
Abstract
Introduction:
This scoping review evaluated the efficacy/effectiveness and utilization of complementary and integrative health (CIH) therapies for pain management within the Military Health System (MHS). Specifically, it aimed to assess evidence-based modalities such as acupuncture, biofeedback, hypnosis, massage therapy, meditation, guided imagery, Tai Chi/Qi Gong, and yoga, which are part of the Veterans Administration’s (VA) Whole Health program. The goal was to determine their effectiveness in military service members and understand their utilization in the MHS, as well as explore CIH research in the MHS to identify gaps.
Methods:
A comprehensive search of PubMed, Embase, and Ovid All EBM Reviews databases was conducted for studies published from January 1, 2014 to March 22, 2024. The search focused on CIH therapies related to pain management in military populations, yielding 433 studies. After screening for eligibility, 53 studies were included for detailed review. Studies included randomized controlled trials, case studies, large database analyses, and retrospective chart reviews. Exclusion criteria eliminated nonpeer-reviewed articles, not pain-related, not related to one of the prespecified CIH modalities (acupuncture, biofeedback, hypnosis, massage therapy, meditation, guided imagery, Tai Chi/Qi Gong, and yoga), and those not specific to the MHS. The review did not address bias due to the heterogeneity of study designs included.
Results:
The review identified significant evidence supporting the use of CIH modalities for pain management. Acupuncture, particularly Battlefield Acupuncture, showed immediate reduction in pain score for both acute and chronic pain. Studies of massage therapy and biofeedback demonstrated efficacy/effectiveness in reducing pain and improving functional outcomes in various musculoskeletal and stress-related disorders. Meditation and yoga were shown to be effective for chronic pain, stress management, and enhancing overall well-being. Utilization data indicated a steady increase in CIH therapy use across military facilities.
Discussion:
CIH therapies, particularly acupuncture, massage therapy, and yoga, appear to be effective nonpharmacologic interventions for pain management in military populations. Their growing utilization reflects the recognition of their benefits in managing chronic pain and improving quality of life among service members. Further research is needed to standardize practices and optimize utilization across the MHS.
Registration of Protocol:
PROSPERO 2024 CRD4202453685, 29 April 2024, https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42024536853.
Introduction
Acute and chronic pain are endemic in military service members and are a treatment priority within military medicine. Pain has substantial economic, operational, and personal impact within the Department of Defense (DoD). 1 –3 In the DoD Military Health System (MHS), rates of chronic pain (pain lasting at least 3 months) diagnoses quadrupled from 2007 to 2014. 4 Almost half (44%) of nontreatment seeking, active-duty, postcombat deployed service members report chronic pain. 5 Compared with their civilian counterparts, pain prevalence is higher in active-duty service members and veterans, and frequently follows combat deployments. 6,7 Musculoskeletal pain incidence is steadily increasing among Operations Enduring Freedom, Iraqi Freedom, and New Dawn veterans. 8 Pain-related conditions are economically costly and fuel military attrition in times of conflict eroding the fighting force. 2 Ensuring access to effective nonpharmacological treatments across the MHS could reduce the impact of acute and chronic pain and improve quality of life among service members and veterans. Examining the use of these therapies is critical to identifying gaps in access, as well as informing strategies to expand their availability to the active-duty population.
Complementary and integrative health (CIH) treatment modalities have been recognized as effective pain treatment options and have been implemented as part of the Veterans Health Administration’s (VHA) Whole Health System of care included in Department of VA Directive 1137—Provision of Complementary and Integrative Health (recertified December 2022). 9 CIH modalities in the VHA include acupuncture, biofeedback, hypnosis, massage therapy, meditation, guided imagery, Tai Chi/Qi Gong, and yoga. The VHA conducted a review of these approaches and determined them to be safe and supported as evidence-based care. 9 We used the Veterans Administration’s established list of medical CIH therapies to define the scope of our review because it provides a comprehensive and evidence-based framework that has been rigorously evaluated and implemented in a comparable health care system.
