
Abstract
During chronic liver disease (CLD), angiogenesis participates in the fibrogenic process. Herein, we aimed at verifying the on-treatment kinetics of serum vascular endothelial growth factor (VEGF) and angiopoietin-2 (Ang-2) in hepatitis C virus (HCV) patients undergoing antiviral therapy. Forty-three HCV patients treated with pegylated-interferon/ribavirin and 26 controls were studied. Serum VEGF and Ang-2 were determined before treatment, at different time points during treatment, and at follow-up after treatment. Thirty and 13 patients were sustained virological responder (SVR) and No-SVR, respectively. Patients showed increased Ang-2 levels [504 (368–720) versus 449 (389–483) pg/mL, P < 0.05], and equivalent VEGF levels [271 (193–377) versus 274 (199–324) pg/mL, P = 0.6], with respect to controls. By univariate analysis, stage of fibrosis was associated with Ang-2 levels (odds ratio 4.25, P < 0.05). In SVR patients VEGF levels showed a progressive reduction (P < 0.05) but returned to pretherapy levels at follow-up, and Ang-2 levels showed an opposite progressive increase, being significantly reduced at follow-up (P < 0.01). No significant modifications in VEGF and Ang-2 levels were observed in No-SVR. We conclude that, in patients with HCV-CLD, Ang-2 serum levels are associated with fibrosis and reduced at follow-up in SVR patients. On-treatment, VEGF and Ang-2 serum levels undergo different-sided modifications only in SVR patients, possibly expressing the vascular remodeling occurring early after viral clearance.
P
Hepatic angiogenesis can be observed during chronic liver disease (CLD), and is thought to participate in the fibrogenic process (Medina and others 2004). Fibrotic tissue offers resistance to blood flow and to oxygen delivery, thus stimulating angiogenesis by the upregulation of hypoxia-inducible factors and the consequent induction of angiogenic cytokines, such as vascular endothelial growth factor (VEGF) and angiopoietin-2 (Ang-2) (Pugh and Ratcliffe 2003). The appearance of endothelial cells forming characteristic capillary structures has been demonstrated in inflamed portal tracts from patients with chronic HCV-related hepatitis (García-Monzón and others 1995), and these patients also present increased hepatic VEGF mRNA and protein levels (Shimoda and others 1999; Medina and others 2003). More recently, serum Ang-2 levels were found to be increased in patients with chronic HCV infection, and both VEGF and Ang-2 serum levels were reduced after antiviral treatment (Salcedo and others 2005). However, no data are available on the on-treatment kinetics of angiogenic cytokines during therapy for chronic HCV infection. Therefore, we aimed at verifying serum levels of VEGF and Ang-2 before treatment, at different time points during treatment, and after treatment, in HCV patients undergoing antiviral therapy, and compare the groups achieving or not achieving SVR.
Forty-three consecutive patients about to begin antiviral treatment for HCV-related chronic hepatitis and 26 age- and sex-matched controls free from liver disease were enrolled in the present study. All subjects gave written informed consent to take part in the study and the study protocol was approved by the University Ethics Committee. Exclusion criteria for both patients and controls were considered: infection with hepatitis B or human immunodeficiency viruses, liver decompensation, hepatocellular carcinoma, history of any kind of cancer within the previous 5 years, inflammatory bowel disease, and concurrent autoimmune diseases except for chronic thyroiditis. Patients with HCV-related chronic hepatitis underwent antiviral treatment with peg-interferon alpha-2b (Peg-Intron®; Shering-Plough, Kenilworth, NJ), 1.5 μg/kg, and ribavirin (Rebetol®; Shering-Plough), 1,000 mg in patients <75 kg and 1,200 mg in patients ≥75 kg, for 48 or 24 weeks for patients with genotypes 1 and 4 infection or patients with genotypes 2 and 3 infection, respectively. SVR was defined as serum HCV-RNA negativity 6 months after the completion of antiviral treatment, whereas patients not achieving this outcome were defined No-SVR. All patients were assessed weekly during the first month of treatment and monthly thereafter. When scheduled, patients underwent blood drawing for laboratory examinations (blood cell count, liver enzymes, and HCV-RNA), and serum aliquots were stored at −80°C for subsequent analysis. VEGF and Ang-2 were assayed using commercially available kits in serum aliquots taken the day of treatment beginning, after 1 and 3 months of treatment, at the end of treatment, and after 6 months from the end of treatment. VEGF was determined using the Quantikine Human VEGF Immunoassay (R&D, Inc., Minneapolis, MN), with a minimum level of detection of 5 pg/mL; Ang-2 was assayed by the Quantikine Human Ang-2 Immunoassay (R&D, Inc.), with a sensitivity of 8 pg/mL. Depending on the parametric or nonparametric distribution of the variable tested, data are expressed as mean values ± standard deviation, or median values and interquartile range (25%–75%). Student's t-test and Mann–Whitney U-test were used for parametric and nonparametric continuous variables, respectively, and χ 2-test for categorical variables. Differences in VEGF and Ang-2 levels at the different time points between the beginning and the end of treatment were analyzed by the Friedman test followed by the Wilcoxon test for post hoc analysis. SPSS software (version 17.00; SPSS, Inc., Chicago, IL) was used for statistical analyses.
