
Abstract
Higher blood levels of the essential amino acid phenylalanine (Phe) together with impaired conversion of Phe to tyrosine (Tyr) have been observed in patients suffering from inflammatory conditions. Data suggest that inflammatory responses may interfere with Phe metabolism. This study aimed to investigate whether treatment with cytokine interferon-α (IFN-α) influences Phe concentrations and the Phe to Tyr ratios (Phe/Tyr) measured by HPLC. Twenty-five patients (9 females, 16 males, aged mean±SD: 44.5±11.0 years) with hepatitis C virus (HCV) infection were examined before and after 1 month of effective antiviral therapy with pegylated IFN-α and weight-based ribavirin. Results were compared to HCV-RNA titers and concentrations of neopterin. IFN-α treatment was associated with a drop of HCV load (from median 6.3 to 3.2 log10 copies/μL; P<0.001) and an increase of neopterin concentrations (from median 4.83 to 12.1 nM; P=0.001) which confirms effectiveness of therapy. Before therapy, median Phe concentration were 123.9 μM, Tyr was 98.8 μM, and Phe/Tyr was 1.23 μmol/μmol, and under therapy median Phe concentrations increased to 132.6 μM and Phe/Tyr to 1.33 (both P<0.05; paired rank test), Tyr levels remained unchanged. The increase of Phe concentrations and of Phe/Tyr in HCV infected individuals is caused by IFN-α therapy. Data indicate that activity of enzyme phenylalanine 4-hydroxylase becomes impaired. Future studies should show whether side effects of IFN-α treatment such as mood changes and depression will be associated with the alterations of Phe metabolism.
Introduction
C
Increased blood concentrations of phenylalanine (Phe) and of the Phe to tyrosine (Tyr) ratio have been described in diseases such as human immunodeficiency virus-1 (HIV-1) infection (Ollenschläger and others 1988; Zangerle and others 2010), trauma, sepsis (Ploder and others 2008), burns (Rath and others 1987), and malignancy (Ollenschläger and others 1988; Neurauter and others 2008a), and also in the healthy elderly (Capuron and others 2011). The reason for the increase of Phe and of Phe/Tyr in these inflammatory conditions is still unexplained. Phe/Tyr better than Phe alone is a useful measure of the activity of phenylalanine 4-hydroxylase (PAH; EC 1.14.16.1) (Rosenblatt and Scriver 1968; Anderson and others 1994; Shintaku 2002). Accordingly increased Phe concentrations and an increased Phe and Phe/Tyr in such patients indicate an impaired activity of PAH.
The accumulation of Phe in patients correlates with concentrations of immune activation markers such as neopterin or soluble tumor necrosis factor receptors (Ploder and others 2008; Neurauter and others 2008a; Zangerle and others 2010). Moreover, in patients with HIV-1 infection, increased Phe and Phe/Tyr were associated with the clinical presentation of patients, with HIV load and inversely with CD4+ T-cells counts (Zangerle and others 2010). Interestingly successful antiretroviral therapy of patients led to a decline of Phe and Phe/Tyr along with the declines of HIV load and concentrations of neopterin and with the increase of CD4+ cell counts.
Taken together, data support the view that the process of immune activation and inflammation is involved in the impairment of PAH (Neurauter and others 2008b). However, thus far only a correlation between these effects was described which does not allow a conclusion about any cause-effect relationship. This study aimed to investigate whether the treatment of patients with pro-inflammatory cytokines influences the turnover of Phe. In patients with HCV infection we examined whether therapeutic administration of IFN-α is associated with alterations of plasma Phe and Tyr concentrations and of Phe/Tyr.
Materials and Methods
Patients
This retrospective study is based on a total of 50 plasma specimens which were obtained from 25 patients with established HCV infection (9 females=36%, 16 males=64%, aged mean±SD: 44.5±11.0 years). Median HCV load was 1.996,000 copies/μL=6.3 log10 copies/μL (interquartile range: 5.05–6.81 log10 copies/μL). Patients were treated with pegylated IFN-α2a 180 μg/week or IFN-α2b 1.5 μg/kg body weight per week and ribavirin (800 mg for patients with HCV genotype 2 and 3 or 1,000–1,200 mg for patients with HCV genotype 1 or 4). All patients were included in this study who entered treatment between July 2008 and March 2010 and showed a sustained treatment response, and they were selected on the basis that plasma samples were available collected at baseline and after 1 month of therapy. All participants' rights were protected, and according to the Helsinki Declaration, informed consent was obtained that a small portion of their blood collected for routine examinations was forwarded for further scientific testings.