While CIH therapies have been extensively studied and implemented in the VHA, differences in population demographics and operational environments between the VHA and MHS warrant focused investigation. For example, the MHS primarily serves actively deployed service members and younger individuals facing combat-related injuries and operational stressors, whereas the VHA largely supports older veterans. These distinctions may result in varying utilization patterns and effectiveness of CIH therapies. Differences in population characteristics, care delivery models, and operational demands necessitate further research to understand CIH implementation in the MHS context.
While the evidence base on the efficacy/effectiveness of CIH therapies for pain is growing, utilization of these modalities in the MHS is less clear. Acupuncture has been explored in military settings as a nonpharmacological approach to pain management, with protocols such as battlefield acupuncture developed for quick deployment in field conditions. 10 Likewise, biofeedback and hypnosis were integrated selectively within military mental health programs for stress and pain management, particularly for managing post-traumatic stress disorder and combat-related chronic pain. 11,12 Emerging research and policy changes have encouraged broader integration, supporting these modalities as viable components of holistic care for active-duty personnel and veterans. 12,13 Despite these developments, a lack of standardized training and credentialing across facilities has often limited consistent application. 14
The goal of this scoping review is to describe CIH efficacy/effectiveness and utilization in the MHS within a framework of evidence-based practices incorporated in the VA’s Whole Health program 15 addressing the following questions: 1) What is the state of the science for each one of these modalities for pain management for military service members; and 2) What is the state of utilization of these modalities in the MHS and what are the gaps?
Materials and Methods
This scoping review examined the efficacy/effectiveness and use of acupuncture, biofeedback, hypnosis, massage therapy, meditation, guided imagery, Tai Chi/Qi Gong, and yoga within the MHS. The review focuses on studies conducted and published between 2014–2024. We used the VA’s list of CIH therapies to define the scope of our review, as it offers a validated, evidence-based framework relevant to comparable health care systems. The research was conducted in accordance with Institutional Review Board requirements under a protocol deemed exempt from full review.
The review was registered with Prospero. The search, title and abstract screening, full-text review, and data extraction steps were performed using Covidence (https://app.covidence.org). We did not include the funding source PRISMA 16 field.
Search strategy
A research librarian performed the literature searches using PubMed, Embase, and Ovid All EBM Reviews (Cochrane) databases. The search strategies are specified below for each database. A combination of subject headings and keywords were utilized to fully represent the concepts of pain, CIH therapies, and various military terms.
The following filters were used for each database search: English language; Date Range: 2014–present; and Document types: journal articles. All searches were performed on March 22, 2024. The specific search terms used for each database were as follows:
PubMed
(“Acupuncture”[mh] OR “Acupuncture Therapy”[mh] OR “Biofeedback, Psychology”[mh] OR “Complementary Therapies”[Mesh] OR “Hypnosis”[mh] OR “Massage”[mh] OR “Meditation”[mh] OR “Qigong”[mh] OR “Tai Ji”[mh] OR “Yoga”[mh] OR alternative-medicine[tiab] OR biofeedback[tiab] OR complementary-medicine[tiab] OR complementary-therap*[tiab] OR integrative-health[tiab] OR massage*[tiab] OR acupuncture[tiab] OR yoga[tiab] OR meditation[tiab] OR hypnosis[tiab] OR guided-imagery[tiab] OR tai-chi[tiab] OR tai-ji[tiab] OR qi-gong[tiab] OR qigong[tiab]) AND (“Pain”[mh] OR “Pain Management”[mh] OR pain[tiab]) AND (“Military Personnel”[mh] OR active-duty[tiab] OR air-force[tiab] OR airmen* [tiab] OR armed-forces[tiab] OR armed-services[tiab] OR army[tiab] OR guardian*[tiab] OR marine-corps*[tiab] OR marines[tiab] OR military[tiab] OR navy[tiab] OR sailor*[tiab] OR servicemember*[tiab] OR service-member*[tiab] OR soldier*[tiab] OR space-force*[tiab]) AND english[lang] AND (2014:3000/12/12[pdat]).
