
Abstract
Tumor necrosis factor (TNF)-α plays a central role in psoriatic arthritis (PsA). A subgroup of patients with PsA do not respond to anti-TNF-α antibodies but respond to TNF receptor p75-Fc IgG fusion protein (etanercept), which also neutralizes lymphotoxin (LT)-α. It has been suggested that LT-α might be involved in the development of the disease. We determined LT-α serum levels in 15 PsA patients before (T0) and after 3, 6, 9, and 12 months of etanercept therapy (T3, T6, T9, and T12, respectively) and correlated them with their response to treatment. Bath Ankylosing Spondylitis Disease Activity Index, Psoriasis Area Severity Index, Disease Activity Score (DAS28), erythrocyte sedimentation rate (ESR), and C reactive protein (CRP) levels were assessed at the same time points. All patients showed a clinical response at T6, which persisted up to T12; ESR and CRP mean levels significantly decreased at T3 and remained within the normal range up to T12. LT-α levels significantly increased from T3 to T6 and returned to baseline levels at T12. Therefore, the LT-α serum levels do not seem to correlate with clinical and laboratory parameters of the response to etanercept in PsA patients. Further studies are required to better define the role of LT-α and LT-α blockade by etanercept in PsA patients.
Introduction
T
High levels of LT-α have been detected in the serum and synovial fluid of a subgroup of RA patients and, in particular, in juvenile RA patients (Buch and others 2004). Of note, the clinical response to etanercept has been reported in 38% to 75% of subjects with RA after the failure of anti-TNF-α monoclonal antibody therapy (Di Poi and others 2007). It is known that TNF-α also plays an important role in the pathogenesis of psoriasis and psoriatic arthritis (PsA) and that both diseases respond to anti-TNF-α monoclonal antibodies (Mease 2005). Moreover, TNF-α/LT-α inhibition with etanercept down-regulates multiple proinflammatory cytokines, such as interleukin (IL)-1, IL-8, and IL-23, in psoriasis plaques (Gottlieb and others 2005). Among the PsA patients, there is a subgroup that does not respond to anti-TNF-α monoclonal antibodies but responds to etanercept (Conti and others 2007; Mazzotta and others 2009), suggesting that in these patients, LT-α might also play a role in the development of the disease. The aim of the present study was the determination of LT-α serum levels in patients affected by PsA before and during etanercept treatment and the correlation with their response to treatment.
Materials and Methods
Fifteen consecutive patients (8 women and 7 men; age 26–73 years) who had been affected by PsA, attending our outpatient clinic and eligible for etanercept treatment, were enrolled. Inclusion criteria were as follows: Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) ≥4, Psoriasis Area Severity Index (PASI) ≥20, Disease Activity Score (DAS28) >5.1, and erythrocyte sedimentation rate (ESR) and/or C reactive protein (CRP) level ≥2 times the normal range. Response criteria were as follows: BASDAI ≤2, PASI ≤10, DAS28 ≤3.2, and normalization of ESR and CRP levels. Etanercept was subcutaneously given at a dose of 25 mg twice a week for 12 months. Clinical evaluation was performed every 3 months for a 12 month-follow-up period. Serum samples were obtained before (T0) and then after 3, 6, 9, and 12 months of etanercept treatment (T3, T6, T9, and T12, respectively). The LT-α serum levels were determined by an enzyme-linked immunosorbent assay (Bender MedSystems GmbH, Vienna, Austria) according to the manufacturer's protocol and reported as pg/mL. Results are expressed as means±standard deviation. Statistical analysis was performed by 1-way analysis of variance, and comparisons among the values of laboratory parameters at each follow-up time point to the baseline level were performed by Bonferroni's multiple-comparisons t-test. The significant level was set at P≤0.05.
Results
All patients showed a clinical response at T6 that persisted up to T12 (Fig. 1A–C). ESR and CRP mean levels significantly decreased at T3 (P<0.05) and remained within the normal range up to T12 (Fig. 1D and E, respectively). The LT-α serum levels were 13,100±11,491 at T0, then significantly increased at T3 (29,560±20,868; P<0.05) and T6 (32,256±17,320; P<0.01), and gradually returned to baseline levels at T12 (12,616±9,094) (Fig. 1F).
