
Abstract
We assessed long-term outcome of 118 consecutive patients in chronic phase of chronic myeloid leukemia (CML) treated with interferon-alpha (IFN-α) in the Central and Northern Moravia region between 1989 and 2006 with focus on operational cure. The median follow-up was 82.6 months (range 12.4–212.6). Eighteen (15.3%) patients achieved complete cytogenetic response (CCyR) after median 16.7 (3.7–40.8) months. Nine of these patients (7.6%) achieved BCR-ABL negativity in nested reverse transcriptase–polymerase chain reaction [“complete” molecular response (CMR)] and 6 of them have been operationally cured without any treatment for median 6 (4–10) years, while 2 continue with IFN-α and 1 died from CML-unrelated cause. Operationally cured patients had a significantly lower percentage of initial peripheral promyelocytes, blasts, and erythroblasts than the rest of patients treated for more than 12 months (P=0.01–0.03). Unlike patients with sole CCyR, the majority of whom lost CCyR despite continuing IFN-α therapy and required imatinib, patients who achieved CMR had excellent long-term outcome.
C
Interferon-alpha (IFN-α) was one of the main treatment options before the discovery of TKIs. Reports of complete cytogenetic response (CCyR) and complete molecular response (CMR) associated with excellent long-term prognosis achieved after IFN-α therapy have been published (Mahon and others 2002; Kantarjian and others 2003). Some patients maintained CCyR after discontinuation of IFN-α (Mahon and others 2002). There is laboratory evidence of effective targeting of quiescent CML stem cells by IFN-α (Pierce and others 2001). Angstreich and others (2005) demonstrated that in comparison with imatinib, IFN-α had significantly greater in vitro activity against primitive Ph-positive progenitors. IFN-α also stimulates autologous cytotoxic T lymphocytes to specifically recognize Bcr-Abl or Bcr-Abl-dependent antigens (Burchert and Neubauer 2005).
We evaluated outcome of all CML patients treated in the Central and Northern Moravia region with IFN-α alone or in combination with cytosine arabinoside (Ara-C) or hydroxyurea with special attention to achievement of BCR-ABL negativity (CMR) assessed by nested reverse transcriptase–polymerase chain reaction (RT-PCR).
All consecutive patients with chronic phase CML diagnosed and treated with IFN-α at the University Hospital Olomouc between 1989 and 2006 were included. Patients participating in clinical studies gave IFNormed consent approved by the local Ethics Committee. Diagnosis of CML was based on cytogenetic confirmation of the Ph chromosome and/or demonstration of the BCR-ABL1 fusion gene using nested RT-PCR or fluorescence in situ hybridization (FISH). Cytogenetic examinations were performed according to the standard procedure from bone marrow cells at the time of starting IFN-α therapy and then once every 6 months or in cases of suspected progression. Molecular response was assessed by nested RT-PCR (van Dongen and others 1999) and from November 2004 also by real-time quantitative RT-PCR (Gabert and others 2003). Sensitivity of the nested RT-PCR method was 10−5. Responses to treatment were evaluated according to European LeukemiaNet criteria (Baccarani and others 2009). Mann–Whitney test and log rank test were used for statistical analysis. Probability of overall survival was calculated according to the method of Kaplan and Meier (1958).
Roferon (Roche, Basel, Switzerland) or Intron-A (Schering-Plough, Kenilworth, NJ) were used for the treatment. IFN-α was applied in a single daily subcutaneous injection. The initial dose of 1.5 or 3 MU was increased depending on the patient's tolerance to 9 or 10 MU daily. Inpatients who did not achieve complete hematologic response and in cases with WBC >5×109/L, hydroxyurea or Ara-C (10–20 mg s.c. or 40 mg p.o. daily) was added to achieve WBC=2–4×109/L. In cases with neutropenia (<1.0×109/L) or thrombocytopenia (<50×109/L), the dose of IFN-α was appropriately reduced.
The study group comprised consecutive 118 adult patients in the chronic phase of CML at the time of diagnosis. The median time from diagnosis to treatment initiation was 1 month (range 0–43 months). Patients were treated with IFN-α for a median period of 12 months (0.3–192). The median follow-up was 82.6 months (12.4–212.6). Average IFN-α dose was 9 MU (1.5–10) daily. Sixty-six patients (55.9%) were treated with IFN-α in combination with hydroxyurea and 32 patients (27%) with low dose Ara-C. Seven patients (5.9%) underwent autologous hematopoietic stem cell transplantation.
