
Abstract
Objective:
Yoga has been recommended as a complementary management strategy for women with chronic pelvic pain (CPP), but many women lack access to specialized yoga instruction for this indication, and few data are available to evaluate changes in CPP with yoga. This feasibility trial evaluated the acceptability and tolerability of a remotely delivered yoga program for CPP in women and examined data quality and interpretability for measures of pelvic pain intensity and impact with yoga instruction.
Methods:
Ambulatory women with CPP were recruited from northern California in 2020–2022 and randomly assigned to a 2-month program involving twice weekly group classes delivered by videoconference supplemented by individual practice of pelvic yoga techniques versus a control program involving equivalent-time instruction and practice of nonspecific skeletal muscle stretching-strengthening exercises. Diaries, questionnaires, and in-class observations assessed intervention adherence and self-efficacy as well as CPP intensity and impact.
Results:
Among the 36 participants randomized (aged 27–77 years), the average (±standard deviation) baseline pelvic pain intensity was 4.2 (±2.0) (0–10 scale). Thirty-one (86%) completed the 2-month intervention programs, and 27 (75%) attended more than 85% of intervention classes. Among participants completing the yoga program (N = 16), 14 (87%) reported being at least moderately confident about performing all yoga postures after 2 months. Thirty (83%) provided pain intensity data at 2 months. Average pelvic pain intensity “at its worst” and “on average” were 1.9 (±1.6) and 1.1 (±1.4) points lower, respectively, after 2 months in this yoga group. Yoga participants also reported improvements in scores in the emotional, occupational, and psychological domains of the Impact of Female Chronic Pelvic Pain Questionnaire.
Conclusions:
Findings demonstrate the feasibility and acceptability of a videoconference-based yoga program and collection of pain-related data among women with CPP, paving the way for future research to rigorously evaluate its specific efficacy in representative samples of women.
Clinicaltrials.gov identifier:
NCT04615247.
Introduction
Between 10% and 20% of women suffer from chronic pelvic pain (CPP), a syndrome that can lead to depression, sexual dysfunction, physical inactivity, and pain-related disability. 1 –5 Due to the limitations of existing clinical therapies, many women are interested in identifying alternative or complementary treatments for CPP that are not only effective but better tolerated or more accessible. 6 –11 Yoga has been recommended as a community-based, patient-centered management strategy for CPP, 12 –14 given its potential to improve multiple contributors to this syndrome. When taught in a way that emphasizes mindful awareness of pelvic structures, deep breathing, and relaxation techniques, yoga can help women address pelvic floor hypertonicity, superimposed central pain sensitization, and overlapping perceived stress and anxiety 15 –24 that can lead to progressive disability.
However, many women with CPP live in communities without a high density of yoga instructors, especially those trained in yoga for therapeutic indications. Pelvic pain is also associated with high rates of interpersonal trauma that can affect willingness to engage in in-person, group-based interventions. 25 Telehealth options have been shown to mitigate trauma-related barriers to health care utilization, promoting a greater sense of emotional safety and willingness to engage in care. 26 With the rise of telehealth for delivering other forms of health care, there is growing interest in using digital technology to increase access to specialized yoga instruction for pelvic conditions. 27,28
Building on prior work by an expert clinical and yoga panel to develop a yoga program for female pelvic pain, 14 this report describes a feasibility trial of a remotely delivered, videoconference-based pelvic yoga intervention for women with CPP, based on a protocol approved by the University of California San Francisco (UCSF) institutional review board (IRB#19-29762) and registered in clincaltrials.gov (NCT04615247).
Materials and Methods
Design and participants
This was a randomized, parallel-group, investigator-blinded, multicenter feasibility trial of a remotely delivered pelvic yoga intervention (yoga) versus nonspecific skeletal muscle conditioning intervention (physical conditioning) for CPP in women. The goal was to evaluate the feasibility, acceptability, and tolerability of this intervention and collection of pelvic pain-related data.
From 2020 to 2022, participants were recruited from northern California by UCSF or Stanford University personnel, using community-based mass mailings and recruitment of patients from affiliated health care systems. Participants were self-identified women aged 18 years or older reporting pelvic pain for at least 6 months that was not exclusively associated with menses, with a pain intensity of at least 4 on a 0–10 numerical rating scale (NRS). Candidates were required to have undergone prior clinical evaluation to exclude reversible causes of pelvic pain requiring a fundamentally different treatment modality (e.g., pelvic infection). However, candidates could have other chronic pelvic health conditions (endometriosis, interstitial cystitis, irritable bowel syndrome), without restriction to any single diagnosis. All participants provided informed consent before enrollment.