Embase
(“acupuncture”/exp OR “biofeedback”/exp OR ‘alternative medicine’/exp OR ‘hypnosis’/de OR “massage”/exp OR “meditation”/exp OR “Tai Chi”/syn OR (alternative-medicine OR biofeedback OR complementary-medicine OR complementary-therap* OR integrative-health OR massage* OR acupuncture OR yoga OR meditation OR hypnosis OR guided-imagery OR tai-chi OR tai-ji OR qi-gong OR qigong):ab,ti,kw) AND (“pain”/exp OR pain:ab,ti,kw) AND (“military phenomena”/exp OR (active-duty OR air-force OR airmen* OR armed-forces OR armed-services OR army OR guardian* OR marine-corps* OR marines OR military OR navy OR sailor* OR servicemember* OR service-member* OR soldier* OR space-force*):ab,ti,kw) AND [english]/lim AND [2014–2024]/py AND ([article]/lim OR [article in press]/lim OR [review]/lim).
Ovid All EBM Reviews (Cochrane)
(alternative-medicine OR biofeedback OR complementary-medicine OR complementary-therap* OR integrative-health OR massage* OR acupuncture OR yoga OR meditation OR hypnosis OR guided-imagery OR tai-chi OR tai-ji OR qi-gong OR qigong).ab,ti. AND pain.ab,ti. AND (active-duty OR air-force OR airmen* OR armed-forces OR armed-services OR army OR guardian* OR marine-corps* OR marines OR military OR navy OR sailor* OR servicemember* OR service-member* OR soldier* OR space-force*).ab,ti. AND english.lg.
1. limit 1 to yr=“2014–2024”
Inclusion/exclusion criteria
English language studies from any country with all types of study designs were included in the search. Articles from nonpeer-reviewed sources, abstracts from conference proceedings, and other non-scholarly sources were excluded. Articles were considered for final inclusion if they described or studied acupuncture, biofeedback, hypnosis, massage therapy, meditation, guided imagery, Tai Chi/Qi Gong, and yoga for pain management within the U.S. MHS. Although battlefield acupuncture is a specific auricular protocol, it was included under the umbrella of acupuncture for the purpose of this review. Forms of manual therapy were included in the reported studies of massage therapy as they met the initial search criteria, although the focus of this review was to include massage therapy as a distinct treatment modality.
Methods of review
All authors except one who performed the search, participated in abstract and title screening, full-text screening, and data extraction performed in Covidence and were blinded to other reviewers’ decisions. Duplicate studies were removed by Covidence and manually prior to screening. For abstract and title screening, each abstract was reviewed by two reviewers; disagreements were resolved by a third reviewer. Articles determined to meet inclusion criteria from preliminary abstract review were then reviewed by two independent reviewers based on the article full text; reviewers were required to agree on the reason for exclusion for any full-text article excluded. Discrepancies among reviewers were resolved by a third (blinded) reviewer.
Data extraction for articles selected as meeting inclusion criteria based on full-text review was performed by one of the authors for the following elements: General Information: study title, lead author, and publication year; Methodology: study aim, study focus (efficacy/effectiveness, utilization, other), study design, intervention/CIH modality, intervention details and comparator, outcome(s) (pain, post-traumatic stress disorder, traumatic brain injury, other), and outcome measurement frequency; Participants: population description, number of participants, and setting; and Findings and Conclusions. Final data extraction information in Covidence was exported as .csv files and saved as Excel files. Following data extraction, all studies were grouped based on Efficacy/Effectiveness, Utilization, or Other. Within these groups, studies were stratified by CIH modality. Results of the Data Extraction are presented by CIH modality by Efficacy/Effectiveness, Utilization, or Other study focus. Quality scoring was not performed as the articles reviewed were not homogenous and it was not the objective of the review.
Results
Search and screening
The number of studies resulting from each database search, abstract/title screening, and full-text screening are presented in the PRISMA 16 flow chart in Figure 1 and detailed below.