Out of all 118 patients, 18 (15.3%) patients achieved CCyR in a median of 16.7 months (3.7–47.3) and maintained their response for a median of 64 months (7–267). Follow-up of 18 patients who achieved CCyR is depicted in Fig. 1. Nine responders achieved CMR (Table 1). Six of these 9 responders continuously maintained CMR while remaining 3 achieved negativity and maintained at least major molecular response (MMR) at follow-up. A higher proportion of these 9 patients (55.6%) had low Sokal or Hasford scores. The initial percentage of promyelocytes [median=0 (0–1) versus median=1 (0–15); P=0.03], erythroblasts [median=0 (0–0) versus median=0 (0–12); P=0.021], and blasts [median=0 (0–1) versus median=1 (0–12); P=0.01] in peripheral blood was significantly lower in patients who achieved CMR in comparison with all patients treated for more than 12 months according to the Mann–Whitney test. Six patients discontinued IFN-α (after the slow cessation over 1–2 years) because of at least 2-year CMR. All 6 patients have been off any treatment for a median of 6 (4–10) years and are considered to have achieved “operational cure” defined by Talpaz others (1991). The difference in probability of overall survival according to Kaplan and Meier has not reached statistical difference in the log rank test (Fig. 2).
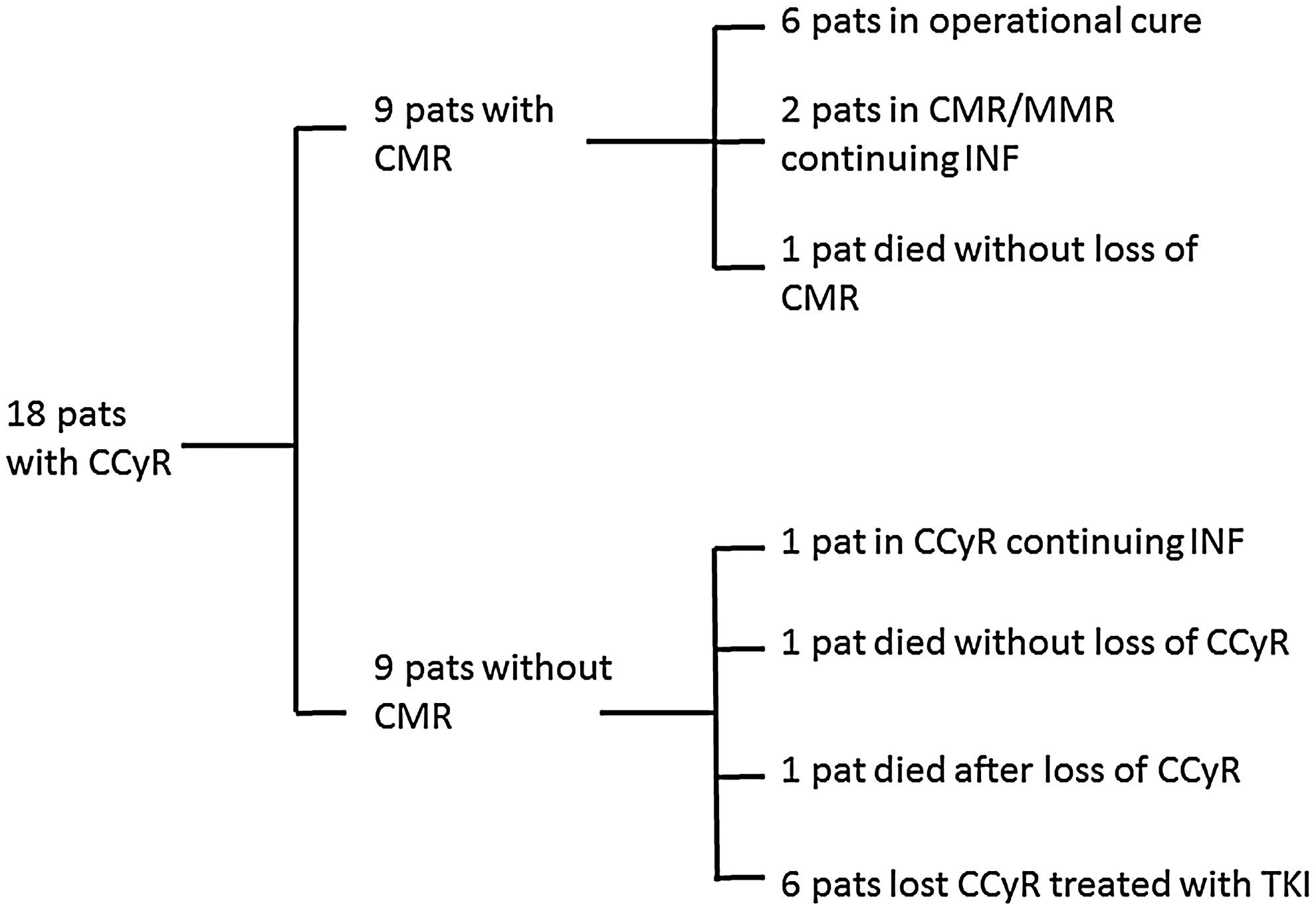
Analysis of complete responders treated with INF-α. Nine patients reached negativity of BCR-ABL in reverse transcriptase–polymerase chain reaction (RT-PCR) [complete molecular response CMR)]: 1 discontinued INF-α due to intolerance and maintained CMR without any treatment for 2 following years and died from causes not related to chronic myeloid leukemia, 2 continue on INF-α maintaining at least major molecular response (MMR), 6 patients discontinued INF-α because of prolonged CMR. The second half of patients who achieved complete cytogenetic response (CCyR) had not achieved CMR: 6 lost their CCyR and were switched to treatment with tyrosine kinase inhibitors (TKIs), 1 died without the loss of CCyR from suicide due to severe depression, 1 died after the loss of CCyR due to blastic transformation, 1 patient continues on INF-α and is still in CCyR. INF, interferon alpha.
