
Abstract
Endothelin-1 (ET-1) increases in the ischemically induced ventricular fibrillation (VF) swine model of cardiac arrest and affects outcome by potentially attenuating the hemodynamic response to epinephrine. Fifty-one swine underwent percutaneous left anterior descending occlusion. Seven minutes postonset of ischemic VF, cardiopulmonary resuscitation (CPR) was initiated. If VF persisted after 3 shocks, 1 mg of epinephrine was given. ET-1 (collected at baseline and every 5 min until VF onset) was assayed with ELISA. Bayesian multivariate logistic regression analysis compared peak ET-1 levels with the binary outcome of a positive coronary perfusion pressure response of >20 mmHg following epinephrine. Sixteen animals (31%) failed to achieve a positive response. Restoration of spontaneous circulation (ROSC) was observed in 1/16 (6.3%) of epinephrine nonresponders and 20/35 (57.1%) of epinephrine responders (P=0.0006). The median peak ET-1 level was 2.71 pg/mL [interquartile range (IQR) 1.06–4.40] in nonresponders and 1.69 pg/mL (IQR 0.99–2.35) in responders. ET-1 levels were inversely associated with epinephrine response with a median posterior odds ratio (OR) of a coronary perfusion pressure response of 0.72 (95% confidence interval [CI] 0.48–1.06) for each one-unit increase in ET-1 and a probability that the associated OR is <1 of 0.95. Peak ET-1 levels predict a lack of a hemodynamic response to epinephrine during treatment of cardiac arrest during ischemic VF.
Introduction
A
Chest compressions are intended to provide vital organ perfusion during cardiac arrest and to facilitate resuscitation. Coronary perfusion pressure (CPP), defined as the pressure difference between aortic and right atrial pressure during the relaxation phase of rhythmic chest compression, has been shown to be a major determinant of myocardial perfusion and cardiac resuscitation outcome (Kern and others 2007). Epinephrine (adrenaline) and vasopressin are currently used in the cardiac arrest setting to increase peripheral arterial resistance, thereby increasing CPP and, by inference, the likelihood of restoration of spontaneous circulation (ROSC) (ECC Committee and others 2005). Despite the recognized benefit of vasopressors in the standard laboratory animal restoration model of cardiac arrest, the role of drug therapy in facilitating resuscitation and survival in the clinical population has been questioned (Ong and others 2007; Olasveengen and others 2009).
We recently reported that elevated endothelin-1 (ET-1) levels measured in the ischemically induced VF swine model of cardiac arrest were predictive of unsuccessful resuscitation (Shah and others 2009). ET-1, a potent vasoconstrictor, may adversely affect coronary arterial tone and myocardial perfusion during CPR, or facilitate the development of ischemic contracture. Previous work has demonstrated that ET-1 may attenuate the vascular response to phenylephrine in an in vitro endotoxic shock model (Scicluna and others 2008). The purpose of this study was to determine if ET-1 attenuates the hemodynamic response to epinephrine, thereby decreasing the likelihood of return of circulation during cardiac arrest and cardiopulmonary resuscitation.
Methods
This investigation was approved by the Animal Care and Utilization Review Committee of our institution and adheres to the American Physiological Society's Guiding Principles in the Care and Use of Animals and the Guide for the Care and Use of Laboratory Animals as stipulated by the U.S. National Institutes of Health.
Male mixed breed Yorkshire swine (n=51, mean weight 38±5 kg) were premedicated with ketamine (20 mg/kg) and xylazine (2 mg/kg). General anaesthesia was induced with isoflurane via nose cone and, after endotracheal intubation, maintained with inhaled isoflurane (MAC 1.0%–2.5%) and nitrous oxide in a 1:1 mixture with oxygen. End-tidal CO2 was continuously monitored and minute ventilation was adjusted to maintain end-tidal CO2 at 35–45 mmHg. Standard lead II of the surface ECG was monitored continuously during instrumentation and throughout the study protocol.
Instrumentation has been previously described in detail (Niemann and others 2007, 2009). In brief, micro-manometer-tipped catheters (Millar Instruments, Houston, TX) were positioned in the ascending aorta, left ventricle, and right atrium. A thermistor-tipped catheter for thermodilution cardiac output determinations was positioned in a branch of the pulmonary artery. Commercially available, standard adhesive defibrillation electrode patches were applied to the left and right lateral aspects of the shaved thorax. Transthoracic impedance was measured using a tetrapolar constant current impedance measuring system (THRIM®, Morro Bay, CA). A 30-ohm noninductive resistor was then placed in series with a truncated exponential biphasic defibrillation waveform defibrillator (LifePak 12; Medtronic Emergency Response Systems, Redmond, WA).