Laboratory examinations
HCV RNA levels were determined using the Cobas Amplicor assay (Roche Molecular Systems, Branchburg, NJ) immediately after the visits of the patients at the outpatient unit. Concentrations of neopterin were analyzed using a commercially available competitive ELISA (BRAHMS GmbH, Hennigsdorf, Germany) with a detection limit of 2 nM (Mayersbach and others 1994).
Phe and Tyr concentrations were simultaneously determined by HPLC, monitoring their natural fluorescence at an excitation wavelength of 210 nm and an emission wavelength of 302 nm (Neurauter and others 2008a). One hundred microliter plasma was diluted with 100 μL of 500 μM 3-nitro-L-tyrosine (internal standard), and 25 μL of 2 M trichloroacetic acid was used to precipitate and separate proteins. After centrifugation, supernatants of the samples were diluted 1:25 with 0.015 M potassium dihydrogenphosphate, which was also used as elution buffer on HPLC. An albumin-based calibration mixture was prepared which contained 100 μM Phe and 100 μM Tyr and underwent the same preanalytical procedures as plasma specimens. The intra- and interassay coefficients of variation of the method ranged between 5.1% and 10%. To estimate the activity of PAH, the ratio of the substrate Phe versus the concentrations of the enzyme product Tyr (=Phe/Tyr) was calculated (Rosenblatt and Scriver 1968; Anderson and others 1994; Neurauter and others 2008b).
Statistical analysis
Statistical comparisons were made using nonparametric tests because some of the data sets did not show normal distribution: Wilcoxon paired rank test was applied for group comparisons and Spearman rank correlation to test for associations between variables.
