
Abstract
Aim:
This study was conducted to evaluate the effect of laughter yoga on blood glucose levels, disease perception, and perceived stress levels in patients with type 2 diabetes.
Methods:
The research is a randomized controlled trial with pretest–post-test control group. The population of the study was followed up with the diagnosis of type 2 diabetes mellitus (T2DM) in the endocrine outpatient clinics of a hospital in the western region of Turkey. The sample consisted of 100 patients (laughter yoga group = 50, control group = 50) determined by power analysis. Participants were assigned to each group through a process of simple randomization. Those in the laughter yoga group (LYG) participated in online eight laughter yoga sessions together with a diet program. The following statistical methods were used to evaluate data: percentage, mean and standard deviation, chi-square, independent-sample t test, and paired sample t test. Data collection was facilitated using a “Patient Identification Form,” “The Brief Disease Perception Scale,” and “The Perceived Stress Scale.”
Results:
It was determined that the descriptive characteristics of the patients in the experimental and control groups were similar. According to the primary outcome, the postprandial blood glucose level of the patients in the LYG was (mean ± standard deviation [SD]: 98.17 ± 18.71) in the pretest; it decreased to (mean ± SD: 75.15 ± 9.65) in the post-test, and this difference was statistically significant (p < 0.001, effect size d: 1.628). While the mean blood glucose level of the patients in the control group was (mean ± SD: 102.17 ± 16.50) in the pretest, it increased to (Mean ± SD: 139.08 ± 15.65) in the post-test and this difference was statistically significant (p < 0.001, effect size d: 2.295). While the mean score of the Brief Disease Perception Scale post-test was (mean ± SD: 33.50 ± 4.51) points in the experimental group, it was (mean ± SD: 53.70 ± 4.15) points in the control group and the difference between them was statistically significant (p < 0.001). It was determined that the Perceived Stress Scale post-test mean score was (mean ± SD: 21.50 ± 4.54) points in the experimental group and (mean ± SD: 32.70 ± 4.15) points in the control group, and the difference between the groups was statistically significant (p < 0.001). It was determined that the negative illness perceptions and stress levels of the patients who applied laughter yoga were significantly reduced.
Conclusion:
Laughter yoga was found to reduce postprandial blood glucose levels, improve disease perception, and reduce stress levels in patients with T2DM.
Introduction
“Diabetes mellitus (DM) is recognized as a chronic metabolic disorder marked by ongoing high blood sugar levels. This condition can stem from the body’s inability to produce enough insulin, a resistance to insulin’s effects in peripheral tissues, or a combination of both factors.” 1 The prolonged state of high blood sugar, together with other metabolic issues in individuals with DM, may lead to damage across various organs and systems, potentially causing numerous complications. Type 2 diabetes mellitus (T2DM), which constitutes approximately 90% of diabetes instances globally, is notably prevalent. 2 T2DM is characterized by a diminished effectiveness of insulin, a condition known as insulin resistance. Initially, the body compensates for this resistance by increasing insulin production to maintain blood sugar balance. However, over time, insulin production may decline, resulting in T2DM. 1 This form of diabetes not only heightens insulin resistance but also elevates the risk of death related to cardiovascular diseases. 3 In addition, emotional stress affects depression, poor glycemic control, and quality of life for patients. 4 For metabolic control in T2DM, a healthy diet, regular physical activity, monitoring of blood glucose, and regular use of prescribed medications are required. 5 Studies have shown that maintaining glycemic control is important in reducing diabetes-related complications. 6,7 However, it has been reported that approximately 40%–60% of individuals with T2DM worldwide fail to achieve glycemic control. 7 Since it is seen that current medical treatments are not sufficient to control blood glucose levels, it has been suggested that new complementary therapeutic approaches should be used. 8
The research investigated the healing effects of laughter yoga on individuals diagnosed with T2DM. Studies suggest that laughter can influence the regulation of genes associated with the activity of natural killer (NK) cells, enhancing immune function in diabetes patients. 9 Additionally, laughter has been found to impact vascular tone by influencing the renin–angiotensin system. 10 The release of endorphins and dopamine, along with a reduction in cortisol (the stress hormone), and an effect on cytokine production are physiological changes attributed to laughter. 9,10 Literature review reveals instances where laughter has led to decreased postmeal blood sugar levels and bettered the clinical outcomes in conditions such as inflammation, asthma, cancer, and heart disease, attributed to diminishing the physiological stress response. 2 –11 Furthermore, laughter is documented to lower stress and anxiety, elevate mood and self-esteem, foster self-compassion, enhance coping mechanisms, and boost pain tolerance. 12,13 Negative emotions such as anxiety, fear, and sadness are known to increase blood sugar levels. In contrast, positive emotions like laughter are reported to adjust the levels of neuroendocrine factors tied to negative emotions and modulate immune functions. 8
A brief literature analysis shows that laughter mostly has positive effects on health in studies on laughter. This study was conducted to evaluate the effect of laughter yoga on postprandial blood glucose level, disease perception, and perceived stress level in patients with T2DM.
