
Abstract
Patients with therapy-induced neutralizing antibodies (NAbs) to interferon-beta (IFN-β) have reduced responses to IFN-β treatment, resulting in higher relapse rates, increased magnetic resonance imaging activity, and a higher risk of disease progression. A functional assay was employed for both screening and titering of IFN-β NAbs utilizing a human cell line transfected with a luciferase reporter gene responsive to IFN-β. This assay demonstrated 100% sensitivity and specificity compared with the traditional cytopathic effect (CPE) assay and normal donor specimens. Additionally, 183 patients with multiple sclerosis (MS) undergoing therapy with IFN-β were tested in the reporter gene assay. Percent positivity for NAbs to the IFN-β was as follows: Avonex (1α) 26.5%, Rebif (1α) 34.1%, and Betaseron (1β) 31.8%. The IFN-β reporter gene assay showed excellent correlation with the well-established CPE assay offering clear advantages. The 50% false-positivity rate typically seen in enzyme-linked immunosorbent assays could be eliminated by using a functional assay for both screening and titering. Results can be reported within 20 h, and the cell line is cryopreserved, eliminating the need to maintain live viral and cell cultures. The use of this functional assay should be a valuable tool for detecting and monitoring the presence of NAbs in IFN-β-treated patients with MS.
Introduction
M
Viral neutralization assays are considered the gold standard for detecting antibodies to IFN-β. The cytopathic effect (CPE) assay is the most commonly used, but is laborious and time consuming to perform. Screening assays for binding antibodies (BAbs) to IFN-β are therefore usually performed and followed-up with viral neutralization assays (Pachner 2003; Pachner and others 2005; Sorensen and others 2005a). Studies have shown however that only about 50% of patients positive for BAbs are positive for NAbs as detected in the viral neutralization assays (Sorensen and others 2005a; Prince and others 2007).
In this study, we compared a functional cell-based IFN-β reporter gene assay to the traditional viral inhibition CPE assay, for both the screening and quantitation of therapy-induced NAbs in patients undergoing IFN-β treatment. Included in the study were 218 confirmed patients with MS either treated with IFN-β or undergoing no treatment, as well as 70 healthy controls. Additional parameters of the IFN-β reporter gene assay, including sensitivity, specificity, and reproducibility, were also evaluated.
Materials and Methods
Clinical samples
Sera were collected from patients with clinically definite multiple sclerosis (CDMS) under the Intermountain Multiple Sclerosis Project (IRB No. 00013382) (Brettschneider and others 2009; Rose and Carlson 2011). Only patients meeting CDMS defined by the McDonald criteria were included in this study (McDonald and others 2001; Polman and others 2005; Polman and others 2011). Exclusion criteria included active treatment with solumedrol, prednisone, or any other corticosteroids, as well as patients in active relapse. Patient demographics are given in Table 1. Normal controls were obtained from the ARUP Institute of Clinical and Experimental Pathology normal values study program IRB number 7740. Patients with MS were also classified by the type of IFN-β immunotherapy administered: (1) Avonex (IFN-β 1a), (2) Rebif (IFN-β 1a), (3) Betaseron (IFN-β 1b), and (4) no-immunotherapy group.
SD, standard deviation.
CPE assay
The CPE assay was performed by Focus Diagnostics (Cypress, CA), which first screens samples for the presence of BAbs using a capture enzyme-linked immunosorbent assay (ELISA) system (Pachner 2003; Prince and others 2007) before titering with the CPE assay. The CPE assay employs a lung carcinoma-derived epithelial (A549) cell line and an encephalomyocarditis virus (EMC) (Grossberg and others 2001a, 2001b, Prince and others 2007). A standard number of A549 cells was added and grown overnight in titration plates at 35°C in 5% CO2. Patient serum was diluted 1:20 and 1:100 and spiked with 10 laboratory units (LU) of IFN-β for 1 h and then placed into the A549 cell-containing titration plates and incubated overnight at 35°C in 5% CO2. A known amount of EMC virus was then added to each well and incubated again at 35°C in 5% CO2 overnight. The following day, the cells were stained using a dye, and the extent of CPE was determined spectrophotometrically. The titer that caused a 10-fold reduction (TRU) in the biological activity of the IFN-β from 10 to ≤1 LU is reported. One LU is defined as the amount of IFN-β that inhibits 50% of A549 cell infection (Perini and others 2004; Pachner and others 2005; Hartung and others 2007). The 3 reported titer results were <20 TRU, NAb negative; ≥20 but <100 TRU, NAb positive; and ≥100, NAb positive.