Results
In patients with HCV infection before IFN-α therapy, Phe and Tyr concentrations were (mean±SD) 122±34.0 μM and 109±50.1 μM, respectively, Phe/Tyr was 1.23±0.31. HCV load was 5.9±1.0 log 10 copies/μL and neopterin concentrations were 8.2±9.3 nM, 7/25 (28%) patients presented with elevated neopterin concentrations (upper limit of the normal range: 8.7 nM) at baseline. There were no differences between male and female patients.
After 4 weeks of IFN-α therapy, median HCV load dropped by ∼2.5 orders of magnitude to 3.1±1.9 log 10 copies/μL (U=4.292, P<0.001; paired test), whereas neopterin concentrations increased to 14.4±7.9 nM (±75%, U=3.351, P=0.001; Fig. 1). Phe concentrations increased to 139±30.6 μM (±13.5%, U=2.085, P=0.037) and Phe/Tyr increased to 1.32±0.27 (±7.3%, U=2.428, P<0.015; Fig. 2). Tyr concentrations were not different from baseline (110±35.1 μM; U=0.390, not significant).
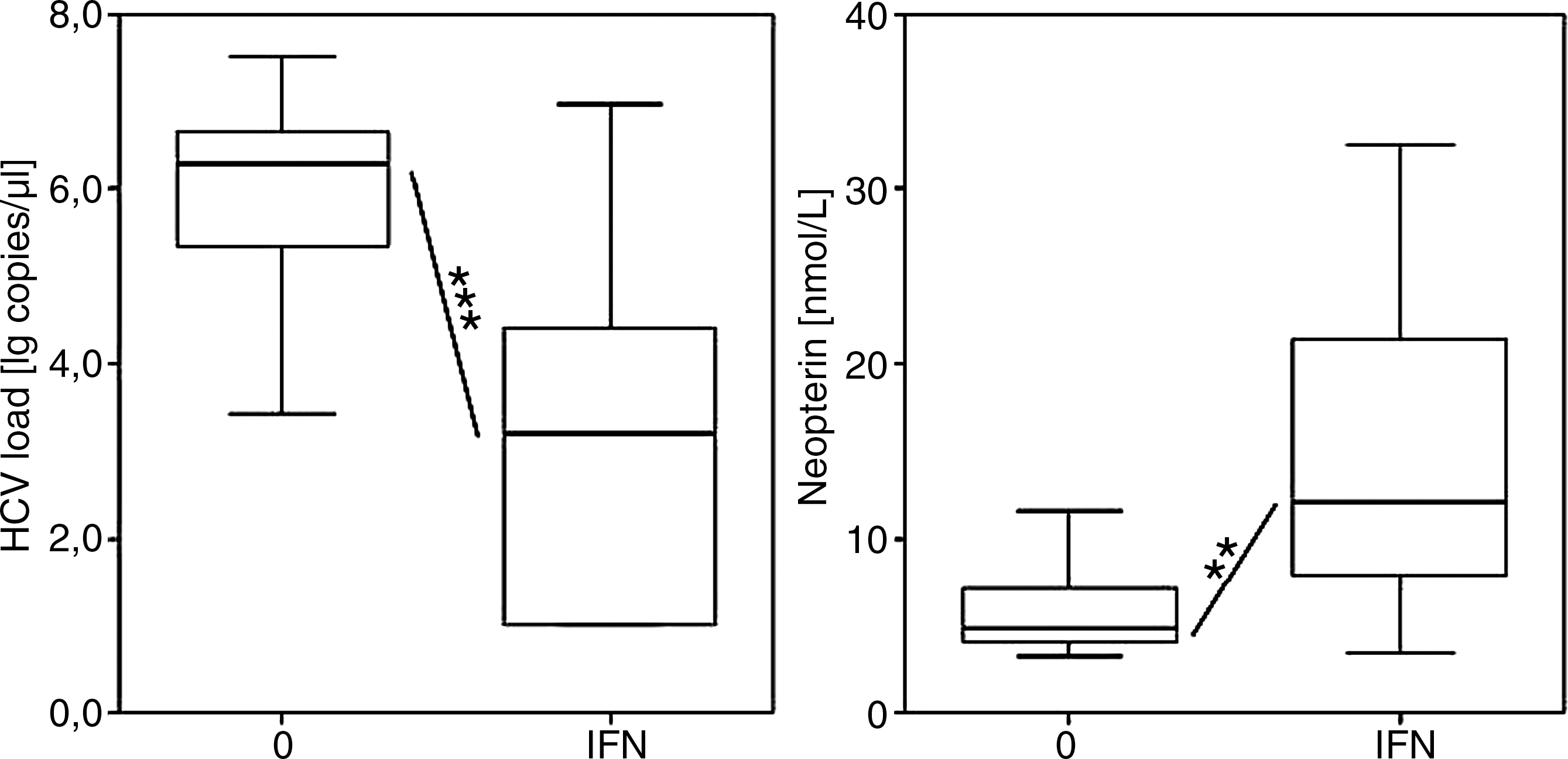
HCV load (left; note log scale) and neopterin (right) concentrations in patients with HCV infection before (0) and after 1 month of IFN-α therapy (IFN), boxes with medians, ranges and interquartile ranges are shown; **P=0.001, ***P<0.001. HCV, hepatitis C virus; IFN, interferon.
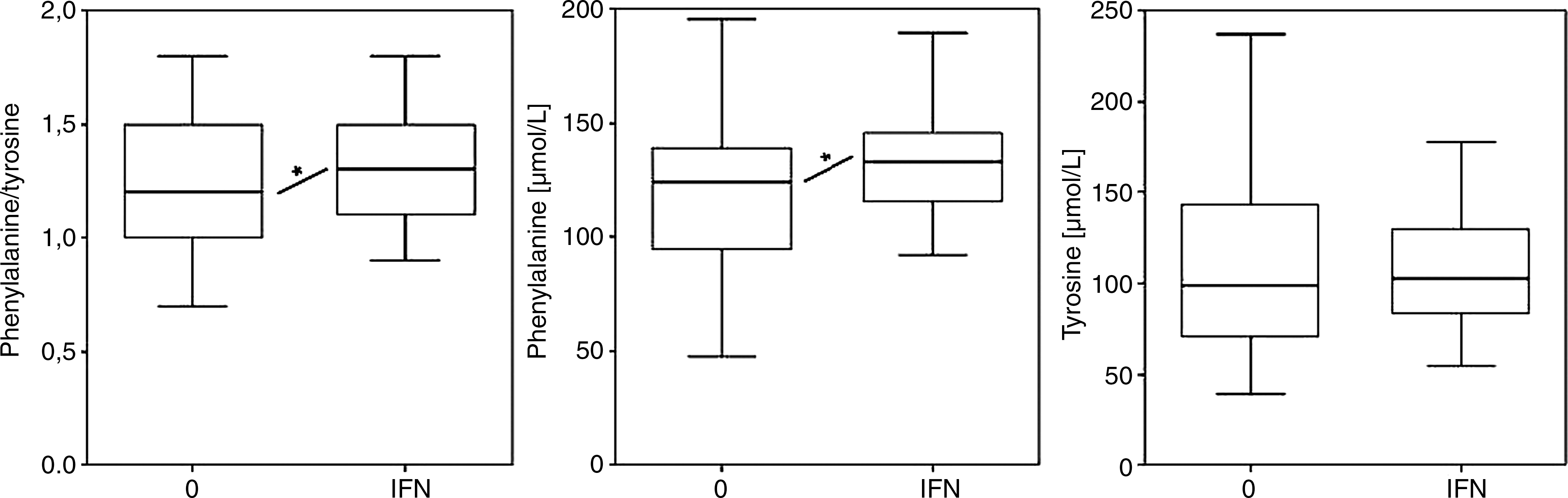
Plasma phenylalanine to tyrosine ratios (left), and phenylalanine (middle) and tyrosine (right) concentrations in patients with HCV infection before (0) and after 1 month of IFN-α therapy (IFN, filled columns), boxes with medians, ranges and interquartile ranges are shown; *P<0.05.