Exclusionary criteria included pelvic surgery in the past 3 months or any history of pelvic cancer or irradiation. Candidates could not already be engaged in organized yoga or muscle-strengthening activities, nor other formal behavioral, psychological, or invasive pelvic pain treatments in the past month. Candidates using medications that could affect pain severity (including analgesics or antidepressants) had to confirm they were on stable doses for at least 1 month; those reporting recent initiation, discontinuation, or dose changes had to wait at least 1 month before enrollment.
All candidates had to be able to walk two blocks on level ground and get from a supine to a standing position without assistance. Access to an electronic device larger than a smartphone with videoconference capacity was required. Candidates were excluded if they had conflicts with intervention class times or could not complete procedures in English.
Randomization and blinding
Eligible participants were assigned in equal ratios to interventions based on a randomization scheme programmed by an independent statistician using SAS software, with randomly permuted blocks of sizes 2 and 4, and stratification by study site. Randomization was implemented in Medrio, the study’s electronic data capture system. Upon confirmation of eligibility, each participant was assigned a randomization ID by Medrio; once assigned, randomization was locked. Prior to randomization, the allocation sequence was concealed from study personnel. 29 Since intervention instruction was delivered through synchronous group classes involving approximately six students, with pre-established start and end dates, recruitment was organized in three successive waves, each designed to assemble a cohort of 12 participants (approximately half to each arm) to begin instruction on the same dates.
Participants were aware of their intervention assignment, as were intervention instructors and study staff assessing adherence. Investigators and staff evaluating or abstracting outcomes and safety data were blinded. To establish similar expectations of treatment success, participants were told they were participating in a trial of two different types of physical-based interventions, both of which had plausible mechanisms for improving CPP outcomes.
Interventions
The study yoga program focused on 16 postures widely used in Hatha yoga: Supta Baddha Konasana, Viparita Karani, Salamba Setu Bandhasana, Supta Padagusthasana (variations 1, 2, and 3), Ardha Ananda Balasana, Anjaneyasana (variations 1 and 2), Prasarita Padottanasana, Adho Mukha Svanasana, Utkata Konasana, Malasana, Salabhasana, Savasana, and Bhravajasana. Instruction emphasized tailoring the practice of postures to maximize awareness and control of the pelvic floor, reduce underlying stress, and improve physical function. Informed by the principles of Iyengar yoga, the program emphasized alignment and awareness of body structures during practice and used props to minimize the risk of injury.
For 8 weeks, participants engaged in twice weekly 90-min group classes led by instructors who were trained by the trial’s expert yoga consultants and had at least 2 years of previous experience teaching yoga. Instruction was delivered over an institutional videoconference platform (Zoom), and study staff guided participants in downloading and using platform features. Participants used their own computers or computer tablets but were given tablet stands or tripods to position their devices and cameras during class. Study coordinators guided participants in identifying spaces in their homes where they could position a yoga mat at an appropriate distance from their cameras, arranging lighting to shine on themselves rather than into cameras, and adjusting cameras to ensure visibility from head to toe in multiple positions.
Instructors followed a study-specific manual to introduce postures and call attention to ways postures could improve pelvic floor function. In early classes, instructors first demonstrated each posture and then observed students attempting the posture. After initial observations, instructors re-demonstrated postures to point out ways in which students’ performance of postures could be improved. Participants were also asked to practice yoga individually 1 h per week, using a manual with pictures and descriptions of postures. Instructors suggested specific postures for participants to focus on during self-directed practice. For example, one participant might be encouraged to practice Prasarita Padottanasana due to hamstring restriction; another might practice Salabhasana due to gluteus weakness. Participants were given a yoga mat, belt, two blocks, and bolsters to use in classes and practice.
The physical conditioning program featured equivalent-time group instruction and individual practice of nonspecific stretching and strengthening exercises to improve upper and lower extremity muscle conditioning but avoid engaging the pelvic floor. A personal trainer led twice weekly 90-min group classes after receiving training from the study’s physical therapist consultant. Participants were also asked to practice on their own 1 h per week using a manual. All received a stretch strap, resistance bands, and an exercise mat.