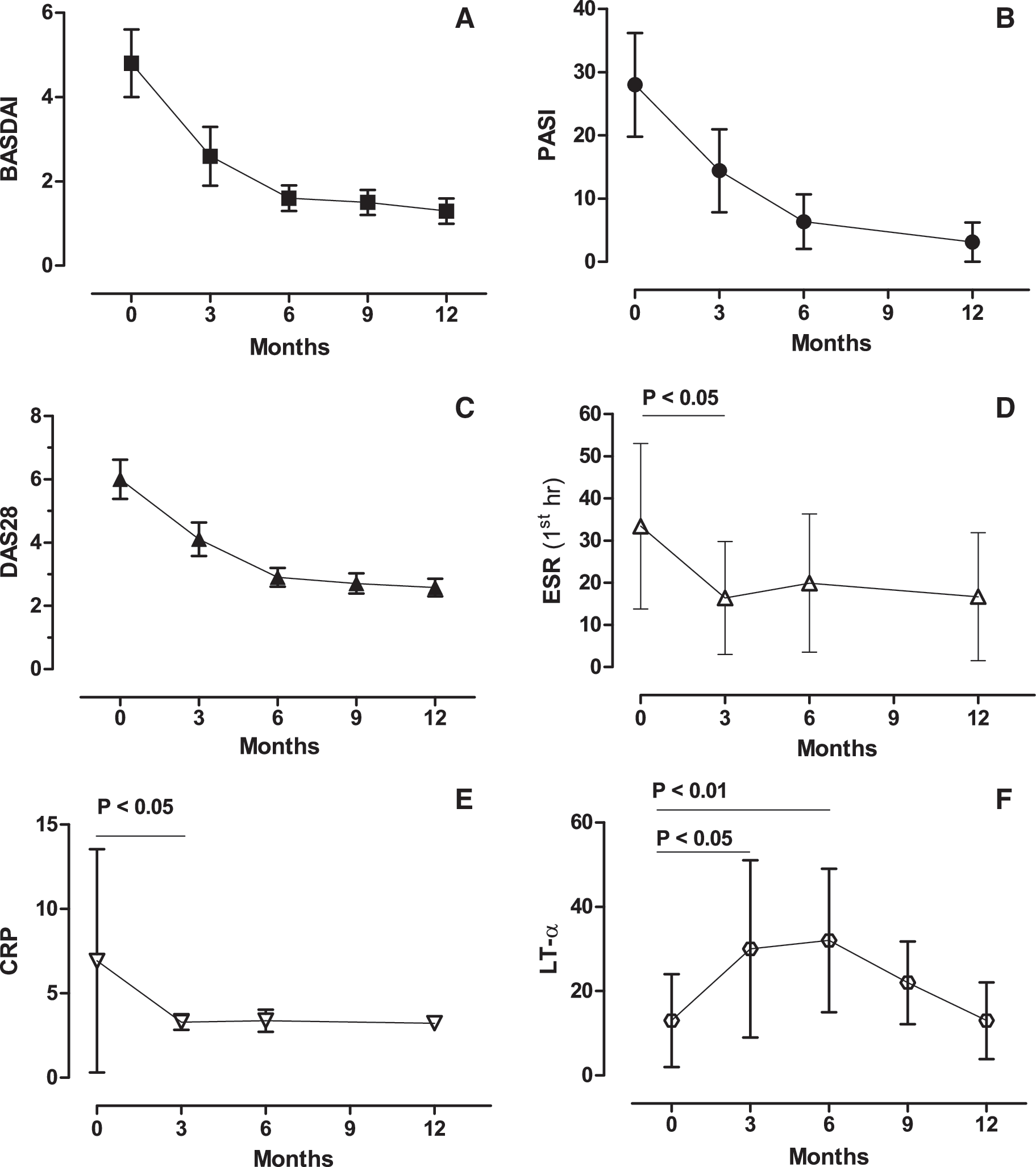
Change in Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Psoriasis Area Severity Index (PASI), and Disease Activity Score (DAS28)
Discussion
The data reported in the present study confirm that in PsA patients undergoing etanercept treatment, a significant reduction of inflammatory parameters and disease activity indexes is observed beginning from the 3rd and 6th month of therapy, respectively. However, the concurrent behavior of LT-α was somewhat unexpected. In fact, the LT-α serum levels significantly increased after 3 and 6 months of etanercept treatment and returned to baseline levels after 12 months of therapy. These data are in partial disagreement with previous studies performed in juvenile RA patients showing a mean decrease of LT-α serum levels during etanercept treatment (Gudbrandsdottir and others 2004; Bjørnhart and others 2005). However, considerable intra- and inter-individual variations in the LT-α serum levels were detected, and no significant association was found between the LT-α levels and clinical measures of disease activity, suggesting that a different distribution or metabolism of etanercept and natural TNFR may occur among patients. Moreover, these latter data cannot be directly compared with those obtained by us due to the different assays utilized to determine the LT-α concentrations. A tentative interpretation of these apparently inconsistent results could be the early formation of stable etanercept/TNF-α complexes, leading to an excess of free LT-α during the initial phase of etanercept treatment. This hypothesis implies that etanercept binds TNF-α with a faster and higher affinity than does LT-α. Pharmacological data indicating that the efficacy of etanercept in binding TNF-α is approximately 1,000-fold greater than that of the natural p75 receptor (Mohler and others 1993) could partially support this hypothesis. However, to the best of our present knowledge, data comparing the binding affinity of etanercept to TNF-α and LT-α are not available and, then, the interpretation of our findings that has been just provided remains theoretical. Regardless of the interpretation, the results of the present study denote that in PsA patients, the LT-α serum level does not correlate with the clinical and laboratory parameters of the response to etanercept and does not appear to affect the response to treatment at least in the first 6 months of therapy. This interpretation is in agreement with previous studies performed in RA patients in whom infliximab therapy had failed and who responded to etanercept treatment in which no differences were noted in the synovial and serum LT-α levels between responders and nonresponders (Buch and others 2007). In summary, the results of the present research indicate that in PsA patients responding to etanercept, an increase in the LT-α serum levels is observed at the beginning of treatment. Further investigation is required in order to better define the role of LT-α in PsA pathogenesis and the effect of the LT-α blockade with etanercept in PsA treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.