There were no significant correlations between HCV-load, Phe/Tyr and Phe, Tyr and neopterin concentrations, neither at baseline nor after IFN-α therapy.
Discussion
Treatment with IFN-α plus ribavirin was effective in suppressing HCV production in patients. At the same time the concentrations of immune activation marker neopterin increased. The increased production of neopterin in macrophages is related to the antiproliferative effects which are triggered by IFNs in target cells. Therefore, the monitoring of neopterin production in patients treated with, for example, IFN-β is utilized to indicate the biological response to therapy (Durastanti and others 2011).
Treatment was also associated with an increase of Phe concentrations and of Phe/Tyr in the plasma of patients. Data allow us to conclude that the process of immune activation and inflammation which is elicited during treatment with IFN-α underlies the increase of Phe and of Phe/Tyr. Results indicate diminished hydroxylation of Phe to Tyr and thus impaired activity of PAH. Thereby plasma levels of Phe and Tyr and Phe/Tyr are representative because relevant PAH activity takes place only in liver (Shintaku 2002). Still, the exact mechanism by which IFN-α therapy might influence PAH activity is not clear.
Function of monoxygenase PAH requires cofactor 5,6,7,8-tetrahydrobiopterin (BH4) (Fitzpatrick 2003), a pteridine derivative like neopterin. IFNs induce GTP-cyclohydrolase I (GCH, EC 3.5.4.16), the key enzyme for biosynthesis of pteridines, in various cells and cell lines (Werner and others 1989). However, only human and primate macrophages and dendritic cells form neopterin upon induction of GCH (Huber and others 1984; Wirleitner and others 2002), whereas other human cells and cells from other species form BH4 instead. Thus, during IFN-α therapy one would expect an increased production of not only neopterin but also BH4. As a consequence PAH activity should increase and Phe levels and Phe/Tyr should decline in patients. However, the opposite was observed in our study, data indicating that during IFN-α therapy PAH activity becomes subnormal despite induction of GCH as is shown by the increase of neopterin concentrations. Diminished stability of BH4 could underlie these findings.
Oxidative metabolites induced by IFN-α administration may reduce the half-life of BH4, because this tetrahydropteridine derivative is extremely sensitive to oxidation (Connor and others 1979; Fuchs and others 2001). Macrophages and other cells stimulated with IFN are well known to produce reactive oxygen species (ROS) at a high rate (Nathan and others 1983). Overwhelming production of ROS may wipe out antioxidant defense systems and, in turn, oxidative stress is developing. Earlier in patients with chronic HCV infections decreased antioxidative defense was observed when pegylated IFN-α and ribavirin was applied (Lin and Yin 2009). At the same time several biochemical pathways related to immune effector functions were observed to be induced by IFN-α therapy (Fuchs and others 1992). Oxidative stress induced by IFN-α could be involved in the decline of BH4 and the observed increase of serum Phe concentrations and Phe/Tyr. Alternatively or in addition, ROS may interfere with redox-sensitive structural elements of proteins such as sulfhydryl residues and thereby influence their tertiary structures (Schroeder and others 2010). This may impair binding of the substrate and/or the cofactor to enzyme PAH (Fuchs and others 2011).