Measures/outcomes
Intervention instructors documented adherence to intervention classes using attendance logs. Participants documented self-directed practice on home practice logs. Self-efficacy in practicing postures or exercises was assessed using a previously developed self-report measure 30 in which participants rated their confidence in performing each posture or exercise (5—extremely to 1—not at all confident). During the last week of class, a study expert consultant also observed participants evaluate success in performing each posture or exercise (5—extremely to 1—not at all successful). For these assessments, the consultant considered specific alignment points, which varied for each posture, as well as participants’ ability to breathe normally while in the posture versus the appearance of discomfort or difficulty recovering normal breathing. Intervention acceptability was examined by structured questionnaires assessing participants’ perceptions of the benefits and disadvantages of videoconference-based intervention instruction.
Pelvic pain intensity was assessed at baseline, 2 months, and 4 months using diaries in which participants rated their pain severity/intensity on a standard 0–10 NRS, 31,32 including “at its worst,” “at its best,” and “on average.” Pelvic pain function/impact was assessed using the 26-item Impact of Female Chronic Pelvic Pain Questionnaire (IFCPPQ) yielding scores for five domains (psychological, sexual, relationship, emotional, occupational) and an overall score, 33 as well as the 8-item PROMIS Pain Interference Scale 8a. 34
To assess adverse events, study coordinators asked participants about any negative changes in their health at follow-up visits. Participants were also encouraged to call study staff to report any events between scheduled calls or visits.
Structured questionnaires also assessed participants’ demographic background, medical and reproductive history, medication use, mood symptoms based on the Center for Epidemiological Studies Depression-10 Scale 35 and Generalized Anxiety Disorder-7, 36 physical activity level, tobacco and alcohol use, interpersonal traumatic exposures using the Brief Trauma Questionnaire, 37,38 and post-traumatic stress disorder (PTSD) symptoms using the PTSD Checklist for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). 39 Participant height and weight were measured to calculate body mass index.
Statistical analyses
As the primary objective was to assess potential challenges to the feasibility and acceptability of the study protocol, the sample size of 36 participants was not driven by hypothesis testing or estimating precision of parameters but guided by considerations about the number of participants needed to reasonably field-test participant and study workflows. 40,41 The sample was designed to allow the study team to assemble three distinct and complete “cohorts” of 12 randomized participants, with half assigned to each intervention arm, consistent with a planned group intervention class size of six participants per yoga/exercise class. This amounted to three distinct trial runs of recruitment, intervention, and follow-up procedures, each involving different yoga instructors and study coordinators. Although influenced in part by practical reasons including time and budgetary constraints, this sample size was nevertheless larger than that of multiple previous pilot/feasibility studies of yoga interventions for pelvic conditions. 14,42,43
Baseline participant characteristics were summarized with mean, standard deviation (SD), frequency, and percentage in each randomized group. Feasibility of recruitment and retention was assessed by examining the proportion of candidates randomized, the proportion of randomized participants retained at 2 months, and the percentage completing at least 75% of intervention classes. Intervention feasibility was assessed by measuring the percentage reporting at least moderate self-efficacy in performing intervention techniques after 2 months, based on average self-efficacy ratings of 3 or higher. Feasibility of outcomes assessment was evaluated by examining completion rates for pelvic pain measures at 2 months and the quality and variability of pain measures data. As a simple composite measure of feasibility, investigators examined the cumulative number of participants who were randomized, did not drop out before 2 months, attended at least 75% of intervention classes, reported at least moderate intervention self-efficacy, and provided pelvic pain intensity data over 2 months. The composite feasibility goal was for at least two thirds (24) of the planned 36 participants to meet all criteria. Responses to questions about the benefits and disadvantages of videoconference-based instruction were also examined.
Average within-group changes in pain measures from baseline to 2 months and 4 months were examined in each group. By design, no between-group comparisons of pain intensity or impact were performed. Analyses were performed with SAS statistical software (version 9.4; SAS Institute Inc, Cary, NC).
Results
Among the 59 women screened, 36 were randomized, including 17 to yoga and 19 to physical conditioning (Fig. 1), approximately evenly distributed across three intervention waves (March–May 2021, September–November 2021, April–May 2022). One participant in the yoga and four in the physical conditioning group discontinued interventions early. Sixteen in the yoga and 15 in the physical conditioning group completed at least one pain outcome measure after 2 months. Twenty-six (or 72% of the randomized) met all trial feasibility criteria, including completing the 2-month intervention programs, reporting at least moderate self-efficacy in performing intervention techniques, and providing pain data at 2 months. The trial ended when a 4-month follow-up of the last participant was completed.
