
Abstract
No data are available for chemokine (C-X-C motif) ligand 11 (CXCL11), together with CXCL10, circulating levels in autoimmune thyroiditis (AT). We measured serum CXCL11 and CXCL10 in 158 patients with newly diagnosed AT (26% with subclinical hypothyroidism), 56 euthyroid controls, and 20 patients with nontoxic multinodular goiter, all similar in gender distribution and age. CXCL11 was significantly higher in patients with AT (113±56 pg/mL) than in controls (67±16 pg/mL) or patients with multinodular goiter (75±18 pg/mL; P<0.0001). Among patients with AT, CXCL11 was significantly higher in those with a hypoechoic ultrasonographic pattern and hypothyroidism. In a multiple linear regression (MLR) model including age, thyroid volume, hypoechogenicity, hypervascularity, thyroid-stimulating hormone (TSH), and anti-thyroid peroxidase, age (P=0.009) and TSH (P<0.008) were significantly related to serum CXCL11. In an MLR model of CXCL11 (ln[pg/mL]) versus age, TSH, CXCL10 (ln[pg/mL]), TSH (P=0.028), and CXCL10 (P=0.003) were significantly and independently related to CXCL11. We first show that circulating CXCL11, together with CXCL10, is increased in patients with thyroiditis and hypothyroidism, and is related to CXCL10 levels. These results underline the importance of a Th1 immune attack in the initiation of AT.
Introduction
C
CXCL11 utilizes CXC chemokine receptor 3 (CXCR3) (Cole and others 1998; Cox and others 2001), a G protein-coupled receptor primarily expressed in activated T cells, yet also found in endothelial cells (Romagnani and others 2001). CXCL10 and CXCL9 also bind CXCR3, but with lower affinity (Cole and others 1998; Cox and others 2001) and less potency (Cole and others 1998) than CXCL11.
Among activated T cells, CXCR3 is more highly expressed in the Th1 subset (Bonecchi and others 1998). CXCL11 expression is strongly increased in response to interferon (IFN)-β or IFN-γ, and is presumed to be involved in pathologies characterized by the presence of activated T cells.
CXCL11 recruits activated Th1 lymphocytes to sites of inflammation
Recent evidence has shown that CXC α-chemokines (Th1), especially CXCL10, play an important role in the initial phases of autoimmune thyroid disorders. Patients with newly diagnosed autoimmune thyroiditis (AT) show increased serum CXCL10, in particular in the presence of a more aggressive thyroiditis and hypothyroidism (García-López and others 2001; Antonelli and others 2004, 2005).
Little is known about CXCL11 in the thyroid autoimmunity. Kimura and others (2004) analyzed C57BL6 transgenic mice that aberrantly express IFN-γ under control of the thyroglobulin promoter. They compared by reverse transcriptase PCR the thyroidal expression of 10 chemokines [chemokine (C-C motif) ligand 1 (CCL1) through 5 and CXCL9 through 13] in thyr-IFN-γ (that aberrantly express IFN-γ under control of the thyroglobulin promoter) transgenics and wild-type littermates. They found that transgenics exclusively expressed CCL4, CXCL9, and CXCL11, and showed increased expression of CCL5 and CXCL10 (Kimura and others 2004).
Further, we have recently shown that the secretion of CXCL9 and CXCL11 in primary cultures of human thyrocytes can be stimulated by IFN-γ and tumor necrosis factor (TNF)-α (Antonelli and others 2009, 2010b).
No study has evaluated CXCL11, together with CXCL10, circulating levels in thyroid autoimmunity. The aim of the current study, therefore, was to measure serum CXCL11 levels in patients with chronic AT, and to relate the findings to the clinical phenotype.