After instrumentation, heart rate, systolic and diastolic aortic pressure, left ventricle end-diastolic pressure, mean right atrium pressure, and cardiac output were recorded and arterial blood was analyzed (I-Stat EG7+; I-Stat Corp, Princeton, NJ). Hemodynamic data were recorded and stored on a laptop computer using PowerLab Chart v. 5.2 (ADInstruments, Colorado Springs, CO).
Using a 6 French guiding catheter inserted via a carotid artery or a femoral artery, an angioplasty catheter was positioned in the left anterior descending coronary artery distal to the first septal perforator. The balloon was then inflated to 8–10 atm. The site of coronary occlusion and confirmation of complete cessation of coronary flow distal to the balloon were confirmed with manual contrast injections.
Seven minutes after the occurrence of spontaneous, ischemic VF, closed-chest compressions were begun manually or with a mechanical device (Thumper™; Michigan Instruments, Grand Rapids, MI, or LUCAS™; Jolife AB, Lund, Sweden) at a rate of 100 compressions/min with force sufficient to depress the sternum 1.5–2.0 inches The occluding balloon remained inflated throughout resuscitative efforts. One minute after starting chest compressions, a transthoracic biphasic countershock at 200 J was given. For the purpose of these experiments, successful defibrillation was defined as termination of VF, regardless of the postshock cardiac rhythm or hemodynamic outcome, eg, spontaneous QRS complexes with or without associated arterial pressure pulses, determined 5 sec after a defibrillation shock. If asystole or pulseless electrical activity (PEA) followed the first shock, the second shock at 300 J, or the third shock at 360 J, 1 mg of epinephrine IV was administered. If VF persisted after the third shock, additional shocks at 360 J (monophasic shocks were substituted for the initial biphasic shock based on our prior experience) were delivered and 1 mg of epinephrine was given every 3–5 min. Chest compressions were performed between shocks and positive pressure ventilations (FiO2=1.00) were given at a rate of 8 ventilations/min. At the end of 15 min of advanced cardiac life support, animals remaining in VF, PEA, or asystole were considered resuscitation failures and resuscitative efforts terminated.
Restoration of spontaneous circulation (ROSC) was defined as an arterial systolic pressure >60 mmHg for >10 min. Pre-epinephrine CPR CPP (diastolic or relaxation phase aortic minus right atrial pressure) was determined by measuring the mean peak CPP over a minimum of 45 compression-relaxation cycles preceding epinephrine injection. The CPP response to epinephrine was measured over 20 cycles at the peak of the epinephrine response. The absolute change in CPP was measured and a CPP response after epinephrine of >20 mmHg was defined as a successful response to epinephrine (Reynolds and others 2010).
Before left anterior descending balloon inflation and at 5 min intervals until VF occurrence, blood was sampled from the right atrium, placed in sterile, chilled (0°C), EDTA-coated tubes, and centrifuged at 5,000 rpm for 10 min. Plasma was immediately separated and stored at −80°C until batch analysis. ET-1 concentrations were determined using commercially available kits for a quantitative sandwich ELISA highly sensitive and specific for porcine ET-1 (R&D Systems, Inc., Minneapolis, MN). Cross reactivity with ET-2, ET-3, and proendothelin is <0.05%.
Data were entered into an Excel Spreadsheet (v. 12.0, Microsoft Corp, Redmond, WA) and imported into SAS statistical software (v. 9.1; SAS Institute, Cary, NC) for analysis. Student's t-test was used to compare the means of normally distributed variables. Wilcoxon rank sum tests were used to test for differences in non-normal distributions. Fisher's exact test was used to compare proportions. Bayesian multivariate logistic regression was performed to evaluate the association between ET-1 levels and the outcome of epinephrine response. Specifically, the SAS procedure Proc Genmod with the logit link function and the Bayes option was used to model the log odds of an epinephrine response (defined a priori as achievement of a CPP of at least 20 mmHg) as a function of the peak plasma ET-1 level measured during the ischemic period preceding VF, controlling for chest compression type (manual versus Lucas® versus Thumper®) since the quality of chest compressions may influence CPP. The Bayesian approach allows the assignment of exact posterior probabilities to hypotheses regarding the association of interest. This analytic procedure uses Markov Chain-Monte Carlo (MCMC) methods to randomly sample from a user-defined prior probability distribution, as well as the likelihood distribution, derived from the current data, to arrive at a fully defined posterior probability distribution. Then, 5,000 sampling iterations were performed with the first 2,000 discarded as “burn-in” to avoid the influence of early, unstable samples. Noninformative or “flat” priors (lognormal distributions with mean 0 and standard deviation 8) were used in all analyses to model uncertainty regarding the location of the parameters of interest, namely, the coefficients of the 2 independent variables in the fitted model. Odds ratios (OR) are reported as median values with associated 95% credible intervals, the Bayesian analog of confidence intervals. We also report the posterior probability that the true OR lies above or below an OR of 1 (where unity suggests no association). Posterior autocorrelations and Geweke diagnostics, as well as visual inspection of trace plots were used to assure MCMC convergence.