The hypotheses of the study are given below: Laughter yoga is effective in decreasing postprandial blood glucose levels. Laughter yoga is effective in reducing the negative perception of illness. Laughter yoga is effective in reducing the level of perceived stress.
Materials and Methods
Design
The research is a randomized controlled trial with pretest–post-test control group (CG) (the clinical trial number is NCT06783608). The “CONSORT 2010 checklist of information to include when reporting a randomised trial” was used to check the randomized-controlled trial design. 14,15
Participants
The study population consisted of patients who were followed up with T2DM and who applied to the endocrine outpatient clinic of a hospital in western Turkey.
Eligibility criteria
Inclusion and exclusion criteria
Diagnosed with T2DM for at least 6 months, 18–65 years of age, able to use computers and/or mobile applications, have at least a primary education degree, and patients who were on oral antidiabetic drugs and who did not have any communication problems to participate in the study were included.
Patients using subcutaneous insulin, not attending all yoga sessions, patients with physical ailments (respiratory distress, persistent cough, vertigo, etc.) that prevent them from participating in laughter yoga sessions, patients who use drugs or apply another nonpharmacological method to reduce stress, and patients who did not want to participate in the study were not included in the study.
Elimination criteria
Patients who did not attend all yoga sessions were excluded from the study.
After evaluating the patients in terms of inclusion criteria, we assigned them to the groups. During the nutrition process, patients were trained to comply with the diet programs recommended by the hospital. Therefore, we aimed to minimize the differences in terms of nutrition. We also determined that there was no difference between the groups in terms of body mass index (BMI). We excluded patients who used a different nonpharmacological method (such as breathing exercise or physical exercise) to reduce stress. We minimized the differences between the groups. Thus, we made stronger inferences about the effectiveness of laughter yoga.
Interventions
Laughter yoga group
The researcher is certified as an International Leader of Laughter Yoga. As a nursing intervention, patients with T2DM were made to do laughter yoga by the researcher. The laughter yoga program was conducted online (Google Meet online) due to the ongoing COVID-19 pandemic at the time of the study. WhatsApp groups were created in order to facilitate communication with the patients in the experimental group and information was provided here. Before starting the application, the use of the Google Meet program was explained to the participants and/or their relatives. It was announced that it can be easily connected from a phone or computer.
Interviews were conducted with the patients in the experimental group in order to learn about their shyness towards laughter yoga or attitudes and behaviors that may be negative to therapy in the presence of a joint group, and it was explained that patients who did not want to participate in group therapy could also participate in the sessions individually. Groups were created for individuals who wanted to participate in individual or group therapy. The times and days of the sessions were organized and information was provided about the online platform to be used. Laughter yoga was applied to the experimental group for 4 weeks, 2 days a week, for eight sessions (each session duration is 30–45 min on average). Before and 2 h after breakfast, patients were asked to measure and record their blood glucose levels. It was explained to the patients that they should attend all yoga sessions. It was explained that patients who did not attend more than two sessions would be excluded from the study. WhatsApp groups were established to maintain communication about the start times of the sessions and the application process. All patients who participated in the yoga session groups were recorded by the first researcher. Blood glucose measurements were also confirmed by the first researcher when the sessions started.
The sessions were organized as follows: Monday–Thursday 10:00–10:45, Tuesday–Friday 10:00–10:45, Wednesday–Saturday 10:00–10:45. Participants participated in two sessions that were suitable for them within a week. A participant in a group was not allowed to change days in the following weeks. The sessions were conducted in single groups of 3 (2 groups), 5 (4 groups), or 10 (3 groups).
After the days and sessions were determined, the participants were informed about the practice of laughter yoga. Within the scope of this information, he was carefully informed to follow the diet program regularly, not to change it, not to skip any meal, or to take less or more calories than the recommended calorie amount. The diet forms provided were also written in detail on the daily diet program cards and the effect of compliance on blood glucose control was explained in detail. These diet programs are planned to be 1600 calories per day. A total of 1600 calories are arranged as 500 calories in the morning, 600 calories at noon, and 500 calories in the evening.
The days and times for yoga were not changed according to the group to which the patients belonged but were arranged in the morning. Breakfast time was set at 9:00 am, which is the time when most patients have their breakfast. First, the patients measured their blood glucose levels using their own glucometer device before breakfast and recorded them in the blood glucose level registration form. Immediately after the measurement, they had the 500-calorie breakfast they were given. 1 h after the session, the sessions started with a laughter yoga instructor. The sessions lasted between 30 min and 45 min, after the first session, each session was extended according to the patient’s request when 30 min were filled.