Materials and Methods
Patients
From the outpatient clinic, we selected 158 consecutive Caucasian patients with newly diagnosed chronic AT (Table 1). The patients were referred to us by general practitioners or other hospitals because of the presence of circulating thyroid autoantibodies or hypothyroidism, or clinical suspicion of a thyroid disorder. The diagnosis of AT was established from the clinical presentation (presence of a firm goiter, varying in size from small to very large, with a lobulated surface), thyroid hormones and thyroid autoantibodies measurements, and/or thyroid ultrasonography (decreased, dyshomogeneous echogenicity) (Antonelli and others 2004). The majority of these patients had a normal thyroid volume, some showed goiter (21%) or atrophic thyroiditis (12%). A minority of patients (9%) were submitted to fine-needle aspiration (FNA) to exclude the presence of thyroid cancer or lymphoma; in these cases, cytology confirmed the presence of a lymphocytic infiltration.
Serum TSH (μU/mL=mU/L)
P<0.02 versus controls.
P<0.05 or less versus controls and versus multinodular goiter.
AbTg, antithyroglobulin antibody; AbTPO, Antithyroperoxidase antibody; CXCL, chemokine (C-X-C motif) ligand; TSH, thyroid-stimulating hormone
Controls
Two control groups were used. The first control group (n=56) consisted of a random sample of the general population from the same geographic area in whom a complete thyroid work-up [history, physical examination, thyroid-stimulating hormone (TSH), free triiodothyronine (FT3), free thyroxine (FT4), antithyroglobulin antibody (AbTg) and antithyroperoxidase antibody (AbTPO) antibodies measurements, and ultrasonography] was available, and excluded the presence of thyroid disorders. A second control group comprised 20 patients with nontoxic multinodular goiter extracted from the same random sample of the general population. The majority of these patients had a normal thyroid volume, some showed goiter (40%). All these patients were submitted to FNA to exclude the presence of thyroid cancer; cytology confirmed the absence of a malignancy. In all patients and controls, a blood sample was collected in the morning, after overnight fasting, and serum was kept frozen until thyroid hormone, thyroid autoantibodies, CXCL10, and CXCL11 measurement.
Exclusion criteria for patients and controls
Exclusion criteria were as follows: (1) presence of anti-TSH receptor antibodies; (2) clinical history of hyperthyroidism; (3) concurrent endocrine or nonendocrine autoimmune diseases; (4) evidence of infectious diseases in the last 3 months; (5) treatment with drugs known to interfere with immune system (namely cytokines, IFN, corticosteroids, NSAIDs, amiodarone, and lithium); (6) pregnancy and lactation over the previous 6 months; and (7) presence of acute or chronic systemic diseases.
All study subjects gave their informed consent to the study, which was approved by the local ethics committee.
Ultrasonography of the neck and FNA
Neck ultrasonography was performed by the same operator, who was unaware of the results of thyroid hormones, autoantibodies, CXCL10, and CXCL11 measurements, using a probe (Esaote, Florence, Italy; AU5 with a sectorial 7.5 MHz transducer). Thyroid volume was calculated using the ellipsoid formula, as described (Antonelli and others 2004). The presence of hypoechoic and dyshomogeneous echogenicity was arbitrarily rated at 3 levels (0=normal echogenicity; 1=slight hypoechoic and dyshomogeneous; 2=severely hypoechoic and dyshomogeneous) to evaluate structural abnormalities of thyroid tissue associated with thyroid autoimmunity (Antonelli and others 2004). The presence of thyroid nodules was recorded, and nodules with a diameter >10 mm were submitted to ultrasonography-guided FNA, which was performed by the same operator, using a free-hand method as already described (Antonelli and others 2004).
Thyroid blood flow
Thyroid blood flow (TBF) by color-flow Doppler (CFD) was studied in all patients. The CFD pattern was defined as normal (or type 0), TBF limited to peripheral thyroid arteries; type I, TBF mildly increased; type II, TBF clearly increased; or type III, TBF markedly increased (Antonelli and others 2004). In patients with AT, TBF bore no relation to the thyroid status, and was type 0 in 58%, type I in 34%, type II in 8% of patients, whereas none had type III CFD pattern.