Results
A total of 51 animals were in the analysis. Sixteen animals (31.4%) failed to achieve an epinephrine response of >20 mmHg and were classified as epinephrine nonresponders; the remaining animals achieved the target postepinephrine CPP value (n=35). Prearrest hemodynamic variables for epinephrine responders and nonresponders are shown in Table 1. Statistically significant differences between groups were not observed. Table 2 compares resuscitation variables between the 2 groups. ROSC was observed in 1/16 (6.3%) of nonresponders and 20/35 (57.1%) of responders (P=0.0006).
Values are reported as the mean and standard deviation.
Values are reported as the means and standard deviation.
The median peak ET-1 level was 2.71 pg/mL [interquartile range (IQR) 1.06–4.40) in nonresponders and 1.69 pg/mL (IQR 0.99–2.35) in responders. In univariate analysis an inverse relationship between ET-1 and epinephrine response was found such that a 1 pg/mL difference in peak ET-1 value was associated with an OR for an epinephrine response of 0.72 (95% confidence interval [CI] 0.50–1.05, P=0.08).
This association was consistent with results of Bayesian multivariate logistic regression, which controlled for type of CPR administered, and is given in Table 3. Inspection of trace plots and diagnostics demonstrated excellent convergence to a stationary posterior distribution for all coefficients. The posterior probability that the ET-1/epinephrine response OR was <1 was 0.95, suggesting that the measured inverse association is extremely likely.
ET-1, endothelin-1; OR, odds ratio. CPR, cardiopulmonary resuscitation.
Figure 1 displays the predicted probabilities of a CPP response to epinephrine during resuscitation from VF as a function of ET-1 level correlating an increase in ET-1 levels with a reduced CPP response to epinephrine.
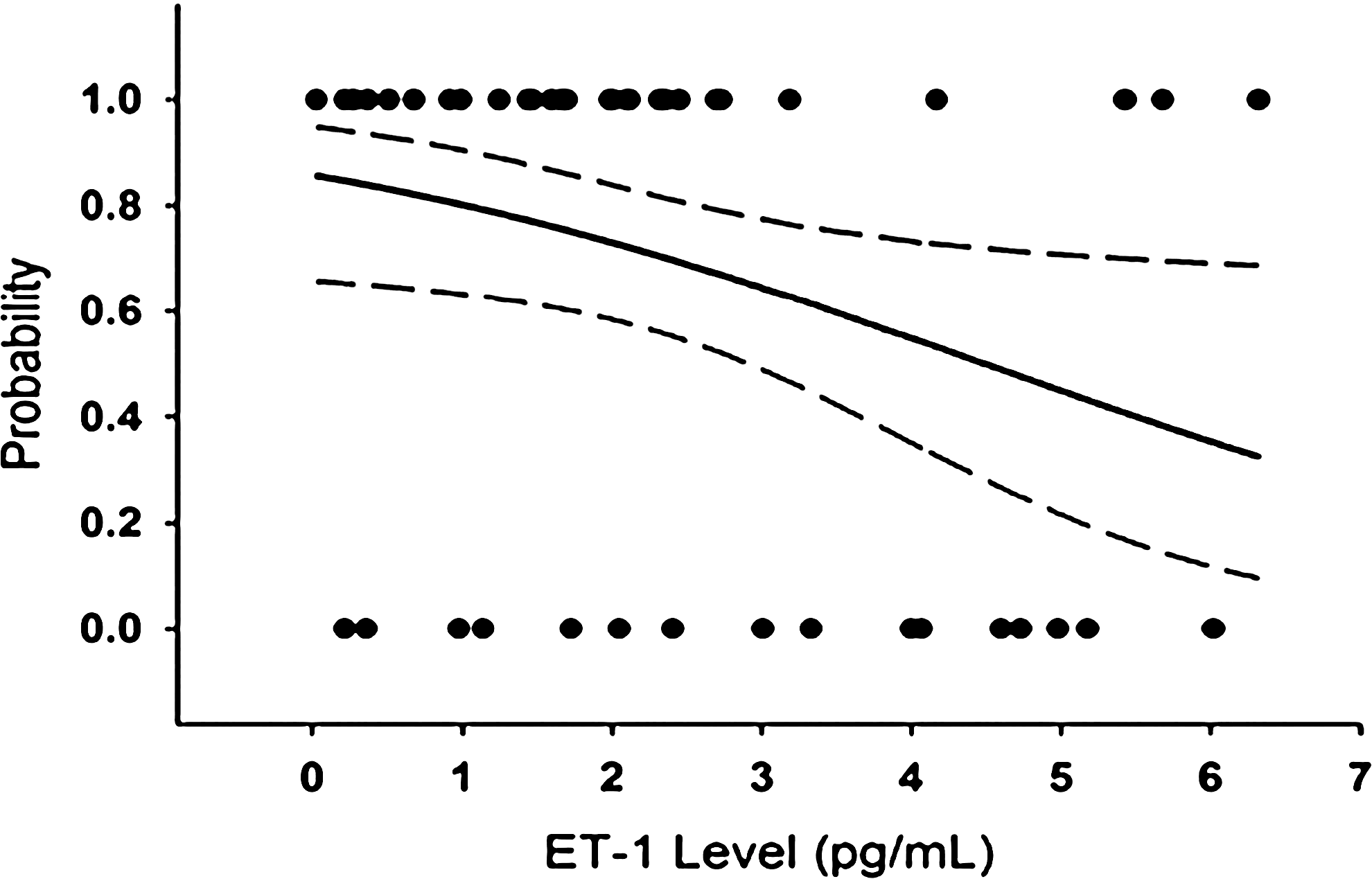
Predicted probabilities (solid line) and 95% confidence band (long dash) of a coronary perfusion pressure response to epinephrine during resuscitation from ventricular fibrillation as a function of endothelin-1 (ET-1) level. Actual outcomes are demonstrated by the superimposed scatter plot, where 1=a measured epinephrine response and 0=otherwise.
Discussion