As a nursing intervention, eight sessions of the laughter yoga program were applied to the patients in the experimental group. Patients in both groups were asked to follow the same diet program in order to avoid differences in terms of diet and calorie intake between the patients in the experimental groups and CG. Thus, we only evaluated the effect of laughter yoga on blood glucose levels.
Practice laughter yoga
Laughter yoga sessions are structured to include initial warm-up activities such as clapping and bodily movements, followed by deep breathing exercises, engaging in child-like play, and various laughter exercises, including mimicking congratulatory and lion laughter, along with other forms of self-initiated laughter. While the initial three segments of the sessions typically remain consistent, the fourth segment features a variety of laughter exercises that can differ from one session to another (Table 1).
Laughter Yoga Practice Stages
Control group
Patients in the CG did not receive any intervention. Considering the duration of the laughter sessions, they were asked to measure their blood glucose levels two days a week before and 2 h after breakfast and record them on a blood glucose level registration form.
Data collection
The data were collected by the researcher himself from patients who applied to the endocrine policlinics of a training and research hospital located in a megacity in the west of Turkey between November and December 2022 and met the criteria for inclusion in the study. The patients included in the study were met by the policlinics and the purpose of the research was explained and their contact numbers were obtained. “Blood Glucose Level Registration Form” was given to the patients and they were informed about the measurement times. The ability of the patients to perform self-measurement of blood glucose was questioned. It was determined that there were no patients who had problems while measuring. Measurements were measured from fingertips by enzyme colorimetric assay using a blood glucose meter by the individuals themselves. Fasting blood glucose was measured before breakfast. Postprandial blood glucose was measured 2 h after breakfast. Patients in the experimental group participated in 30–45 min laughter yoga sessions 1 h after breakfast. Postprandial blood glucose was measured 2 h after breakfast. In the CG, postprandial blood glucose was measured 2 h after breakfast without any additional intervention. Measurements were performed at the same time in both groups to avoid any difference in measurement time between the groups. Pretest data were collected face-to-face in the hospital. Patients/family members were informed that post-test data would be collected online. Patients/family members were informed about the use of the online form. The data collection form was prepared from Google Forms. It was shared with patients/family members via WhatsApp.
LYG data collection
The data collection process was completed in three stages:
Stage 1: Pretest data were collected by applying the Patient Introduction Form, the Brief Disease Perception Scale (Brief Illness Perception Questionnaire or B-IPQ), and the Perceived Stress Scale (PSS) forms face-to-face with the participants in the experimental group.
Stage 2: Participants were asked to measure their blood glucose levels before and after each laughter yoga session and record the results on a blood glucose level registration form.
Stage 3: After the participants completed the laughter yoga sessions, the Patient Introduction Form, the B-IPQ, and the PSS forms were administered online four weeks later and post-test data were collected.
CG data collection
The data collection process was completed in three stages:
Stage 1: Pretest data were collected by administering the Patient Introduction Form, the B-IPQ, and the PSS forms face-to-face to participants in the CG.
Stage 2: Participants were asked to measure and record their blood glucose levels just before and 2 h after breakfast on a blood glucose level registration form.
Stage 3: Post-test data were collected by administering the Patient Introduction Form, the B-IPQ, and the PSS forms online four weeks later to participants who did not receive the intervention.
Data collection tools
Patient Description Form, B-IPQ, PSS, and Blood Glucose Level Record Form were used to collect data.
Patient Introduction Form
This form evaluates demographic and disease characteristics of patients such as age, gender, educational status, marital status, height, weight, BMI, employment status, duration of diagnosis, presence of additional diagnosed chronic diseases, complication status, and HbA1c level. 8,16,17
The Brief Disease Perception Scale (B-IPQ)
The B-IPQ, developed by Broadbent and colleagues, examines how individuals perceive their illness. 18 It comprises nine items. Each item investigates a different aspect of illness perception. Respondents are asked to rate each item on a scale from 0 to 10. The Turkish version of the B-IPQ was validated and deemed reliable by Karataş and others in 2017 for a study on patients with cancer. Cronbach’s α coefficient of the Turkish version was 0.71, which indicates internal consistency across the scale. 19 In the present study, Cronbach’s α was calculated to be 0.96, reflecting a high level of internal consistency.
The Perceived Stress Scale
The PSS was developed by Cohen, Kamarck, and Mermelstein. The Turkish validation and reliability of the scale was conducted by Eskin et al. 20,21 This tool includes 14 questions that assess individuals’ perception of stress in various scenarios in their lives. Using a 5-point Likert scale, responses range from 0 (never) to 4 (very often). The scale features seven items phrased positively whose scores are reversed and combined with the scores of the other items to calculate the overall stress score. During the process of validating and ensuring the reliability of this scale, it achieved a Cronbach’s α value of 0.84. 21 For this particular study, Cronbach’s α was recorded at 0.94.