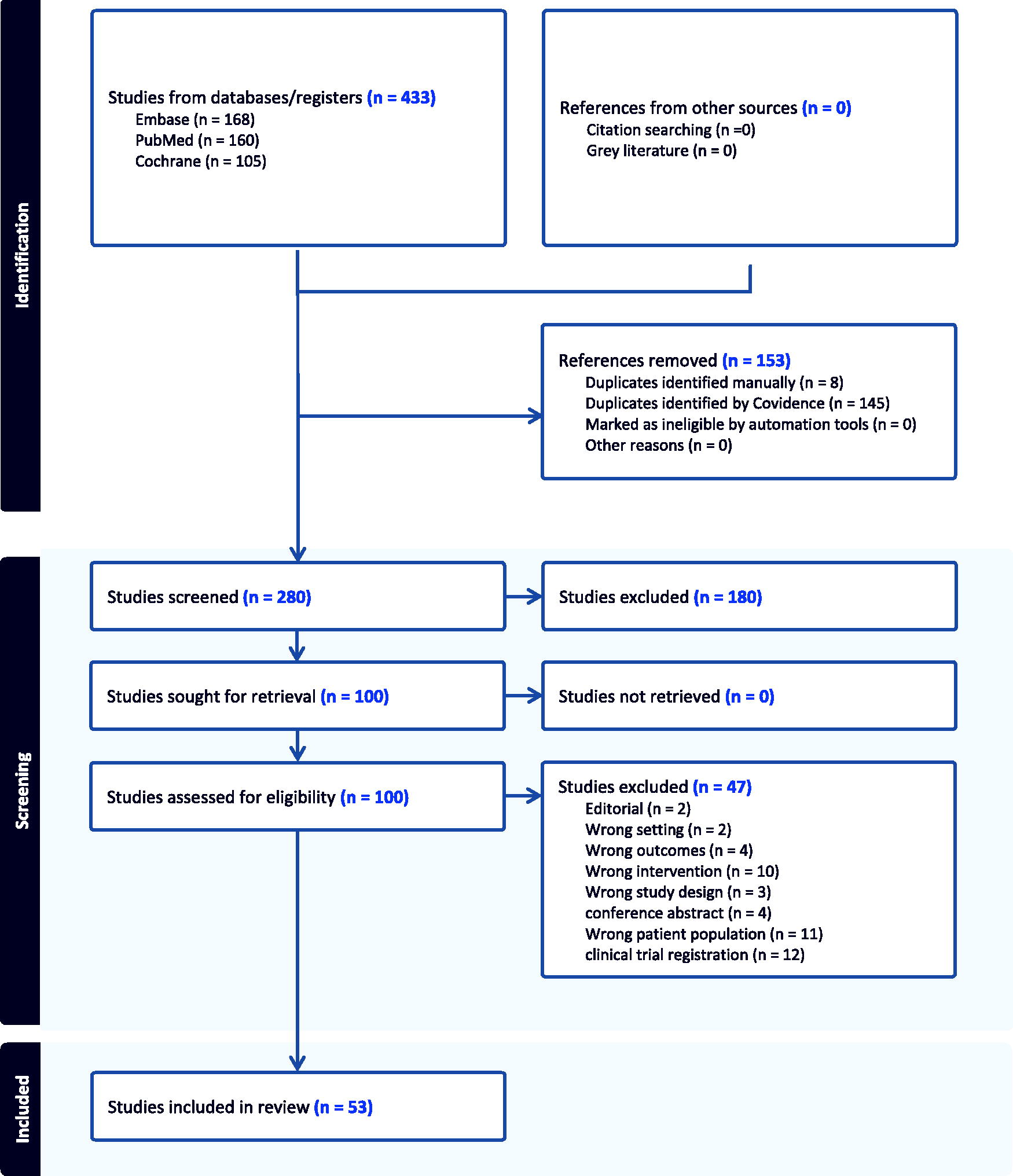
Study identification and screening.
Search results
The total number of studies resulting from the databases search was n = 433 (Embase, n = 168; PubMed, n = 160; Ovid/Cochrane, n = 105). Of these studies, 153 references were removed; 145 by Covidence; 8 manually.
