies, and document use in the patient’s medical record. 18 Under DSHEA law, herbal and dietary supplements are not prospectively regulated as medications. 43 A massive information gap remains surrounding efficacy, dosing, and safety of supplements for children receiving concurrent cancer-directed therapy despite individual supplements potentially being “generally recognized as safe.” If clinicians are not specifically asking patients about supplements, potential interactions or drug metabolism concerns may be missed when prescribing traditional medications. Several studies using medication:herb interaction programs document that adult patients with cancer using herbal medications may be at risk of a serious medication interaction (27%, 62%). 25,44 Although physicians hesitate to initiate this conversation when they may lack knowledge or resources to provide a risk–benefit evaluation, 45 potential patient safety issues may be overlooked if clinicians neglect to inquire. In a survey of ASCO members, 41% of participants reported discussing supplements/herbals with patients, and when they did, it was due to questions from the patient/family. 45 The participants were even less likely to ask about herbal products or supplement use (<25%), and these discussions primarily stemmed from patient/family query. A “don’t ask, don’t tell” policy is inconsistent with quality care as HCPs are unable to dissuade harmful practices or document potential concerns without inviting families into that conversation. 46 PHO clinicians should systematically ask about and document the use of all categories of IMMs to prompt discussion, avoid toxicity, and build trusting relationships. In patient/family queries, 40% of PHO patients using IMM noted they disclosed use to their provider reinforcing to clinicians that it is their responsibility to ask rather than assuming use will be disclosed unprompted. 47
PHO providers inherently care for their patients, and the enormous symptom burden in the PHO population dictates that providers educate themselves about health practices that may mitigate symptoms. Most participants agree that many of the queried IMMs may benefit patients by improving quality of life and/or relieving symptoms. Physical and psychological IMMs present minimal risk and should be supported if beneficial for an individual patient. In fact, two out of three providers noted that they use IMM in their own care, and this was significantly associated with increased interest in learning about IMM use for patients and referral to IM specialists. For many providers, the desire to benefit patients and their positive individual experiences with IMM are motivation to explore possibilities for their patients. Without advocacy from the PHO community, IMM will remain difficult to operationalize. While specialty training in IO is mandatory for large-scale program development, individual clinicians and hospital systems can begin to conceptualize how certain IMMs can be incorporated into their standard clinical care.
While this is a needs assessment of the largest PHO-specific NCI-designated cancer center, there are several limitations to the current work. First, providers in one center may have similar views about IMM based on shared practice models, geographic location, institutional “culture,” and/or common resources and policies. In addition, providers who are not interested in IMM may have decided to not participate (selection bias). Individual underlying health beliefs may also discourage (or encourage) a provider’s participation in this assessment such that nonparticipants may hold different views than providers who opted in. Pediatric IM offerings are notably scarce in the Southern US which may perpetuate clinician unfamiliarity. 48 Additional national survey-based assessments are vital to understand the barriers to implementation of IMM in PHO patient care in other geographic regions. The most recent national inquiry was published over 15 years ago, and presumably there has been increased PHO provider exposure to IMM. 30 Through their current work, the authors have developed and pilot tested a health care practitioner-facing survey instrument that they plan to use to collect national data. Most IM services are not reimbursed by insurance, so cost is a major barrier to widespread program development. Due to the unique funding mechanism of this institution, cost was not a barrier to services, but may inhibit generalization of results. 49 Several academic pediatric oncology organizations have special interest groups in IM that are collaborating to conduct research, and share data, policies, and protocols to expand IM services to children with cancer nationally. Finally, due to design, this represents a solitary point in time at this institution when no IMMs were offered. The authors have since developed a robust clinical IM program for patients that was thoughtfully created considering included clinician perceptions. Educational opportunities for PHO clinicians have also been created and presented. As this IM program develops, HCP beliefs regarding IM may be altered due to patient feedback and/or increased familiarity with offered complementary modalities.
Conclusions
Integration of IMM into the care of pediatric patients with cancer and blood disorders is fraught with barriers, including concerns about safety and efficacy. PHO HCPs believe that their patients are using IMM and acknowledge that they are not the primary information source regarding IM. HCPs acknowledge that they have minimal education, formal or informal, in the use of IMM in the context of PHO. Importantly, they are interested in gaining knowledge and skills. They recognize that patient, provider, and institutionally identified barriers may influence the development of IMM; nonetheless, they overwhelmingly agree that several modalities may be beneficial for patient quality of life and symptom management.
Footnotes
Acknowledgments
The authors thank the Integrative Medicine Working Group who have collaborated to develop integrative programming at their institution, and pilot tested the survey instrument. These dedicated clinicians have worked tirelessly to bring additional options to the patients and families. Finally, the authors thank Dr. Zhaohua Lu and Chen Li for statistical assistance.
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by H.S.-P., R.E.H., and D.R.L. The first draft of the article was written by H.S.-P. and all authors commented on previous versions of the article. All authors read and approved the final article.
Ethics Approval
The Institutional Review Board at St. Jude Children’s Research Hospital has deemed this project exempt from full review and confirmed that no ethical approval is required.
Author Disclosure Statement
The authors have no relevant financial or nonfinancial conflicts to disclose.
Funding Information
This research was supported, in part, by the American Lebanese Syrian Associated Charities (ALSAC) at St. Jude Children’s Research Hospital.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.