IFN-β reporter gene assay
The iLite™ anti-human IFN-β assay was obtained from Biomonitor Limited (Galway, Ireland). The assay utilizes a human PIL5 cell line carrying the luciferase reporter gene under the control of an IFN-responsive chimeric promoter (Lallemand and others 2008). If a patient is negative for neutralizing IFN-β antibodies, the spiked IFN-β will bind to its receptor on the cell, initiating the transcription of luciferase and the production of light through chemiluminescence. If a patient is positive for neutralizing IFN-β antibodies, the IFN-β is bound by the patient antibody and is, therefore, not free to bind to its receptor, resulting in an absence of luciferase signal generation. The cells were treated with vinblastin, an antimitotic drug, which allows the cells to be stored for up 18 months at −80°C without loss of IFN sensitivity or need for cultivation. The division-arrested cells also minimize assay variation associated with proliferation in culture. Similar reporter gene assays have been previously described, but differ by the lack of a division-arrested cryopreserved cell line as utilized here (Farrell and others 2008; Lam and others 2008; Farrell and others 2011).
Patient samples and controls are first heat-inactivated. An 8-point standard curve is made with concentrations from 80 to 0 LU/mL of IFN-β 1a. For screening, samples are diluted 1:20, either spiked or unspiked, with 25 IU/mL of IFN-β. The nonspiked well is used to control for endogenous levels of IFNs in the patient sample. Serum samples that reduce the activity of the spiked IFN-β concentration from 10 to 1 or less LU are considered positive and titered. The 1 LU/mL value is determined by plotting the relative luminescence unit (RLU) against the standard curve dilution (80–0 IU/mL) on a log–log scale on the x-axis. The linear portion of the curve is then calculated, and the corresponding IFN-β IU/mL value at the midpoint of the curve, 50% luminescence signal, is defined as 1 LU/mL. This is the cutoff value for positive and negative anti-IFN-β samples for the screening portion of the assay. Titering is performed using 3-fold dilutions starting at 1:20. Both the screening and titering can be setup in the same assay plate, using the same standard curve. Patient samples and controls are incubated with 25 IU/mL of IFN-β for 30 min at 37°C in 5% CO2 in a 96-well culture plate. The frozen cells are than rapidly thawed, added to the plate, and incubated for 18 h. Fifty microliters of Bright-Glo™ Luciferase substrate (Promega, Madison, WI) is then added, and the resulting signal is measured on a luminometer. In the titered samples, NAb titers are determined using the Kawade formula, t=f/n−1/9 (Kawade and Watanabe 1984; Kawade 1985), where f=the reciprocal of the antibody dilution a 1 LU, and n=the amount of IFN-β used in the assay as LU/mL, and t=TRU/mL. The TRU is the reciprocal of the antibody dilution that reduces IFN activity from 10 to 1.0 LU/mL, which is the reported value as recommended by the World Health Organization (Grossberg and others 2001a). A TRU of <20 is negative for the presences of NAbs; 20–99 suggests moderate levels of NAbs present; and a TRU of 100 or greater suggests high levels of NAbs.
Results
Comparison to the CPE assay
The IFN-β reporter gene assay had 100% diagnostic sensitivity [confidence interval (CI) 83.4%–100%) when compared with the traditional CPE assay, correctly identifying 25 out of 25 NAb-positive samples. Diagnostic specificity was also 100% (CI 83.4%–100%) identifying 58 normal controls as negative for NAbs (Table 2).
95% confidence interval (CI) was determined using the validated Web tool at
This tool was validated by Andrew Wilson, ARUP Institute Statistician.
IFN-β, interferon-beta; CPE, cytopathic effect.
Sensitivity and specificity of the IFN-β reporter gene cell line
Specificity studies showed that the IFN-β receptor was not reactive to high serum concentrations of 1,000 pg/mL of 11 nonrelated cytokines [interleukin (IL)-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12, IL-13, IL-18, and tumor necrosis factor-α). This was determined by spiking recombinant human cytokines in normal serum, and then comparing the RLUs of these samples to the unspiked sample. The mean RLUs of the spiked samples were all less than or equal to the mean RLU of the unspiked control, indicating that the cytokine-spiked samples did not generate signal above background. The IFN receptor of the transfected cell line was responsive to IFN-β, IFN-α, and IFN-γ, generating signal above the background in spiked samples down to 0.1 U/mL for all 3 types of IFNs. A comparison of the sensitivities of the PIL5 IFN transfected cell line to the 3 IFNs is shown in Fig. 1.