Abstract and full-text screening
A total of 280 study abstracts were screened and 180 were excluded, leaving 100 for full-text review. Forty-seven were then excluded for the following reasons: editorial (n = 2), wrong setting (n = 2), wrong outcomes (n = 4), wrong intervention (n = 10), wrong study design (n = 3), conference abstract (n = 4), wrong patient population (n = 11), or clinical trial registration (n = 12). The total number of studies included in the review was n = 53. Average inter-rater reliability for abstract and full-text screening were 0.71 (range 0.52–0.85) and 0.73 (range 0.66–0.81) respectively, demonstrating substantial agreement among reviewers. No results were found for Qi Gong, Tai Chi, and hypnosis.
Data extraction
Results of the data extraction by CIH modality within Efficacy/Effectiveness or Utilization study focus are summarized in Tables 1–2 and reported below.
Efficacy/Effectiveness Studies (n = 36) of (a) Acupuncture, (b) Biofeedback, (c) Guided Meditation, (d) Massage Therapy, (e) Yoga, and (f) General Complementary and Integrative Health/Multiple Modalitiesa
Efficacy/effectiveness (Table 1)
Thirty-six of the 53 articles included in the review (68%) assessed efficacy/effectiveness of CIH modalities; 15 for acupuncture, 3 for biofeedback, 3 for guided meditation, 2 for massage therapy, 4 for yoga, and 8 for general CIH/multi-modality. Hypnosis and Tai Chi/Qi Gong were not assessed for efficacy/effectiveness by the studies under review in our sample.
Acupuncture
The studies reviewed demonstrate diverse applications and effectiveness of acupuncture for pain management in the military context. Engel et al. (2014) found that active-duty military personnel with post-traumatic stress disorder experienced significant improvements in pain severity, symptoms, and depression with acupuncture compared with usual care. 17 Moss and Crawford (2015) reported that battlefield acupuncture significantly reduced sore throat pain in DoD beneficiaries with effects sustained up to 24 h post-treatment. 18 Bell and Falconi (2016) reported acupuncture showed low to moderate effectiveness in managing lower back pain and osteoarthritis in deployed environments, suggesting feasibility in austere settings. 19 Guthrie et al. (2016) demonstrated that a combined battlefield acupuncture and dry needling intervention reduced chronic neck pain significantly. 20
Studies on traumatic brain injury and headache management (Jonas et al., 2016) and general pain reduction in military populations (Crawford et al., 2017) supported acupuncture’s role in reducing symptom severity and medication use. 21,22 Garner et al. (2018) confirmed that auricular acupuncture reduced pain and insomnia in military beneficiaries. 23 However, Crawford et al. (2019) observed that modified battlefield acupuncture did not yield significant benefits for pain management postsurgery. 24
Case studies by Hawks (2017) and Riegleman et al. (2021) highlighted successful pain reduction and functional improvement with battlefield acupuncture in patients with Achilles tendinopathy and medial tibial stress syndrome, respectively. 25,26 Kim et al. (2022) supported battlefield acupuncture’s effectiveness as an adjunct for immediate pain relief. 27 Recent randomized controlled trials found that acupuncture combined with home exercises significantly reduced pain in plantar fasciopathy. 28,29
Biofeedback
Studies on biofeedback interventions demonstrate promising outcomes for managing chronic pain and post-traumatic headache within military populations. Baker et al. (2018) investigated a multidisciplinary approach involving biofeedback, guided imagery, meditation, mindfulness, and cognitive behavior therapy to address medication-refractory post-traumatic headache among active-duty personnel and observed a 36% reduction in headache frequency, a 56% decrease in headache severity, improved quality of life for 60% of participants, polypharmacy rates declined by 24%, and annual appointment frequency for migraines decreased significantly. 30 A randomized controlled trial comparing biofeedback, traditional Chinese acupuncture, and transcutaneous electrical nerve stimulation for chronic pain relief in military service members showed that all three interventions resulted in significant reductions in chronic pain and functional disability over 6 weeks. 31
Guided meditation
Studies on guided meditation and mindfulness-based interventions reveal potential for managing chronic pain and improving mental health among military populations. A case study on an active-duty Marine participating in a mindfulness-based meditation program, which included guided imagery and mindfulness sessions, demonstrated mild improvements in pain, sleep quality, and mental health postintervention, with more substantial improvements observed at 4- and 7-month follow-ups. 32 Khusid et al. (2016) conducted a systematic review of 72 studies, encompassing active-duty, veteran, and civilian populations, to evaluate mindfulness-based interventions for chronic pain, substance misuse, and insomnia; their findings indicated that mindfulness-based interventions effectively reduced pain intensity, improved functional status and quality of life, alleviated psychological impacts related to chronic pain, and showed potential for reducing opioid cravings and misuse. 33 Stoerkel et al. (2018) assessed the efficacy of a self-care toolkit containing guided meditation audio files and acupressure bands for breast cancer surgery patients at two Army medical centers and showed that the toolkit group reported lower pain interference, fatigue, and postoperative pain scores, as well as reduced inflammatory responses. 34 In a randomized trial, Crisp et al. (2023) evaluated mindfulness-based stress reduction for chronic pelvic pain among active-duty women, with results showing reductions in both pain and depression symptoms. 35