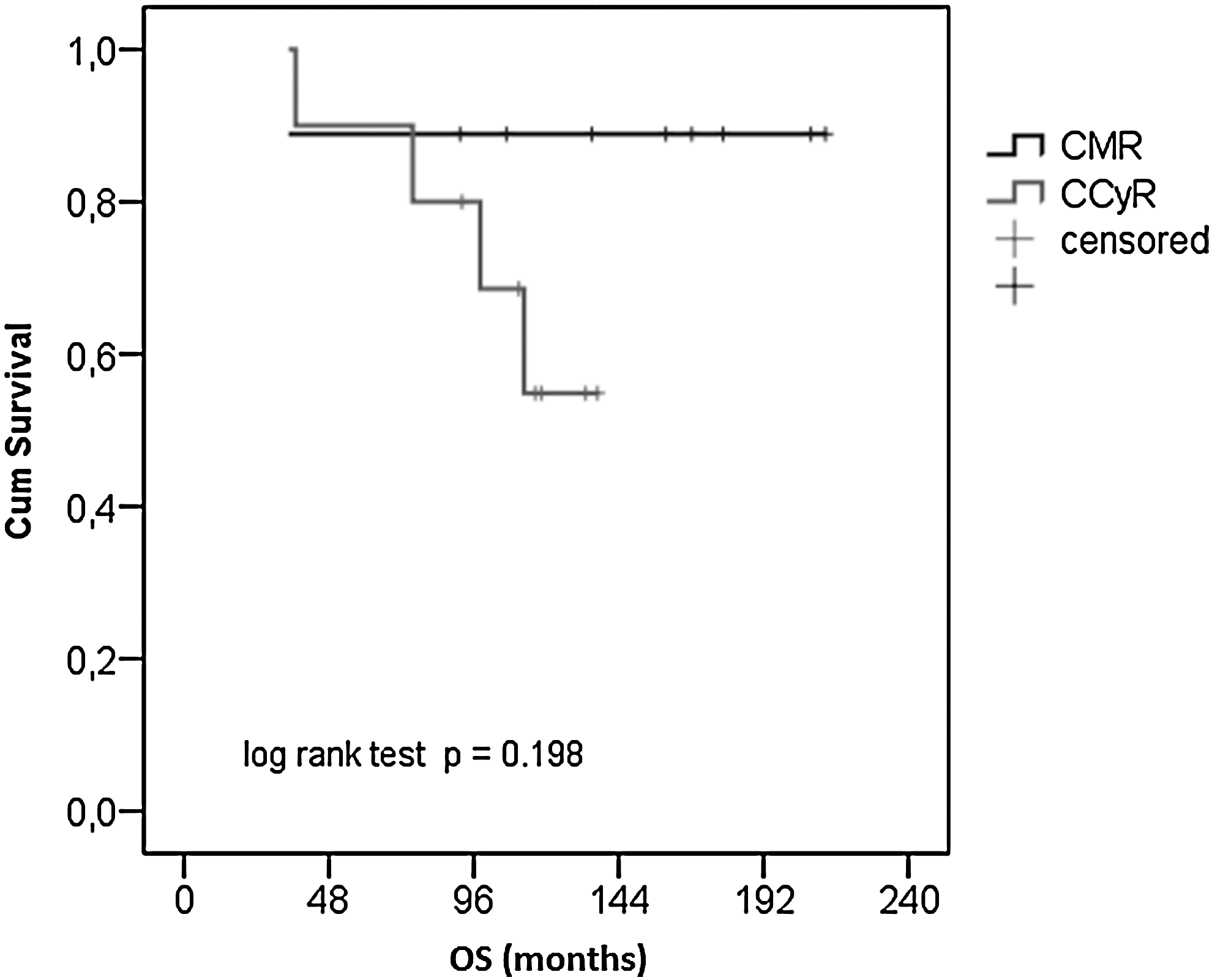
Comparison of overall survival (OS) probability according to Kaplan and Meier between the patients who achieved negativity of BCR-ABL in RT-PCR (CMR) and the patients who achieved CCyR but had not achieved CMR.