Laboratory evaluation
Thyroid function and thyroid autoantibodies were measured as previously described (Antonelli and others 2004). Circulating FT3 and FT4 were measured by commercial RIA kits (AMERLEX-MAB FT3/FT4 Kit; Amersham Biosciences, Little Chalfont, UK). Serum TSH (DiaSorin, Saluggia, Italy), AbTPO, and AbTg (ICN Pharmaceuticals, Costa Mesa, CA) were evaluated by immunoradiometric assay methods. For AbTg, AbTPO, positivity was set at >50 and >10 UI/mL, respectively.
Serum CXCL11 and CXCL10 ELISA
Serum CXCL11 levels were assayed by a quantitative sandwich immunoassay using a commercially available kit (R&D Systems, Inc., Minneapolis, MN), with a sensitivity ranging from 0.41 to 21.5 pg/mL and a mean minimum detectable dose of 11.9 pg/mL. The intra- and interassay coefficients of variation were 4.1% and 7.4%.
Serum CXCL10 levels were assayed by a quantitative sandwich immunoassay using a commercially available kit (R&D Systems), with a sensitivity ranging from 0.41 to 4.46 pg/mL and a mean minimum detectable dose of 1.67 pg/mL. The intra- and interassay coefficients of variation were 3.0% and 6.9%.
Data analysis
Values are given as mean±SD for normally distributed variables, otherwise as median and [interquartile range]. Mean group values were compared by using one-way analysis of variance for normally distributed variables (age and body mass index), otherwise by the Mann–Whitney U or Kruskal–Wallis test. Proportions were compared by the χ 2 test. Post hoc comparisons on normally distributed variables were carried out using the Bonferroni–Dunn test. Univariate and multivariate analysis were performed by multiple linear regression (MLR) analysis using CXCL11 or CXCL10 as dependent variables, and age, thyroid volume, TSH, AbTPO, hypoechoic pattern, and the presence of hypervascularity as covariates. Statistical power (ex post analysis) (stat-power) was calculated.
Results
The demographic and clinical features of patients and controls are reported in Table 1. The mean CXCL11 level was significantly higher in patients with thyroiditis, than in controls or patients with multinodular goiter, although some overlap was evident in the low range of CXCL11 values (Fig. 1) (stat-power=1). In patients with AT, serum CXCL11 levels (Table 2) were significantly higher in patients older than 50 years (123±71 versus 82±32 pg/mL, P=0.008), in patients with a hypoechoic pattern (156±77 versus 76±42 pg/mL, P=0.001), and in those with hypothyroidism (145±84 versus 103±45 pg/mL, P=0.001); whereas no significant difference was observed in relation to the presence of AbTPO positivity, AbTg positivity, the presence of hypervascularity, or thyroid volume (Table 2).