Massage therapy
The studies on massage therapy within military populations indicate beneficial effects for pain management and symptom relief. Davis et al. (2015) examined the effects of Light Touch Manual Therapy on active-duty soldiers with chronic post-traumatic stress disorder and head injury, noting significant reductions in headache severity and anxiety immediately after each session with decreased pain interference sustained several days post-treatment. 36 Kern et al. (2018) conducted a prospective observational study to assess the feasibility and effectiveness of reflexology for chronic pain management in a military pain clinic and found soldiers receiving 25-min reflexology sessions alongside their standard pain management therapies reported a decrease in pain. 37
Yoga
Studies on yoga and mindfulness interventions revealed positive impacts on pain management, mental health, and overall physical resilience among military personnel. Combs et al. (2018) conducted a pilot study integrating a group-based yoga and mindfulness program into military brain injury rehabilitation, finding moderate improvements in health, pain, sleep, and mood at 4 months, with effects sustained at 7 months, although some results were potentially influenced by concurrent neurostimulator treatment. 38 Highland et al. (2018) explored the feasibility of an individualized yoga program for chronic low back pain in service members through a randomized controlled trial; participants showed reductions in pain intensity and disability over the 8-week program, with long-term follow-up supporting sustained benefits. 39 Groessl et al. (2022) compared hatha and restorative yoga types in active-duty personnel with chronic back and neck pain: both led to moderate reductions in pain-related disability, pain severity, and improvements in quality of life, grip strength, and balance. 40
Smith et al. (2023) conducted a large-scale group randomized controlled trial with 1584 military trainees to assess the combined impact of mindfulness training and yoga on injury resilience during basic combat training, trainees in the intervention group reported better health, less pain-related impairment, and improved sleep, mood, and stress levels compared with controls. 41
General CIH/multi-modality
Studies on general CIH or multi-modality approaches for pain management in military populations report positive impacts, in the form of reduced pain scores and improved subjective quality of life. Clifford et al. (2014) reviewed pain management advancements over a decade, highlighting the Army Surgeon General’s recommendation to increase CIH as an adjunct to pharmaceutical treatments, with promising potential for managing chronic pain in wounded service members. 42 Similarly, Jonas et al. (2015) discussed how CIH approaches, including whole-person healing, are essential for addressing the war-related trauma spectrum response. 43
Flynn et al. (2017, 2022) described protocols for evaluating CIH modalities such as acupuncture, biofeedback, massage therapy, and yoga in pain management programs. 44,45 These studies noted logistical challenges in implementing CIH but showed that service members receiving CIH combined with standard rehabilitative care reported greater pain reduction and functional improvement, particularly for those with high baseline pain levels. 44,45
Meerwijk et al. (2019) analyzed the health records of service members with chronic pain, finding that those who received nonpharmacological treatments had significantly lower risk of adverse outcomes, such as substance use disorders and suicidal ideation, upon transitioning to the VHA. 46 Nguyen et al. (2020) further supported the benefits of structured CIH programs, reporting improvements in physical strength, endurance, and reduced fear of movement among Army personnel in a functional restoration program. 47
Donahue et al. (2021) conducted a systematic review and meta-analysis, confirming the effectiveness of CIH in reducing pain intensity and improving physical functioning in military populations. 48 Eaton et al. (2022) examined the role of psychological factors in pain management outcomes, finding that while psychological aspects related to pain improved, CIH therapies did not directly impact chronic pain outcomes through changes in psychological mediators. 49
Utilization (Table 2)
Eight of the 53 articles included in the review (15%) assessed utilization of CIH modalities: 3 for acupuncture), 1 for massage therapy, and 4 for general CIH/multi-modality. Yoga, hypnosis, and Tai Chi/Qi Gong were not assessed for utilization by the studies under review in our sample.