Blood Glucose Level Registration Form
It is a form created by the researcher to record the blood glucose levels measured by patients on a chart.
Variables of the research
Dependent variable
Dependent variables include patients’ blood glucose value, disease perception, and perceived stress level.
Independent variable
The independent variable includes laughter yoga.
Control variables
Control variables include age, gender, marital status, education level, income status, BMI, presence of additional chronic diseases, duration of diagnosis, and complication.
Sample size
Power analysis was performed to determine the sample size of the study. G-Power v3.1.9.4 was used for power analysis and the minimum sample size required for each group was determined as 46 (95% confidence interval [CI], α = 0.05, Power [1-β err probe] = 0.90, d = 0.5) in the calculation made using t test in independent groups. According to Cohen’s effect size classification, the effect size was calculated to be medium (d = 0.5). Cohen classified effect sizes as small (d = 0.2), medium (d = 0.5), and large (d ≥ 0.8). According to Cohen, “a medium effect of 0.5 is visible to the naked eye of a careful observer.” 22 Due to the lack of prior studies directly investigating laughter yoga and blood glucose, we based our medium effect size assumption on Cohen’s recommendation, considering findings from comparable behavioral interventions. Considering the possible losses in the sample, it was planned to take six more patients to each group (LYG = 52, CG = 52). In the research process; two patients from the LYG (because they did not attend all the sessions) and two patients from the CG (because they did not want to fill in the post-test data) were removed from the study and the research was completed with 100 patients (50 LYG, 50 CG) (Fig. 1).
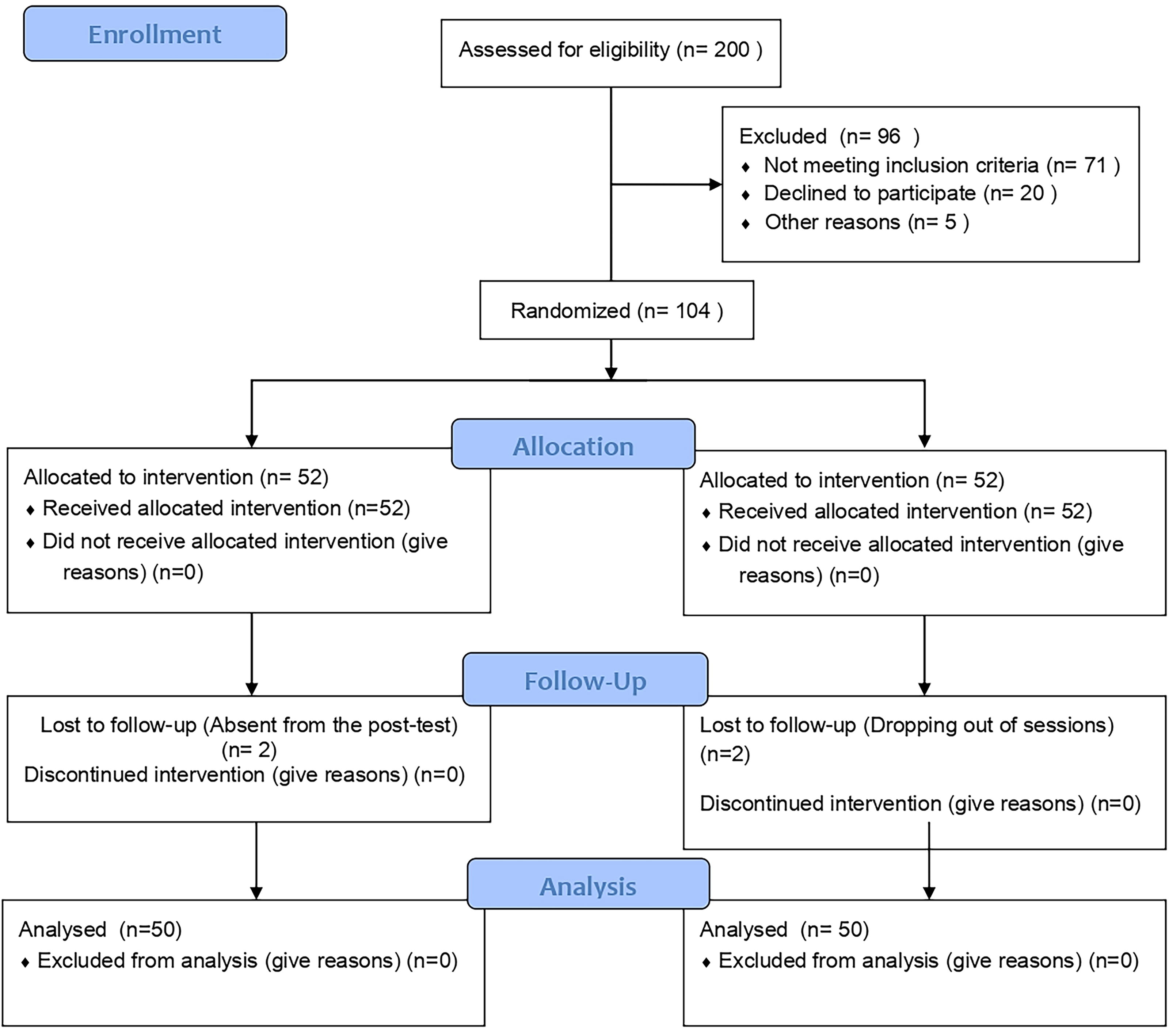
Consort diagram.