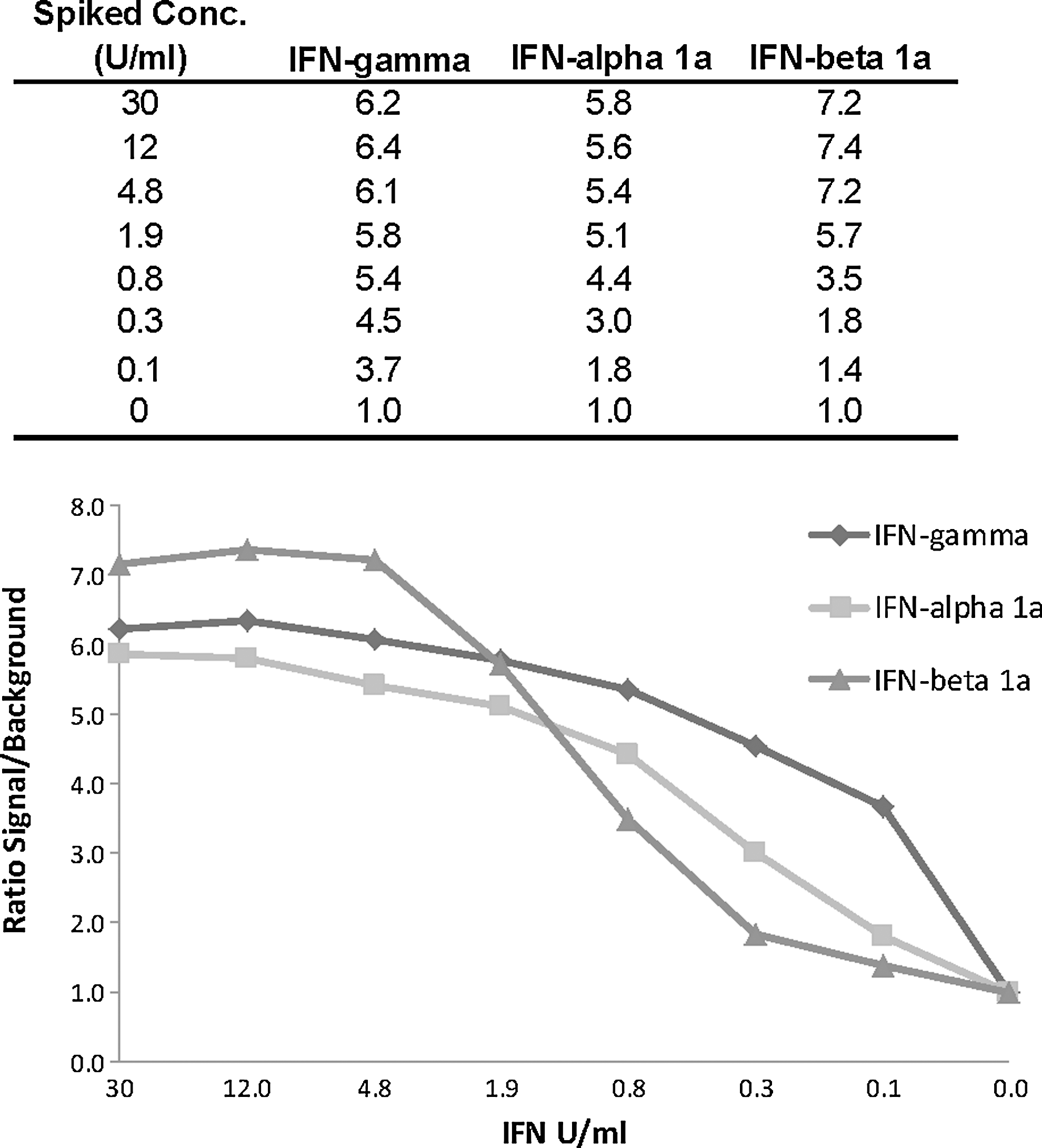
PIL5 interferon (IFN)-transfected cell line sensitivity to IFN-γ, IFN-α, and IFN-β reported in the ratio of signal to background.
Sensitivity of the reporter gene cell line to 3 different IFN-β treatments
The responsiveness of the reporter gene assay to the 3 most commonly administered IFN-β treatments, Avonex (IFN-β 1a), Rebif (IFN-β 1a), and Betaseron (IFN-β 1b), was examined by titering all 3 preparations (Fig. 2). All 3 preparations demonstrated very similar titration curves generating signal above background values for concentrations down to 0.1 IU/mL.