Utilization Studies (n = 8) of (a) Acupuncture, (b) Massage Therapy, and (c) General Complementary and Integrative Health/Multiple Modalities
No results were found for Qi Gong, Tai Chi, and hypnosis.
Acupuncture
The studies on acupuncture use in the military setting highlighted its applications for pain management and other health conditions. Niemtzow et al. (2015) reviewed the history and application of battlefield acupuncture within the U.S. military, suggesting that battlefield acupuncture be expanded to the North Atlantic Treaty Organization (NATO) medical communities as a primary or adjunct pain management modality, recommending its broader integration in MHSs worldwide. 50
Madsen et al. (2018) analyzed 15,761 patient records from the MHS to examine acupuncture utilization trends among TRICARE Prime-eligible beneficiaries and indicated that acupuncture was primarily used for pain management, with similar top diagnoses across active-duty and nonactive-duty groups. 51 In a separate study, Madsen et al. (2019) explored acupuncture use in pregnant patients within the MHS from 2006 to 2016, finding a growing trend in acupuncture visits among pregnant women, with the majority of sessions related to pain and pregnancy-associated conditions. 52
Massage therapy
Rhon et al. (2018) examined health care utilization outcomes over a 1-year period for patients with back or shoulder pain treated with manual therapy alone compared with those treated with both manual therapy and opioids within a military treatment facility setting, including 1876 active-duty, dependent, and retired military personnel, with 714 receiving only manual therapy and 1162 receiving a combination of manual therapy and opioids. 53
General CIH/multi-modality
The studies on CIH modalities within military settings revealed significant trends in usage, capacity, and the impact of nonpharmacological therapies on pain management and opioid use. Williams et al. (2016) examined 6 years of data across military treatment facilities and found a steady increase in the use of chiropractic/osteopathic manipulation, acupuncture, and biofeedback, particularly for managing back pain with nearly 15% of active-duty service members using these therapies during the surveillance period. 54 Madsen et al. (2017) conducted a narrative review summarizing the range of integrative medicine options within the MHS, including acupuncture, biofeedback, and massage therapy noting three key themes: the alignment of integrated medicine approaches with managing multifaceted conditions such as post-traumatic stress disorder and traumatic brain injury, a patient-driven demand for integrative medicine therapies, and increasing research supporting the effectiveness of these therapies. 55
Bolton et al. (2022) assessed the capacity and utilization of nonpharmacological therapies across MTFs, finding increased full-time equivalent positions for chiropractors, physical therapists, and behavioral health providers and linking the rise in nonpharmacological therapies usage to policy changes that improved access. 56
Nine of the 53 articles resulting from the search (17%) assessed something other than efficacy/effectiveness or utilization of CIH modalities and thus were not included in the summary of results.
Discussion
This scoping review demonstrates that there is a significant focus on evaluating the efficacy/effectiveness of CIH therapies within the MHS, with 68% of studies concentrating on effectiveness, particularly in acupuncture, yoga, and multimodal CIH approaches. Among these, acupuncture emerges as a predominant intervention for pain relief across both acute and chronic conditions. The research underscores battlefield acupuncture’s immediate efficacy in acute pain settings and suggests sustained benefits for managing chronic pain in military populations, consistent with the findings by Niemtzow et al. (2007) on battlefield acupuncture’s rapid application and pain-relieving effects in austere environments. 10
Yoga and mindfulness-based interventions appear effective for chronic pain, stress management, and enhancing physical resilience. Studies have shown these interventions provide long-term pain reduction and quality-of-life benefits. However, other CIH modalities such as hypnosis and Tai Chi/Qi Gong require further investigation prior to drawing a conclusion on their effectiveness.