Randomization
In this study, simple randomization was performed to assign participants to experimental group and CG. A computer-aided randomization program (https://www.randomizer.org/) was used to determine who would be assigned to the groups; 104 patients were randomly divided into two groups (two sets of 52 numbers, numbers per set interval: numbered from 1 to 104) and were randomized. The sets determined for the impartial assignment of randomized patients to LYG and CG were placed in sealed envelopes. A lot was drawn by someone who was not involved in the research process and the people to be assigned to the LYG and CG were determined. Thus, the number of individuals in the groups was equalized with the probability of each patient involved in the study being in any of the experimental group or CG. Patients who applied to the endocrine outpatient clinic were selected according to the randomization lists and assigned to the experimental group and CG. Patients who applied to outpatient clinics were evaluated in terms of inclusion criteria and selected by a simple random sampling method.
Blinding
In the study, a randomization program was used to assign patients to the experimental group and CG randomly. Since the first researcher actively carried out the data collection process, the patients were assigned to the groups according to the numbers on the randomization lists. Pretest and post-test data were collected by the first researcher. Blinding could not be done in the data collection process. The second researcher did not participate in the data collection process. In order to prevent bias in data analysis, the second researcher entered the data into the SPSS program. In addition, the data recorded in the database were analyzed by a statistical expert independent of the researcher. The data were sent to the statistical expert by coding the groups as “Group X” and “Group Y” without clearly writing the names of the experimental group and CG.
Statistical analysis
The analysis of the data collected for this study was performed utilizing the free trial version of the SPSS Statistics (Statistical Package for Social Sciences) for Windows, version 26.0. To analyze the gathered data, descriptive statistical techniques were employed, including the calculation of frequencies, percentages, range (minimum–maximum values), mean, and standard deviation. The suitability of the data for normal distribution was examined through the creation of Q–Q Plots. Statistical methods used to evaluate data: chi-square and t tests were used to compare the control variables of the experimental group and CG, independent sample t test was used to compare the mean scores of the experimental group and CG, and paired sample t test was used for intragroup comparisons.
Identification of missing data
First, missing value ratios were calculated for each variable in the dataset, and it was determined that there were no missing data. This was done by calculating the rate of missing values for each variable.
If missing data had been identified, different strategies would have been applied depending on the type of data and missing rates.
If the missing values were small and were found to be missing completely at random, the missing observations would be excluded from the analysis.
If there is a significant proportion of missing data and they are considered to be missing not at random or missing at random, the multiple imputation method will be used. This method would complete the data by generating multiple estimates for each missing value, considering uncertainties.
Results
The findings obtained as a result of the research conducted on 50 LYG and 50 CG patients are as follows. Table 2 presents the demographic information of participants in both the LYG and CGs. The difference between the groups was not statistically significant when comparing the descriptive characteristics of the patients in the LYG and CG (p > 0.05). It is observed that the demographic characteristics of the patients in the experimental group and CG are similar (Table 2).
Demographic Variables of Patients
BMI, body mass index; SD, standard deviation; t, independent samples t test; χ2, chi-square test; X, mean.
According to Table 3, it was determined that there was no statistically significant difference between the groups of patients and pretest HbA1c levels (p > 0.05). However, a significant difference was found in the post-test HbA1c levels between the groups. The difference was statistically significant (p < 0.001). After the tests, 72% of the CG and 56% of the LYG had HbA1c levels within the 7.0–8.0. Significantly, a substantial number of participants in the LYG achieved controlled HbA1c levels post-test, as shown in Table 3.
Comparison of Pretest–Post-test Averages of Experimental and Control Group HbA1c Levels
p < 0.001.
Chi-square analysis.
n, number.
Bold value signifies p < 0.001.