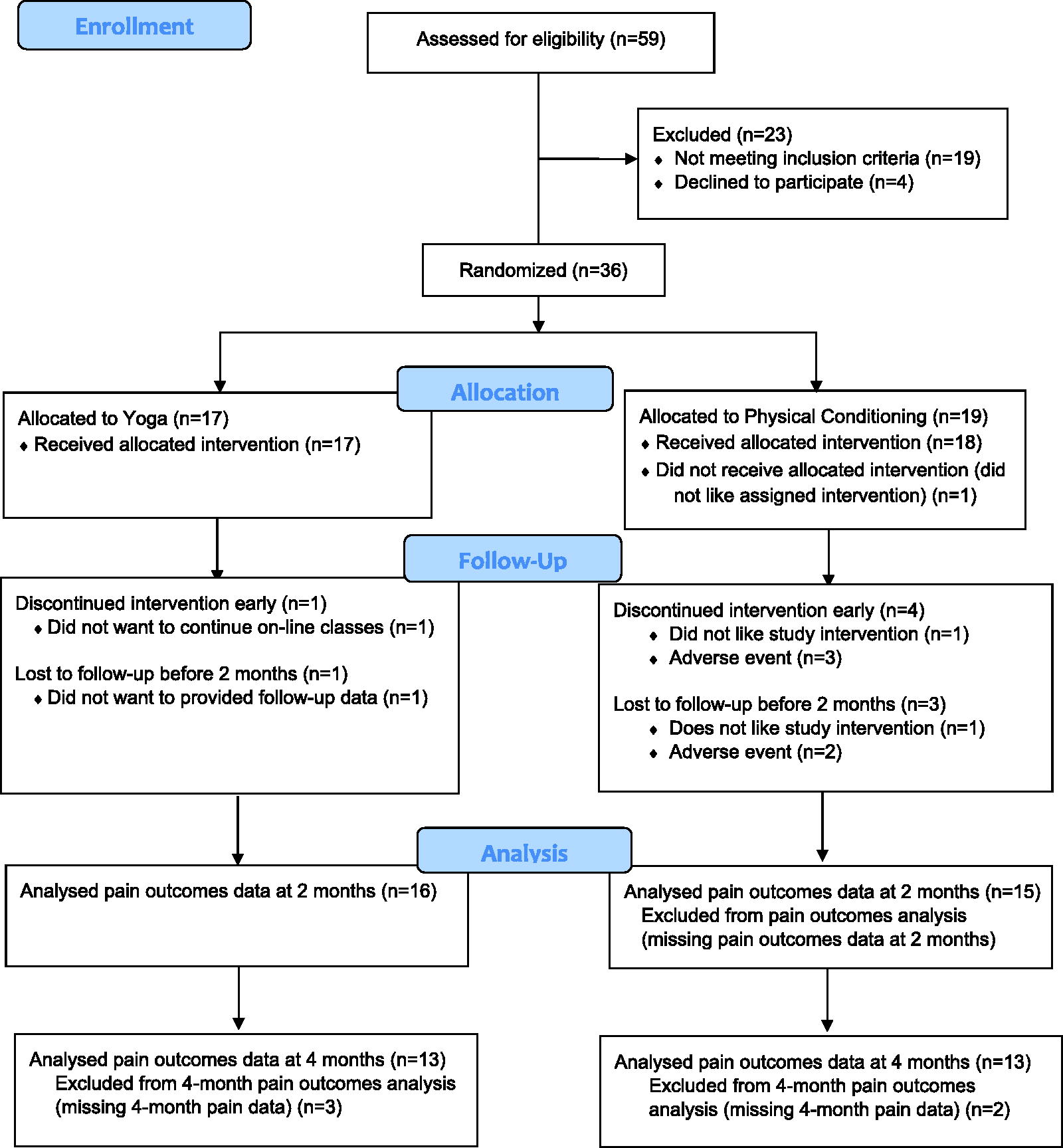
Consolidated Standards of Reporting Trials (CONSORT) flow diagram of recruitment, retention, and follow-up.
The mean (±SD) age of participants was 51.0 (±13.9) years (range 27–77 years), including one third self-identifying as ethnic minorities (Table 1). Participants reported multiple diagnosed pelvic health conditions including endometriosis, irritable bowel syndrome, and leiomyomata. The average pelvic pain intensity in the combined baseline sample was 4.2 (±2.0) on a 0–10 scale.