Patients and controls were age- and sex-matched (48.8 ± 11.9 versus 46.4 ± 8.3 years, P = 0.3; M/F 21/22 versus 13/13, P = 0.9), while alanine aminotransferase (ALT) levels, as expected, were significantly higher in patients before antiviral treatment than in controls (91.6 ± 61.0 versus 16.8 ± 7.3 U/L, P < 0.001). Of the 43 HCV patients enrolled in the study, 30 patients were SVR and 13 patients were No-SVR to antiviral therapy. The high rate of SVR observed in this population should be attributed to the prevalence of patients with genotype 2 and 3 infection (23 out of 43), who are known to have more chances of therapeutic success (Zeuzem 2004). The main characteristics of HCV patients, according to treatment outcome, are reported in Table 1. Only viral genotype and the stage of fibrosis were significantly different between the SVR and No-SVR groups, with genotype 1 patients and patients with higher stages of fibrosis percentually more represented in the group not achieving SVR. Other factors well known to be associated with treatment outcome, mainly viral load, did not reach the statistical significance probably due to the limited sample.
According to Knodell and others (1981).
Abbreviations: ALT, alanine aminotransferase; HCV, hepatitis C virus; SVR, sustained virological responder.
Before treatment beginning, patients showed increased Ang-2 levels [504 (368–720) versus 449 (389–483) pg/mL, P < 0.05] and equivalent VEGF levels [271 (193–377) versus 274 (199–324) pg/mL, P = not significant], with respect to controls. Moreover, baseline Ang-2 levels were higher in No-SVR than in SVR patients [656 (433–872) versus 489 (365–423) pg/mL, P < 0.05)], whereas VEGF levels did not differ between No-SVR and SVR groups [249 (190–306) versus 325 (190–414), P = 0.2]. Between the variables tested in HCV patients (age, sex, viral load, ALT levels, viral genotype, histological grading, and staging), none was found to be associated with VEGF baseline levels (data not shown), and only histological staging (≤1 versus >1 according to the median value) was associated with Ang-2 baseline levels (odds ratio 4.25, confidence interval 95% 1.05–17.20, P < 0.05), by univariate logistic regression analysis.
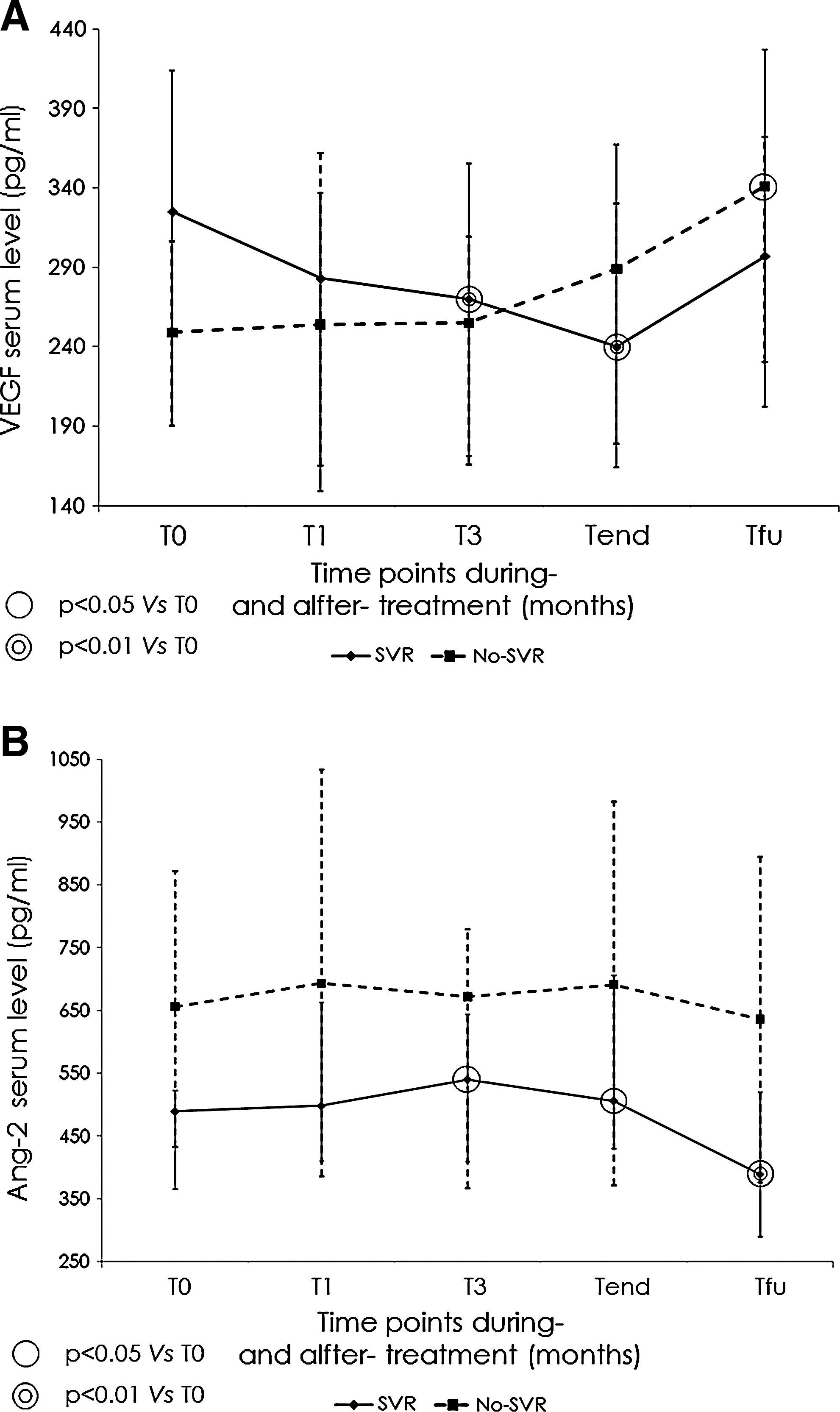
As shown in Fig. 1, during antiviral treatment, significant modifications in angiogenic cytokine levels were observed only in SVR patients. Indeed, in the SVR group, VEGF serum concentrations showed a progressive reduction, while returned to pretherapy levels at follow-up. In this same group, Ang-2 serum levels showed an opposite progressive increase during treatment, but dropped to concentrations lower than the baseline ones at follow-up. In No-SVR patients, no significant modifications in VEGF and Ang-2 serum levels were observed on treatment, and only VEGF concentrations were slightly elevated with respect to baseline at follow-up. Almost identical results were observed in the SVR group when it was reduced to 15 patients by excluding genotype 2 patients, not represented in the No-SVR group (data not shown).
VEGF