According to Table 4, in intragroup comparisons, it was determined that the mean blood glucose level of the patients in the LYG decreased from 98.17 ± 18.71 in the pretest to 75.15 ± 9.65 in the post-test and this difference was statistically significant (p < 0.001, effect size d: 1.628). While the mean blood glucose value of the patients in the CG was 102.17 ± 16.50 in the pretest, it increased to 139.08 ± 15.65 in the post-test and this difference was statistically significant (p < 0.001, effect size d: 2.295). When comparing between groups, the fasting mean blood glucose level of the LYG was 98.17 ± 18.71, compared with 102.17 ± 16.50 for the CG. This result did not indicate a significant statistical difference in pretest levels between the two groups (p > 0.05). However, the postprandial blood glucose level in the LYG was 75.15 ± 9.65, which was significantly lower than the CG’s 139.08 ± 15.65. This finding indicated a statistically significant difference between the groups in post-test levels (p < 0.001, effect size d = 4.917) (Table 4).
Comparison of Experimental and Control Group Blood Glucose Level Pretest–Post-test Score Averages
Paired samples t test.
Independent samples t test.
p < 0.001, d: Effect size.
SD, standard deviation; X, mean.
Figure 2 illustrates the variation in blood glucose levels in the LYG before and after laughter yoga sessions. There was a notable reduction in both fasting and postprandial blood glucose levels (as shown in Fig. 2).

LYG group blood glucose level. LYG, laughter yoga group.
According to Table 5 in intragroup comparisons, it was determined that while the mean pretest B-IPQ score of the patients in the LYG was 56.42 ± 5.31, the mean post-test score decreased to 33.50 ± 4.51, and this difference was statistically significant (p < 0.001, effect size d: 4.652). While the pretest mean score of the patients in the CG was 54.18 ± 4.77, the post-test mean score decreased to 53.70 ± 4.15, but this difference was not statistically significant (p > 0.05).
Comparison of Patients’ Brief Disease Perception Scale (B-IPQ) Scores Intra- and Inter-Group
Paired samples t test.
Independent samples t test, p < 0.05.
SD, standard deviation; X, mean.
In intergroup comparisons, the mean pretest B-IPQ score of the patients in the LYG was 56.42 ± 5.31, while the mean B-IPQ score of the patients in the CG was 54.18 ± 4.77. It was determined that the mean pretest scores of the patients in the LYG and CG were similar and the difference was not statistically significant (p > 0.05). While the post-test mean score of the patients in the LYG was 33.50 ± 4.51, the post-test mean score of the patients in the CG was 53.70 ± 4.15 and the difference between them was statistically significant (p < 0.001, effect size d: 4.661) (Table 5). It was observed that the negative illness perceptions of the patients in the experimental group decreased significantly.
According to Table 6, in intragroup comparisons, it was determined that while the mean pretest PSS points of the patients in the LYG were 32.39 ± 4.08, the mean post-test points decreased to 21.50 ± 4.54, and this difference was statistically significant (p < 0.001, effect size d: 2.523). In the CG, while the mean pretest PSS point was 31.45 ± 4.12, the mean post-test point increased to 32.70 ± 4.15, but this difference was not statistically significant (p > 0.05).
Comparison of Patients’ Perceived Stress Scale Scores Intra- and Inter-Group
Paired samples t test.
Independent samples t test, p < 0.001.
SD, standard deviation; X, mean.
In intergroup comparisons, the mean pretest PSS point of the patients in the LYG was 32.39 ± 4.08, while the mean PSS point of the patients in the CG was 31.45 ± 4.12. The pretest mean scores of the patients in the LYG and CG were similar, and the difference was not statistically significant (p > 0.05). While the post-test mean PSS point of the patients in the LYG was 21.50 ± 4.54, the mean post-test point of the patients in the CG was 32.70 ± 4.15, and the difference between them was statistically significant (p <0.001, effect size d: 2.575) (Table 6). It was seen that the stress level perceived by the patients in the experimental group decreased significantly.