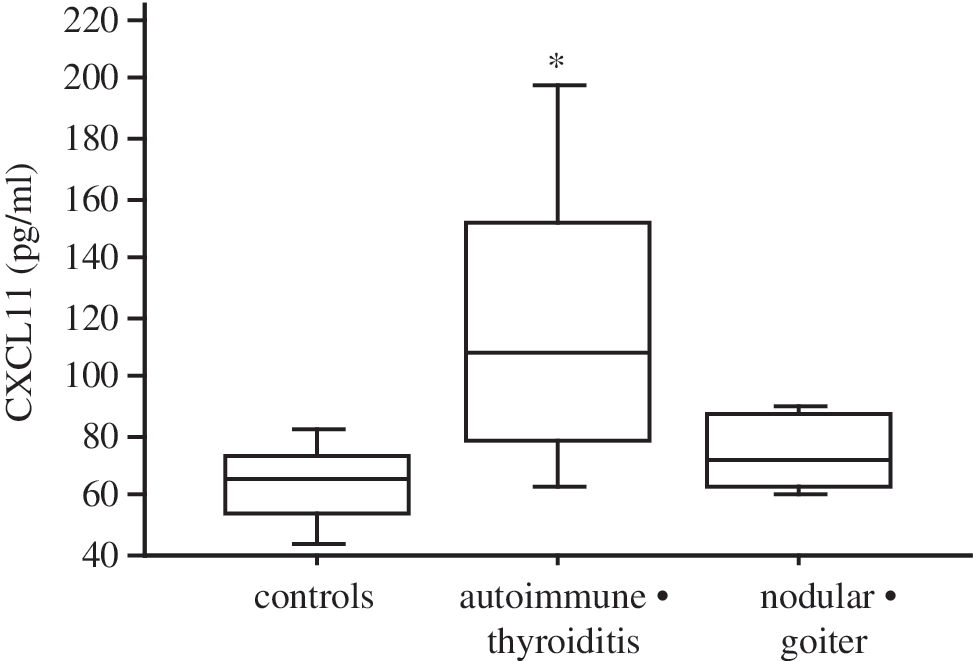
The mean chemokine (C-X-C motif) ligand 11 (CXCL11) level in patients with thyroiditis, in controls, or patients with multinodular goiter. The mean CXCL11 level was significantly (analysis of variance, P<0.001) higher in patients with thyroiditis than in controls or patients with multinodular goiter, although some overlap was evident in the low range of CXCL11 values. The box indicates the lower and upper quartiles, the central line is the median value; the horizontal lines at the end of the vertical lines are the 2.5% and 97.5% values. *P<0.05 or less versus controls or nodular goiter by Bonferroni–Dunn test.
In a simple regression analysis, CXCL11 and TSH serum levels were significantly related to each other (r=0.579, P<0.001) in patients with AT (Fig. 2).
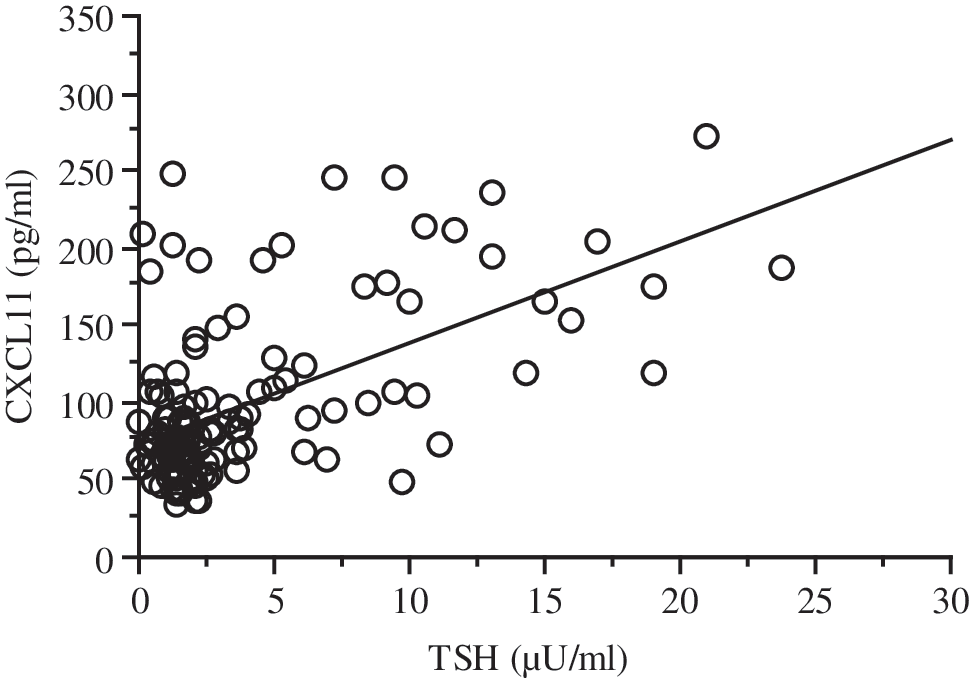
Simple regression analysis between CXCL11 and thyroid-stimulating hormone (TSH) serum levels in patients with thyroiditis. In a simple regression analysis, CXCL11 and TSH serum levels were significantly related to each other (r=0.579, P<0.001) in patients with autoimmune thyroiditis.