Baseline Participant Characteristics, by Intervention Assignment
Assessed by participant report of prior physician-diagnosed conditions.
Assessed by the International Physical Activity Questionnaire-Short Form.
Of the 16 participants completing the 2-month yoga program, 15 attended at least 12 (75%) of group classes (Table 2). Only 3 (21%) documented completing at least 75% of recommended individual self-directed practice hours. After 2 months, 13 of 15 yoga participants providing posture self-efficacy data (87%) were at least moderately confident about their ability to perform postures (Table 2). In an observed yoga intervention class at 2 months, an expert consultant judged 7 of 15 participants (47%) to be “very” successful in performing all postures, and all attending to be at least “moderately” successful in performing postures.
Intervention Adherence and Self-Efficacy Among Participants Completing 8-Week Intervention Programs
Data are presented as number (percentage), based on participants providing data for at least one measure at 8 weeks. Two participants in the pelvic yoga and five in the physical conditioning program failed to return home intervention practice logs. One participant in the pelvic yoga did not complete the 8-week intervention self-efficacy measure. One participant in the pelvic yoga and four in the physical conditioning group missed the session in which independent consults assessed participants’ ability to perform postures or exercises. Two participants in the pelvic yoga group were missing data on self-reported ease of continuing to practice interventions.
Adherence to group classes was assessed by attendance logs kept by the class instructors, while adherence to self-directed practice was assessed by practice diaries in which participants recorded the dates and times of their practice outside of class.
Participants rated their confidence in performing each of the core postures or exercises featured in the intervention programs on a 5-point Likert scale after 6 weeks (not at all, slightly, moderately, very, or extremely).
An expert yoga or physical therapist consultant visited the final group class of the program and independently rated each participant’s success in performing core postures or exercises on a 5-point Likert scale (not at all, slightly, moderately, very, or extremely).
Participants in both groups reported high levels of comfort with engaging in videoconference-based classes (Table 3). Participants also reported satisfaction with their ability to express their thoughts during classes and the convenience of participating in classes. However, some reported only a poor or fair sense of interpersonal connection to other participants over the videoconference platform. Additionally, yoga instructors noted challenges with checking participants’ alignment when restricted to observations over videoconference rather than three-dimensional space.
Participant Perceptions of the Benefits and Disadvantages of Videoconference-Based Intervention Instruction, by Intervention Group
Thirty participants (83%) contributed pain diary data at the end of the 2-month intervention program. Twenty-six (72%) met all criteria contributing to the composite feasibility measurement, including 14 (82%) in yoga and 12 (63%) in physical conditioning.
From baseline to 2 months, pelvic pain intensity “at its worst,” “at its best,” and “on average” decreased by an average of 1.9, 0.6, and 1.1 points, respectively, in the yoga group (Table 4), with persistence of change among participants providing follow-up data at 4 months. Over 2 and 4 months, mean scores on the IFCPPQ emotional, occupational, and psychological scales also decreased in the yoga group (Table 4). Participants also provided interpretable data from the PROMIS Pain Interference scale over 2 and 4 months (Table 4).
Change in Pelvic Pain Severity and Interference Measures Over 2 and 4 Months, by Intervention Assignment
Data are presented as means (±SD).
SD, standard deviation.
Nine participants in the yoga (53%) and 10 in the physical conditioning group (53%) reported at least one adverse event. Five (17%) of the 30 events detected were categorized as being “probably” related to interventions, including 2 reports of muscle or joint pain in the yoga group, 2 reports of pelvic pain or inflammation in the physical conditioning group, and 1 report of upper extremity pain in the physical conditioning group. No serious adverse events were detected.
Limitations
Limitations of this trial include its modest size, which was not designed for evaluating intervention efficacy or safety, or other quantitative hypothesis testing. The trial enrolled participants with a variety of pelvic pain diagnoses and did not explore differences by diagnosis. Although intervention instruction was delivered by videoconference, only women residing in northern California were recruited. Further, most participants had a college education, and the feasibility and acceptability of videoconference-based yoga may differ by educational background. Since participants could have past experience with yoga (although none in the month before enrollment, and none specifically directed at pelvic pain), results may not be generalizable to women who are completely naïve to yoga.