Discussion
DM ranks as a highly widespread metabolic disorder globally and can lead to substantial health and economic challenges. It demands ongoing medical monitoring, modifications in lifestyle, and consistent medication compliance. Negative emotional states, including anxiety, fear, and sadness, are recognized for elevating blood sugar levels in affected individuals. On the contrary, positive emotions, such as laughter, are understood to modify the neuroendocrine factors associated with negative emotional responses. 8,23
In this study, it was determined that the postprandial blood glucose level of the patients in the LYG was significantly lower than the CG after eight sessions. In addition, the blood glucose levels of the patients in the LYG who applied laughter yoga decreased significantly compared to the pretest values of the post-test results (p < 0.001). In the CG, the post-test blood glucose level increased significantly compared with the pretest results (p < 0.001). It has been determined that laughter yoga significantly reduces the increase in postprandial blood glucose levels. In support of this research finding, Hayashi et al. found that laughter significantly suppressed the increase in blood glucose 2 h after eating in patients with type 2 diabetes. It has been thought that this positive effect of laughter may be due to the fact that muscle movement accelerates the use of glucose or positive emotions affect the neuroendocrine system and suppress the rise in blood sugar. 3 In another study by Hayashi et al., determined that an average increase of 26 mg/dL in blood glucose level 2 h after a meal was suppressed and expression changes were observed in some genes in patients who were subjected to a laugh-inducing experience. 24 Again, Hayashi et al. strongly advocated for the incorporation of laughter therapy in diabetic patients, highlighting its advantageous impact in thwarting the progression of diabetic nephropathy, normalizing prorenin receptor gene expression, and reducing blood prorenin levels. 25 In addition, it has been stated that laughter may contribute to the improvement of glucose intolerance by modulating NK cell activity. 26 Cokolic et al., on the contrary, determined that in individuals with type 2 diabetes (regardless of whether they were taking medication for treatment), an intense 30-min session of laughter yoga significantly reduced blood glucose levels immediately after the session. They stated that laughter yoga is a much better option than watching a comedy movie about people with diabetes due to the intense yoga breathing and movements. 27 Hirosaki et al. and Ohira et al. also found that a 12-week laughter yoga program improved glycemic control and lowered HbA1c levels in individuals with type 2 diabetes. 8,28 This research finding supports the literature. It has been determined that negative emotions such as anxiety, fear, and sadness are factors that increase blood sugar in patients with diabetes; on the contrary, positive emotions such as laughter change the levels of neuroendocrine factors involved in negative emotions and modulate immune function. Especially in patients with T2DM, the effect of stress exacerbating hyperglycemia is very important. Stress usually leads to increased levels of cortisol, the body’s main stress hormone. Cortisol increases insulin resistance, making it difficult for cells to take up glucose. However, laughter improves mood and lowers cortisol levels by triggering the release of happiness hormones such as endorphins and dopamine. This process reduces insulin resistance and increases glucose uptake by cells, which helps control blood glucose levels. In addition, in laughter yoga, breathing exercises, hand-arm-running exercises, and various games increase energy expenditure, increase blood oxygenation, reduce stress, and facilitate the control of blood sugar levels. 3,4,6,8,9,13,24,28,29 In this study, it is thought that deep breathing and movement during laughter yoga sessions increase energy expenditure and feeling happy may be effective in reducing blood glucose levels by providing hormonal control.
In line with the studies in the literature and the results obtained from this study, it is seen that laughter yoga, which is one of the non-pharmacological methods, is effective in reducing blood glucose values in diabetic patients. Accordingly, “H1a: Laughter yoga is effective in decreasing postprandial blood glucose levels” hypothesis has been confirmed.
In this study, it was determined that the negative disease perceptions of the patients in the experimental group and CG were similar in the pretest, but the negative disease perception was significantly reduced in the patients who participated in yoga sessions in the post-test. In the literature, it has been observed that there is no study investigating the effect of laughter yoga on the perception of disease in individuals with diabetes. However, there are studies from different groups reporting that laughter yoga is efficacious in the management of diseases. Namazinia et al. observed that implementing a laughter yoga program within a hospital context significantly enhanced the quality of life related to health in patients with cancer receiving chemotherapy. 28 Similarly, research by Farifteh et al. revealed that laughter yoga lessened stress prior to chemotherapy sessions and elevated the health-related quality of life among patients with cancer. 30 Öztürk et al. found that an eight-session laughter yoga program applied to older adults reduced loneliness and increased resilience and quality of life. 29 According to Ko and Youn, laughter therapy can be used to improve overall quality of life and psychosocial behaviors. 31 In this study, it was thought that laughter yoga, which is one of the funny activities that increase positive psychological states in individuals with type 2 diabetes, may be effective in maintaining self-care behavior and reducing negative disease perceptions. The study found that negative perceptions of illness improved significantly.
In line with the results obtained from the current study, it was determined that laughter yoga, which is one of the nonpharmacological methods, is effective in reducing the negative perception of the disease in diabetic patients. Accordingly, “H1b: Laughter yoga is effective in reducing the perception of disease” hypothesis has been confirmed.