In an MLR model including age, thyroid volume, TSH, AbTPO, hypoechoic pattern, and the presence of hypervascularity, only age and TSH were significantly related to serum CXCL11 levels (Table 3).
Serum TSH (μU/mL=mU/L).
AU, arbitrary unit; CI, confidence interval; RC, regression coefficient.
Patients with AT and hypothyroidism had lower thyroid volume (7±7 versus 15±16 mL, P=0.01), FT4 [7.1±2.3 versus 9.8±2.5 ng/L, (9.1±3.0 versus 12.6±3.2 pmol/L) P=0.007], and FT3 [3.1±0.7 versus 3.7±0.6 pg/mL, (4.8±1.1 versus 5.7±0.9 pmol/L) P=0.04] levels, and higher degrees of echogenicity (0.9±0.3 versus 0.5±0.5 score units, P=0.001), AbTPO titers (476±465 versus 213±431 UI/mL, P=0.004), and CXCL11 (see above) than nonhypothyroid patients.
By defining a high CXCL11 level as a value at least 2 SD above the mean value of the control group (>99 pg/mL), 31% of patients with AT, 2% of controls, and none of the patients with multinodular goiter had high CXCL11 (P<0.0001).
For comparison, the mean CXCL10 level was confirmed to be significantly higher in patients with thyroiditis, particularly in hypothyroid patients, than in controls or patients with multinodular goiter (Table 1) (stat-power=1). In patients with AT, serum CXCL10 levels were significantly higher in patients older than 50 years (178±151 versus 123±142 pg/mL, P=0.001), in patients with a hypoechoic pattern (173±124 versus 128±82 pg/mL, P=0.008), and in those with hypothyroidism (221±237 versus 137±109 pg/mL, P=0.001); whereas no significant difference was observed in relation to the presence of AbTPO positivity, AbTg positivity, the presence of hypervascularity, or thyroid volume (CXCL10, 157±171, 141±148, 151±162 pg/mL; in patients with AT with thyroid volume <6 mL, between >6 and <20 mL, or >20 mL, respectively). In an MLR model including age, thyroid volume, TSH, AbTPO, hypoechoic pattern, and the presence of hypervascularity, only age [coefficient (β), 0.32; regression coefficient (RC), 0.017; 95% lower, 0.001; 95% upper, 0.029; P<0.001] and TSH [coefficient (β), 0.39; RC, 0.021; 95% lower, 0.010; 95% upper, 0.032; P<0.001] were significantly related to serum CXCL10 levels.
In a simple regression analysis, CXCL11 and CXCL10 (Fig. 3) serum levels were significantly related to each other (r=0.501, P<0.001) in patients with AT. In an MLR model of CXCL11 (ln[pg/mL]) versus age, TSH (ln[μU/mL]), and CXCL10 (ln[pg/mL]) (Table 4), only TSH (P=0.028) and CXCL10 (P=0.003) were significantly and indepedently related to CXCL11.