This study demonstrates that an elevated peak level of endogenous ET-1 measured before the onset of spontaneous VF predicts attenuation of the response to administered epinephrine during resuscitation in a porcine ischemic cardiac arrest model. Prior studies have demonstrated that ET-1 may cause spasm of the middle cerebral, mesenteric, and coronary arteries and as well as attenuate the hemodynamic response to phenylephrine (Thorin and others 1998; Scicluna and others 2008). The findings of this study suggest that ET-1 may also block or attenuate the effect of epinephrine when administered during resuscitation and may account for differences in resuscitation outcome.
The ETs are 21 amino acid peptides produced by the endothelium and play an important role in cardiovascular physiology during acute myocardial ischemia. ET-1 reacts with membrane G-proteins resulting in peripheral vasoconstriction and increased inotropy and chronotropy (Brunner and others 2006). Vasoconstriction is mediated via a nonadrenergic mediated pathway resulting in an increase in intracellular calcium in vascular smooth muscle cells (Schmitz-Spanke and others 2000).
ET-1 increases during coronary occlusion and may play a role in arrhythmogenesis and myocardial dysfunction, as well as clinical outcomes (Pernow and Wang 1997; Cernacek and others 2003; Fink and others 2009). Elevated acute phase ET-1 levels portend a poor prognosis in patients with acute myocardial infarction due to an increased incidence of ventricular tachycardia, lowered systolic ejection fraction, cardiogenic shock, and cardiac death (Katayama and others 2005). Higher levels of ET-1 are known to reduce regional myocardial perfusion, due to the effects of ET-1 on coronary vascular resistance, and may contribute to early ischemic contracture by increasing cytosolic calcium concentration. Shock states lead to systemic hypotension through low vascular resistance as seen in septic shock, or decreased cardiac output as seen in cardiogenic shock, or due to hypovolemia in hemorrhagic shock. In these shock states, ET-1 levels are elevated and peripheral vascular resistance increases in an attempt to maintain perfusion to the brain and heart. While ET-1 is a potent vasoconstrictor and may confer some advantage to increasing peripheral resistance and increasing blood pressure, Magder has suggested that elevated of ET-1 may also have deleterious effects (Magder and Cernacek 2003). The increase in plasma ET-1 levels in our porcine model of abrupt and complete coronary occlusion mimic those observed in humans.