In this study, it was determined that the perceived stress levels of the patients in the experimental group and CG were similar in the pretest, but the stress level was significantly reduced in the patients who participated in yoga sessions in the post-test. When the literature is examined, many studies report that laughter is effective in reducing stress levels. 18,32,33 A biological explanation has been given for how laughter reduces stress and anxiety. It has been determined that laughter makes a person feel good by triggering the release of endorphins and reducing stress hormones. 16,34 It has been determined that laughter has stress-reducing effects by suppressing the bioactivities of epinephrine, cortisol, and 3,4-dihydrophenylacetic acid (a main dopamine catabolite). 35 Bressington et al. found that laughter yoga applied to patients with psychological problems reduced anxiety, stress, and depression. 32 In Şahin’s master’s thesis, it was determined that laughter yoga practiced in the postpartum period reduced women’s anxiety and stress levels. 36 Kheirandish et al. have determined that laughter yoga reduces stress and depression levels in patients with multiple sclerosis. 37 In all studies in the literature, it has been determined that laughter yoga is effective in reducing stress levels, and this research result supports the literature.
The studies in the literature and the findings obtained in this study indicate that laughter yoga is effective in lowering the perceived stress level in diabetic patients. As a result of this research, “H1c: The hypothesis that laughter yoga is effective in reducing the perceived stress level” has been confirmed.
Limitations and generalizability of the research
The fact that this study was conducted only on patients admitted to the endocrine outpatient clinic of a hospital is a limitation in terms of the generalizability of the results. In addition, due to concerns about the pandemic process, the online implementation of sessions is another limitation in terms of reducing face-to-face interaction. Another limitation of the study is that the first researcher was actively involved in the data collection process and could not be blinded.
However, the strength of the research is that there is no study in the literature evaluating the effect of laughter yoga on blood glucose value, disease perception, and perceived stress level in patients with T2DM and that this study was randomized and controlled.
Conclusion and Recommendations
As a result of this research, laughter yoga has been determined to reduce blood glucose levels, improve negative disease perception, and reduce perceived stress in patients with type 2 diabetes.
The following suggestions can be made for the long-term effects of this research result and clinical applications:
Long-term effects
Sustainable blood glucose control
The blood glucose-lowering effect of laughter yoga can help achieve long-term control when practiced consistently. In other words, with regular practice, it may help maintain stable blood glucose levels. However, to ensure the permanence of this effect, longer-term follow-up and research are needed.
Psycho-social recovery
Chronic diseases such as diabetes can negatively affect patients’ psychological states. It has been observed that laughter yoga reduces this impact. In the long term, reducing stress and improving the perception of the illness could lead to a better quality of life. These effects may also increase patient adherence to treatment.
Stress management and cardiovascular health
Since diabetes can negatively affect heart and vascular health in the long term, reducing stress can indirectly reduce the risk of heart disease. The positive effects of laughter yoga on stress and anxiety may be beneficial in preventing such long-term health issues.
Clinical applications
Integrated treatment models
The effectiveness of laughter yoga can be seen as an additional approach to treatment. In clinical settings, it may be beneficial to direct patients not only toward pharmacological treatments but also to alternative methods such as yoga to balance their physical and mental health. Managing stress levels, in particular, can improve the success of the treatment process.
Education and awareness
Both patients and health care professionals can benefit from educational programs on the benefits of non-pharmacological treatments like laughter yoga. By learning these techniques, patients and caregivers can improve their adherence to treatment.
Multidisciplinary approaches
Laughter yoga can be supported not only by nurses but by all health care professionals (dietitians, psychologists, and therapists). In clinical applications, treatments such as yoga and stress management can be integrated as part of a holistic treatment protocol.
Long-term follow-up programs
Broader and long-term clinical research can be conducted to observe the long-term effects of laughter yoga. These studies could provide clearer insights into the continuity of its effects and its impact on other health parameters.
Encouraging social participation of patients
Laughter yoga can be organized as group activities. This can help patients socialize, increase their motivation, and support each other during the treatment process. Social connections can contribute to psychological recovery and strengthen patient adherence to treatment.
These suggestions could be important steps in improving patients’ overall health and quality of life through the integration of laughter yoga into treatment processes.
Footnotes
Authors’ Contributions
A.A.: Conceptualization, data curation, investigation, methodology, resources, software, validation, visualization, writing—original draft, and writing—review and editing. H.A.: Conceptualization, formal analysis, investigation, methodology, resources, software, supervision, validation, visualization, writing—original draft, and writing—review and editing.
Ethical Consent
In order to conduct the research, ethical approval was obtained from the Scientific Research and Publication Ethics Committee of Inonu University (decision number: 2022/3978) and institutional permission was obtained from the Chief Physician of Istanbul Dr. Sadi Konuk Training and Research Hospital. Permission was obtained from the authors for the scales used in the research. The purpose of the research and the intended use of the results were explained. Written informed consent was obtained from the participants. Institutional permission was obtained from Dr. Sadi Konuk Training and Research Hospital. Permission was obtained from the authors for the scales used in the research. The purpose of the research and the use to which the results would be put were explained. Written informed consent was obtained from participants.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.