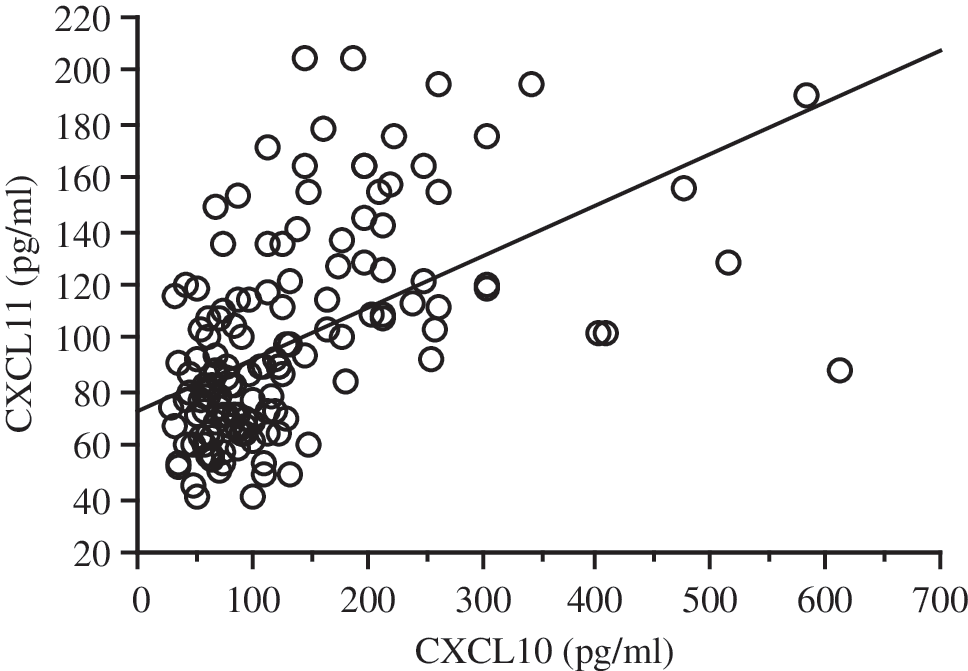
Simple regression analysis between CXCL11 and CXCL10 serum levels in patients with thyroiditis. In a simple regression analysis, CXCL11 and CXCL10 serum levels were significantly related to each other (r=0.501, P<0.001) in patients with autoimmune thyroiditis.
Serum TSH (μU/mL=mU/L).
Discussion
This study is the first to show that circulating levels of CXCL11 and CXCL10 were clearly elevated in patients with AT as compared with normal controls or patients with multinodular goiter; within the AT group, higher CXCL11 levels were associated with older age, hypothyroidism, and a hypoechoic gland. In hypothyroid patients with AT, CXCL11 levels were more strongly associated with the hypothyroidism itself than with other well-known parameters such as thyroid volume or AbTPO levels. Further, CXCL11 levels were correlated with age and serum TSH concentrations in patients with AT as a whole. Overall, these results imply that raised CXCL11 is not only associated with the autoimmune process itself, but may be a marker of a thyroiditic process eventually leading to the destruction of thyroid follicular cells with the attendant impairment in thyroid function.
These results are in agreement with recent evidences which have shown that CXC α-chemokines (Th1), especially CXCL10, play an important role in the initial phases of autoimmune thyroid disorders. Patients with newly diagnosed AT show increased serum CXCL10, in particular in the presence of thyroiditis and hypothyroidism. Serum CXCL10 levels are increased in Graves' disease (GD), especially in patients with active disease and the CXCL10 decrease, after thyroidectomy or after radioiodine, shows that it is more likely to have been produced inside the thyroid gland (García-López and others 2001; Antonelli and others 2004, 2005, 2006a, 2006b, 2007).
CXCL11 expression is strongly upregulated in response to IFN-γ. This effect is dramatically enhanced by addition of IL-1 (Cole and others 1998) or TNF-α (Tensen and others 1999a), though these pro-inflammatory cytokines alone fail to induce expression. CXCL11 mRNA can be induced in astrocytes and monocytes (Cole and others 1998), bronchial epithelial cells (Sauty and others 1999), intestinal epithelial cells (Dwinell and others 2001), endothelial cells (Mach and others 1999; Mazanet and others 2000), keratinocytes (Tensen and others 1999b; Albanesi and others 2000), macrophages (Mach and others 1999), and neutrophils (Gasperini and others 1999).