One important consequence of BH4 deficiency would be an impaired formation of the end products of this pathway, namely catecholamine neurotransmitters adrenaline, noradrenaline, and dopamine, because Tyr is not an end product. Tyr is substrate for a second enzymatic reaction, in which tyrosine 3-hydroxylase, another BH4-dependent enzyme, forms L-DOPA (Fitzpatrick 1999; Shintaku 2002). This fact may explain why Tyr levels remained rather unchanged in our treated patients when cofactor deficiency will affect both, the production and the conversion of Tyr. Earlier studies imply impaired metabolism of dopamine, and noradrenaline in mood disorders (Shintaku 2002; Dunlop and Nemeroff 2007; Stein 2008; Neurauter and others 2008b). So the impaired conversion of Phe might contribute to the development of neuropsychiatric symptoms in patients treated with IFN-α. Depressive symptoms frequently occur in patients on IFN-α treatment for infectious diseases or cancers (Hauser and others 2002; Konsman and others 2002), and clinical symptoms like depressive mood may preferentially develop in patients presenting with moderate hyperphenylalaninemia.
The impaired PAH activity would be in addition to the influence of IFN-α therapy on the activity of indoleamine 2,3-dioxgenase (IDO) and serotonin biosynthesis. The possible association between the development of neuropsychiatric symptoms and the decline of tryptophan concentrations due to its accelerated degradation by IDO is intensely investigated (Bonaccorso and others 2002; Hauser and others 2002; Widner and others 2002; Capuron and others 2003; Raison and others 2005; Cozzi and others 2006; Larrea and others 2007; Zignego and others 2007; Loftis and others 2010; Comai and others 2011). Many patients who develop depressive symptoms under IFN-α therapy respond rather well to treatment with selective serotonin reuptake inhibitors (SSRI), but some do not (Ferrando and others 1997; Hunchak 1997; Dantzer and others 2008). Moreover, no association was found between specific IDO polymorphisms and the appearance of IFN-α related depression in patients with HCV infection (Galvão-de Almeida and others 2011). Such observations suggest that in addition to cytokine-induced tryptophan breakdown, abnormal dopaminergic and noradrenergic neurotransmitters supply could be important.
Until recently, the role of dopamine in the etiopathology and treatment of depression was largely ignored (Kapur and Mann 1992; Bottiglieri and others 2000; Stein 2008). This occurred despite a dopaminergic theory of depression being proposed more than 35 years ago (Braestrup and others 1975). Still in the treatment of depression, adrenergic reuptake inhibitors are less common than SSRIs. Parallel measurements of tryptophan degradation and Phe/Tyr could probably allow better stratification of patients regarding their potential responses to treatment regimens involving serotonergic or adrenergic reuptake inhibitors. The observation that parkinsonism induced by IFN-α and ribavirin recovers after L-DOPA treatment would be in line with our findings that IFN-α therapy impairs Phe metabolism (Bersano and others 2008).
Our findings are limited by the fact that direct measurements of PAH activity or oxidative stress were not performed. Also we did not directly determine biopterin or BH4 concentrations, for that the methodological requirements are very complex and necessary preanalytics almost prevent proper sample collections in clinical settings. One cannot exclude that IFN-α might have a direct effect on PAH or on the recycling biochemistry of BH4. Unfortunately there were also no measures of mood or cognition available in this retrospective study, and thus the relevance of the amino acid changes for the quality of life of patients cannot be extrapolated. Finally the study population is still too small and did not allow any statistical investigation of the possible influence of demographic factors such as HCV genotypes on Phe and Phe/Tyr.
In conclusion, our study shows that IFN-α therapy in patients with HCV infection impairs Phe metabolism. Data support the concept that cytokines released during immune activation are responsible for the increase of Phe and Phe/Tyr in patients with HIV infection, trauma, sepsis and the like (Rath and others 1987; Ollenschläger and others 1988; Ploder and others 2008; Neurauter and others 2008a; Zangerle and others 2010; Capuron and others 2011). Our results would be explainable by an impaired PAH in patients with HCV infection due to developing BH4 deficiency under IFN-α therapy. Future studies are required to demonstrate the influence of IFN-α on adrenergic and/or noradrenergic neurotransmission and the possible association between elevated Phe and/or Phe/Tyr with neuropsychiatric symptoms in patients treated with this cytokine.
Footnotes
Acknowledgments
We thank Mrs. Maria Pfurtscheller for excellent technical assistance.
Author Disclosure Statement
No competing financial interests exist.