Few studies have addressed the potential role that the ETs, specifically ET-1, may have in cardiac arrest and resuscitation. Linder and associates were the first to report plasma ET levels during resuscitation of out-of-hospital cardiac arrest patients (Lindner and others 1996). Although ET levels, measured using a radioimmunoassay, were greater in nonsurvivors than survivors, both before and after administration of epinephrine, differences failed to achieve statistical significance in the small total sample size (n=26) of cases in which pre-epinephrine values were available. Although epinephrine is known to increase ET-1 concentrations (Alonso and Radowski 2003), this was not observed in their study and may be related to the timing of blood sampling. Haynes and others (1994) also observed insignificant differences in initial ET levels, measured using a radioimmunoassay, in survivors and nonsurvivors of out-of-hospital cardiac arrest. However, an increase in ET levels over time was seen in survivors. This group also had resuscitation initiated earlier than nonsurvivors, however. The timing and dosing of epinephrine during resuscitation and the time of return of spontaneous circulation with respect to blood sampling was, furthermore, unclear. Additionally, the definition of survival was not stated. Three studies have evaluated ET-1 as a pressor agent for the management of cardiac arrest (DeBehnke and others 1996; DeBehnke and Benson 2000; Hilwig and others 2000). Although ET-1 was shown to increase CPP, it did not improve regional myocardial perfusion during CPR and worsened 24 h survival when compared to epinephrine.
The findings of our study differ from those reported in the clinical population. This disparity is likely due to our study design and ET-1 sampling times, which were restricted to the pre-VF interval. Blood sampling ceased after the onset of VF and was not continued during the untreated VF period (7 min) or during resuscitation. Prior work suggests that epinephrine increases ET-1 concentrations (Alonso and others 2003) and measurements during or immediately after resuscitation would have been impacted by the therapeutic intervention. Additionally, our measurement method for ET-1, namely, a highly sensitive and specific ELISA for porcine ET-1, differs from the radioimmunoassay. A slightly higher rate of survival in this animal model may also be due to the controlled circumstances of the cardiac arrest, in direct contrast to the occasionally uncontrolled and variable presentation of cardiac arrest in the clinical setting.
In our study, the difference in the median peak ET-1 levels between the responders and the nonresponders was 1.02 pg/mL. Prior studies have shown that an increase in ET-1 of as little as 1.14 pg/mL (Steward and others 1992) is associated with worsening heart failure and that a rise of ET-1 of 2.19 pg/mL was associated with cardiogenic shock when compared to normal volunteers (Cernacek and others 1989).
Current clinical recommendations for the management of VF, as well as PEA and asystole, include the administration of 1 mg of intravenous epinephrine every 3–5 min during cardiopulmonary resuscitation (ECC Committee and others 2005). This recommendation is largely based on the results of laboratory studies that have demonstrated that epinephrine increases peripheral vascular tone via its α-1 adrenergic agonist effect, thereby raising aortic pressure and coronary artery perfusion during CPR. However, a recent observational report suggests that epinephrine does not improve the rate of return of spontaneous circulation, survival to hospital admission, or survival to hospital discharge (Ong and others 2007). A randomized trial suggests the same (Olasveengen and others 2009). The presence of an endogenous epinephrine inhibitor such as ET-1 might explain, in part, the marked difference in ROSC rates and survival when epinephrine is used in the animal laboratory versus the clinical setting. It might support the use of alternative vasopressor, eg, vasopressin, to increase CPP during CPR via a different signaling pathway. However, the relationship between ET-1 and other vasopressors remains unknown.
There are several limitations to our study. For one, there were multiple methods of chest compressions used in this study. Second, the use of a cutoff value of 20 mmHg to define a CPP response to epinephrine, while literature based, may not necessarily represent the ideal cutoff for statistical purposes. A more precise examination of the relationship between ET-1 levels and CPP response to epinephrine would involve timed sampling continued through the resuscitation period and would further elucidate any trends in the slope of the rate of rise in ET-1. Sampling during the postresuscitation period was not performed to evaluate ET-1 kinetics and the potential use of ET-1 as a biomarker for long-term survival. Finally, as there was a definite trend toward statistical significance, the inclusion of more subjects may further strengthen the conclusions of this article.
In conclusion, the peak ET-1 levels during acute myocardial ischemia in a porcine model will predict CPP response to epinephrine administered during resuscitation. This may represent an important mechanism for lack of response of many cardiac arrest patients to epinephrine during cardiopulmonary resuscitation.
Footnotes
Acknowledgment
This study was supported, in part, by a grant from the National Institutes of Health, NHLBI R01 HL076671.
Author Disclosure Statement
The authors have no relevant financial or personal conflicts of interests that could inappropriately influence the design or the findings of this study.