Patient 6 was treated with autologous hematopoietic stem cell transplantation with peripheral stem cells collected after mini-ICE chemotherapy before achieving CMR after INF-α. Patient 8 was treated with autologous bone marrow transplantation before achieving CMR with INF-α.
Time to CMR in the patient cannot be estimated certainly because of irregular monitoring of molecular response.
M, male; F, female; CCyR, complete cytogenetic response; CMR, complete molecular response; IM, intermediate; MMR, major molecular response; RT-PCR, reverse transcriptase–polymerase chain reaction; INF-α, interferon alpha.
Seventy-seven patients (65.3%) from our cohort received the treatment with imatinib after the failure of IFN-α. Interestingly, 30 of them (39%) achieved CMR after imatinib.
There are very few reports on long-term follow-up and significance of CCyR, CMR, and operational cures in CML after IFN-α probably due to the rare occurrence of CMR and introduction of imatinib in patients with CCyR. Kantarjian published the only single center analysis with 512 patients treated with IFN-α where 20 patients (3.9%) achieved CMR (Kantarjian and others 2003). He concluded that achievement of CCyR and CMR was associated with excellent long-term event-free survival. Mahon and others (2002) stopped IFN-α in 15 patients with CCyR (for more than 24 months duration) and none of them experienced disease progression in the next 3-year follow-up. Results were recently updated (Mahon and others 2010). Neither in CMR patients nor in patients with fluctuating levels of BCR-ABL1 disease progression was observed (Mahon and others 2010). It was hypothesized that maintenance of low minimal residual disease (without the need of complete elimination of BCR-ABL1 positive cells) after IFN-α cessation is a result of ongoing IFN-α-induced immunological CML suppression (Ross and others 2011). There is little data concerning the immunological markers that would predict the therapeutic effect of IFN-α. Recently, a unique cytokine profile (increase in NK-cells and T-lymphocyte subpopulation) in complete responders able to discontinue IFN-α was described (Kreutzman and others 2011). However, its predictive role needs to be confirmed.
The rate of CMR in our patients who were treated after the failure of IFN-α with imatinib is in agreement with the recently published results of randomized trial that compared imatinib with the combination of IFN-α with imatinib (Preudhomme and others 2010). Preudhomme with coworkers observed 20% of undetectable molecular disease after the combination treatment at 24 months of follow-up which is complying with the 39% rate of CMR observed in our group of patients sequentially treated with IFN-α and imatinib after considerably longer follow-up.
To summarize, our single-center study contributes to the ongoing quest for different ways toward permanent cure of CML. We observed a 7.6% achievement rate of CMR after IFN-α in a group of 118 consecutive patients with chronic phase CML treated in a defined region in intention-to-treat retrospective analysis. Our results showed that achievement of isolated CCyR was not sufficient for operational cure. Only achievement of CMR allowed safe cessation of IFN-α without relapse in the follow-up. Finally, we demonstrated specific features in differential WBC associated with the molecular response.
Footnotes
Acknowledgments
The work was supported by grants MSM 6198959223 and MSM 6198959205 (Ministry of Education, Youth and Sports, the Czech Republic) and LFUP 2011-006. We are grateful to Mgr. Pavel Kurfürst for editorial help.
Authors' Contributions
E.F. treated the patients, designed the study, analyzed the data, drafted the manuscript; A.K. collected and analyzed the data, drafted the manuscript; J.Z. performed the statistical analysis; M.D., S.R., and P.R. performed the molecular testing; M.H. and M.J. performed cytogenetic analyses and FISH; K.I. treated the patients and critically reviewed the manuscript; all authors reviewed and approved the final version of the manuscript.
Author Disclosure Statement
E.F. received honoraria, study support, participated in advisory boards, and acted as consultant for Bristol-Myers Squibb and Novartis. The remaining authors declare no competing financial interests.