Utilization studies show a steady increase in CIH use, yet disparities persist across military settings. Research highlights increasing adoption of acupuncture for diverse patient groups, including those with pregnancy-related symptoms (Madsen et al., 2019), 52 and indicates the potential for massage therapy to serve as a nonpharmacologic first-line treatment for musculoskeletal pain. Despite this growth, there remains a paucity of utilization studies on hypnosis, Tai Chi/Qi Gong, and yoga within the MHS. Understanding CIH utilization in the MHS provides valuable insights not only for improving care within the military but also for informing broader health care systems. The unique structure of the MHS, which integrates health care delivery with readiness and operational demands, offers a model for studying the scalability and implementation of CIH therapies in other large, complex health care systems.
Lastly, research focused on broader CIH adoption and educational support in MHS emphasizes the need for structural reforms to integrate CIH into standard military health care. Studies from the VA Health Services Research and Development (HSR&D) evidence maps support the potential benefits of these therapies but highlight the importance of addressing challenges in training and availability. 10 Despite evidence supporting the efficacy/effectiveness of CIH therapies such as acupuncture for pain management, their integration into military health care faces significant barriers. TRICARE does not cover these therapies in the purchased care system, limiting access to military treatment facilities, where availability varies widely by location. This inconsistency highlights the need for policy alignment to ensure equitable access to these effective, nonpharmacologic pain management options across the MHS.
This review has several limitations that should be considered when interpreting the findings. First, the reliance on published literature may not fully capture the breadth of CIH therapies implemented within the MHS, particularly at smaller or less-researched facilities. Second, variability in the availability and reporting of CIH therapies across military treatment facilities introduces potential gaps in understanding utilization trends and barriers. Third, this review used the VHA’s list of CIH therapies to guide the scope of analysis, which may not fully align with practices specific to the MHS.
Conclusion
This review highlights that some CIH therapies, particularly acupuncture, yoga, and massage therapy, have been demonstrated to appear to be effective nonpharmacologic options for pain management among military personnel. These findings align with evidence from the VHA, where CIH therapies have demonstrated efficacy/effectiveness in managing chronic pain and improving patient outcomes. However, unique aspects of the MHS population, such as the prevalence of combat-related injuries, acute operational stress, and younger demographics, may influence the patterns of utilization and effectiveness observed. For example, while acupuncture has been widely adopted in the VHA for chronic pain, its implementation in the MHS has focused more on protocols such as battlefield acupuncture for pain relief in operational environments.
As CIH utilization grows within the MHS, these findings support further efforts to standardize CIH practices, enhance access, and provide structural support for implementing these therapies across the MHS. Expanding research on underutilized CIH modalities and ensuring training for health care providers are essential to fully leverage the potential of CIH in improving the health and resilience of service members and veterans.
Registration of protocol
PROSPERO 2024 CRD4202453685, 29 April 2024, https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42024536853
Footnotes
Authors’ Contributions
A.K.C.: Conceptualization (supporting); title, abstract and full text review (supporting); writing—review (supporting). E.T.: Conceptualization (supporting); title, abstract and full text review (supporting); data extraction (supporting); writing—review and editing (supporting). A.G.B.: Conceptualization (supporting); title, abstract and full text review (supporting); data extraction (supporting); writing—review (supporting); K.M.E.: Conceptualization (supporting); title, abstract and full text review (supporting); writing—review and editing (supporting); T.J.P.: Conceptualization (supporting); title, abstract and full text review (supporting); writing—review and editing (supporting); R.J.A.: Methodology (lead); Search (lead); writing—review and editing (supporting). T.L.R.: Conceptualization (lead); writing—original draft (lead); title, abstract and full text review (lead); data extraction (lead).
Disclaimer
The opinions and assertions expressed herein are those of the author(s) and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences, the Department of Defense, or the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.