Discussion
Despite interest in yoga as a complementary management strategy for women with CPP, few data are available to evaluate yoga interventions for this indication. In this multisite feasibility trial, more than 90% of women with CPP assigned to the yoga intervention completed the 2-month yoga program, and more than 85% attended at least 85% of group yoga classes. Based on both self-assessment and expert evaluation, participants were at least moderately successful in learning to practice study yoga techniques after 2 months. Participants also provided interpretable data for multiple measures of pain intensity and impact. Overall, these results provide promising evidence of the feasibility and tolerability of yoga as a complementary self-management strategy for CPP, while highlighting the need for additional research.
Our previous research 44 discussed changes in pelvic pain among women taking part in an earlier version of this yoga program involving in-person instruction. 14 However, enrollment was limited by candidates’ concerns about the difficulty and inconvenience of commuting to brick-and-mortar studios. Although past studies have examined online or videoconference-based yoga interventions to improve accessibility for other chronic pain conditions, 27,45 –49 data are scarce on videoconference-based yoga instruction for CPP.
While providing evidence of feasibility and acceptability, this study also reveals the limitations of remotely delivered yoga for CPP. Participants noted that videoconference-based instruction offered limited opportunities for meaningful interpersonal engagement. Additionally, participants reported relatively low rates of self-directed intervention practice outside of group classes, perhaps because the distinction between class and self-practice blurred when both took place in their own homes.
Further, while all yoga participants undergoing consultant assessments at 2 months were assessed as being at least “moderately” successful in performing yoga poses, less than half were assessed as being “very” successful. In contrast, all physical conditioning participants were assessed as being “very” successful in performing assigned exercises at 2 months. Further, less than two thirds of yoga participants, compared with more than 85% of physical conditioning participants, reported being “very” comfortable engaging in videoconference classes. Findings suggest that learning the physical forms of yoga over videoconference may be more challenging than learning nonspecific muscle conditioning exercises remotely, although further evaluation in larger samples is necessary to draw robust conclusions.
Conclusions
Findings from this feasibility trial support the acceptability and tolerability of a remotely delivered, group-based therapeutic yoga program for women with CPP and the feasibility of assessing changes in pelvic pain intensity and functioning among women engaged with this program. Larger randomized trials are needed to rigorously evaluate the unique efficacy and safety of yoga in comparison to other, nonspecific physical activity-based interventions, as well as identify facilitators and barriers to effective remote engagement with yoga for CPP. If found effective, remotely delivered yoga has the potential to provide a low-cost, accessible, community-based intervention for CPP.
Footnotes
Acknowledgments
The study team gratefully acknowledges the contributions of its project managers (Ann Chang and Lisa Abinanti), expert yoga consultants (Leslie Howard, YACEP, C-IAYT, E-RYT 500; Judith Hanson Lasater, PhD, PT, C-IAYT, E-RYT-500; and Susan McCormick, CIYT), yoga instructors (Emily Combs, E-RYT 500; and Katherine Lindberg, E-RYT 500), and physical conditioning instructor (Giana Lando, CSCS).
Authors’ Contributions
A.J.H.: Conceptualization, funding acquisition, investigation, methodology, project administration, supervision, visualization, writing—original draft, writing—reviewing. L.L.S.: Conceptualization, funding acquisition, investigation, methodology, project administration, supervision, writing—reviewing. T.S.R.: Conceptualization, investigation, methodology, writing—reviewing. M.S.: Data curation, formal analysis, methodology, software, visualization, writing—reviewing. H.R.: Data curation, formal analysis, software, visualization, writing—reviewing. M.T.C.: Conceptualization, funding acquisition, methodology, project administration, writing—reviewing. C.G.: Funding acquisition, investigation, writing—reviewing. J.C.: Supervision, writing—reviewing. S.P.: Methodology, resources, supervision, writing—reviewing.
Author Disclosure Statement
A.J.H. reports royalties from Wolters Kluwer and travel reimbursement and consultant fees from the American Medical Association. C.G. has provided unpaid consultation to Astellas Pharmaceuticals for projects unrelated to the current project, as well as travel reimbursement as a member of The Menopause Society Board of Trustees. No other authors report any potential conflicts of interest regarding this research.
Funding Information
This publication or project was made possible by Grant Number R34AT010356 from the National Center for Complementary and Integrative Health (NCCIH), R01AT012461 from the NCCIH and the Office of Research on Women’s Health (ORWH), and K24AG068601 from the National Institute on Aging (NIA). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NCCIH, ORWH, NIA, or the National Institutes of Health.