In agreement with the results obtained in various human cell types, we have recently shown (Antonelli and others 2009) that the secretion of CXCL11 in primary cultures of GD thyrocytes can be stimulated by IFN-γ and TNF-α. Further, IFN-α and IFN-β were able to stimulate CXCL9 and CXCL10 secretion in normal thyrocytes (Antonelli and others 2010a). Moreover, we have shown that CXCL9 and CXCL11 are increased in patients with AT (Antonelli and others 2011a, 2011b).
T lymphocytes play a central role in the induction of the AT response. Recent observations have indicated that specific combinations of different inflammatory cytokines (IFN-γ and/or TNF-α) transform nondestructive into destructive thyroiditis in murine experimental AT (Caturegli and others 2000; Wang and others 2002). Further, it has been suggested that one of the differences between murine experimental AT and human AT is that human thyroid glands show a chronic inflammatory environment enriched mainly with Th1 cytokines such as IFN-γ and TNF-α and enhanced apoptosis (Caturegli and others 2000; Stassi and De Maria 2002; Wang and others 2002).
The elevated levels of circulating CXCL11 in patients with AT may result from secretion by both lymphocytes and thyroid follicular cells modulated through IFN-γ. However, serum CXCL10 levels are increased in GD, especially in patients with active disease, and the CXCL10 decrease after thyroidectomy or after radioiodine shows that it is more likely to have been produced inside the thyroid gland (Antonelli and others 2006a, 2006b, 2007). These data suggest that thyrocytes may be an important source of CXCL11.
CXCL11 recruits activated Th1 lymphocytes to sites of inflammation. It can be speculated that CXCL11-induced recruitment of Th1 lymphocytes, which secrete IFN-γ, in turn stimulates chemokine production by follicular cells, thus maintaining the autoimmune process, reinforcing the effect of CXCL10.
The association of high CXCL11 levels with a hypoechoic pattern of the thyroid gland in patients with AT is readily explained by the presence of a marked lymphocyte infiltration, the histological hallmark of AT. This is in agreement with previous reports showing that CXCL10 in patients with AT is associated with a thyroid hypoechoic pattern and hypothyroidism (Antonelli and others 2004). Since serum CXCL11 concentrations were higher in hypothyroid than euthyroid patients independently of hypoechogenicity, it is possible that CXCL11 stands for a stronger inflammatory response, thus resulting in more extensive tissue destruction.
To the best of our knowledge, this is the first study reporting a correlation between CXCL11 and CXCL10 levels in an immune related disorder, such as AT. This correlation suggests that the immune process at the base of the initiation of AT (a Th1 immune response with secretion of IFN-γ and TNF-α) might be responsible for the increase of both chemokines in AT.
However, CXCL11 has some peculiarities with regard to CXCL10. In fact, CXCL10 and CXCL9 also bind CXCR3, but with lower affinity (Cole and others 1998; Cox and others 2001) and less potency (Cole and others 1998) than CXCL11. Further, there is evidence that CXCL11 is able to bind both the free and coupled forms of the receptor, whereas CXCL10 and CXCL9 bind only the coupled receptor (Cox and others 2001). Further, CXCL11 is an antagonist of the CC chemokine receptor 3 (CCR3) (Loetscher and others 2001), a chemokine receptor expressed n eosinophils and Th2 lymphocytes, thus suggesting that CXCL11 may act to further polarize T cell recruitment at sites of expression.
The peculiarities of CXCL11 just mentioned, with regard to CXCL10, suggest that they may have, at least in part, a different role in AT which remains to be investigated.
In conclusion, high circulating levels of CXCL11, together with CXCL10, have been shown in patients with AT, in particular in the presence of markers of a more aggressive immune attack, such as hypoechogenicity of the thyroid gland and hypothyroidism. Longitudinal observations in large patients cohorts will be needed to evaluate whether circulating CXCL11 levels may serve as a clinical prognostic marker in AT.
Footnotes
Author Disclosure Statement
No competing financial interests exist.