Consistent with previous studies (Janczewska-Kazek and others 2006; Salcedo and others 2005), our results confirm that serum VEGF levels are not different between HCV patients and controls, and that Ang-2 serum concentrations are significantly higher in HCV patients than in controls and reduced after treatment in patients achieving SVR, suggesting that Ang-2 may be more relevant than VEGF to the pathophysiology of this CLD. Moreover, Ang-2 serum levels were associated with the stages of fibrosis and increased in No-SVR with respect to SVR patients, in accordance with the observation that liver fibrosis was more advanced in the group of patients not achieving SVR. Differently from what observed by Salcedo and others (2005) in SVR patients, we did not observe a reduction in VEGF serum concentrations at follow-up after treatment. We think that our results are consistent with the lack of difference in baseline VEGF levels between HCV patients and controls, reported also by Salcedo and others (2005) suggesting that VEGF serum levels are not good as the Ang-2 ones as marker of angiogenesis/fibrosis.
Peg-interferon and ribavirin therapy induced different-sided modifications of VEGF and Ang-2 serum levels only in SVR patients. Indeed, on treatment, SVR patients showed a significant reduction in VEGF serum levels and an increase in serum Ang-2 concentration. These fluctuations, possibly expressing early vascular remodeling after viral clearance, are difficult to interpret and can be only object of speculations. It should be considered that, in the delicate equilibrium of cytokines and their relative concentrations regulating angiogenesis, Ang-2 has been shown to have a VEGF-dependent activity. Indeed, in vivo, in the presence of endogenous VEGF, Ang-2 efficiently induces increased blood vessel diameter, remodeling of the basal lamina, and endothelial cell proliferation, migration, and sprouting; when endogenous VEGF activity is reduced or inhibited, Ang-2 effectively promotes capillary regression, destabilizes blood vessels, and promotes plasticity (Eggert and others 2000; Etoh and others 2001; Lobov and others 2002). Therefore, our results could express that, in basal conditions Ang-2 plays a major role in the ongoing angiogenic process that supports the nascent fibrotic tissue; in the course of a successful antiviral treatment, when VEGF levels are concurrently reduced, Ang-2 participates in the early phase of capillary regression and vascular remodeling. Conversely, VEGF and Ang-2 serum levels did not show significant on-treatment modifications in No-SVR patients.
In conclusion, our study, the first to investigate serum VEGF and Ang-2 levels in the course of peg-interferon and ribavirin therapy for HCV-related chronic hepatitis, shows that these cytokines undergo significant modifications only in the group of patients achieving SVR, suggesting that complete viral clearance is required to alter the ongoing angiogenic processes. Moreover, our data confirm that serum Ang-2 levels are a better surrogate than serum VEGF concentrations of the angiogenesis/fibrosis progression characterizing chronic hepatitis C. These results need to be validated in a larger group of patients and possibly supported by analyzing hepatic VEGF and Ang-2 expression and localization in the course of antiviral treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.