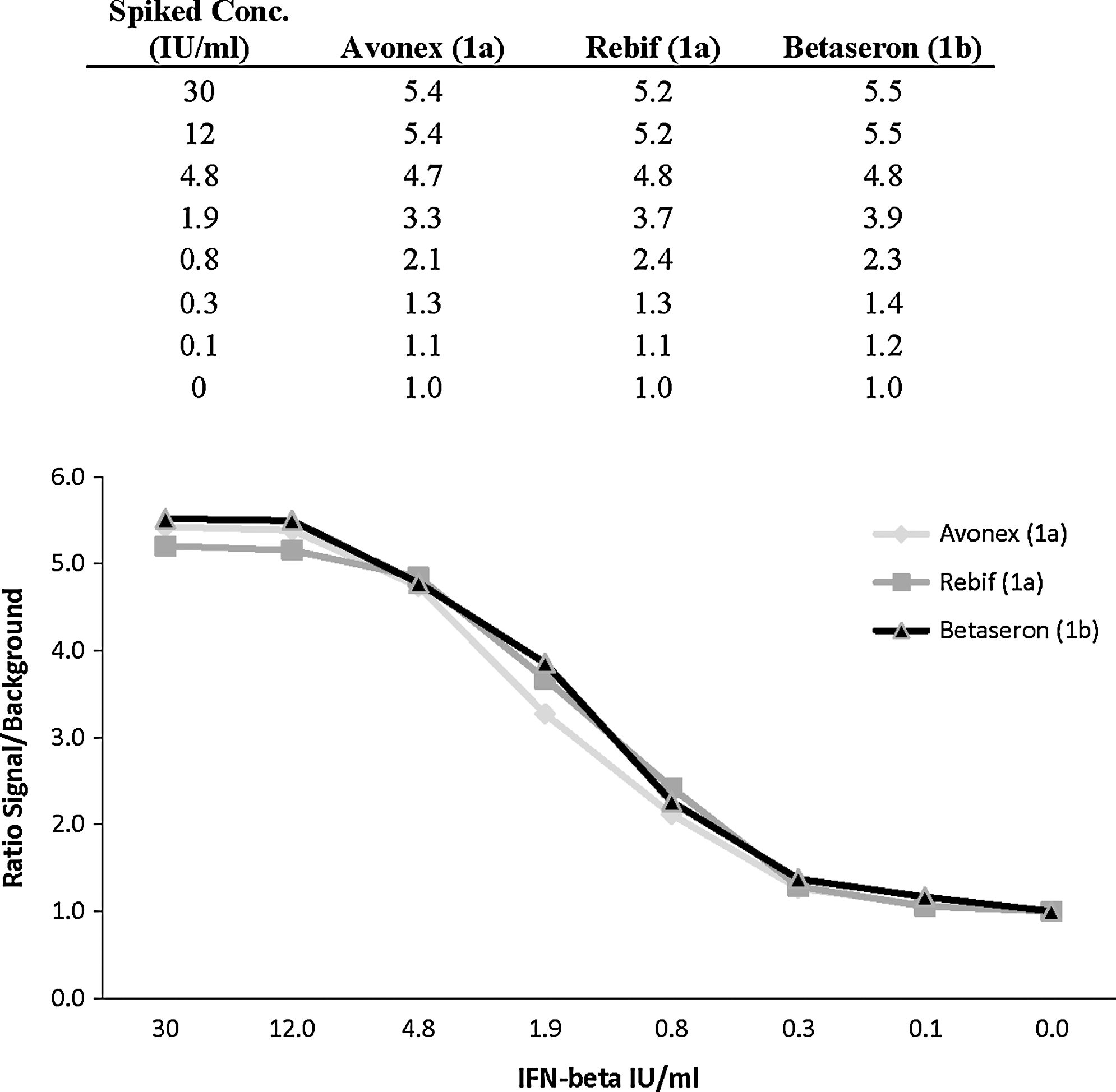
PIL5 IFN-transfected cell line sensitivity to the most common IFN-β treatments reported in the ratio of signal to background.
Precision studies
Precision of the IFN-β reporter gene-screening assay was determined by testing a positive patient pool and a negative single-donor sample in replicates of 3 on 3 separate days. Mean within run values for the negative sample ranged from 9.23 to 9.90 LU with percent coefficient of variation (%CV) ranging from 2.2 to 8.1. Positive screen sample values ranged from 0.26 to 0.51 LU with %CV ranging from 15.4 to 18.5. The %CV between runs was 5.9 for the negative sample, and 31.9 for the positive sample. The positive sample was also titered in replicates of 2, with a mean between-run value of 89.3 TRU and a %CV of 17.6.
Frequency of NAbs in IFN-β-treated patients with MS
Of the 183 patients with MS undergoing IFN-β therapy, 54 (29.5%) were positive for NAbs. Twenty-two of these patients had moderate levels of NAbs present (20–99 TRU), while 32 patients had high levels of NAbs (>100 TRU; see Table 3). Patients receiving Avonex (n=117) had the lowest NAb positivity at 26.5% with 13 patients having moderate and 18 patients having high TRU values. Positivity NAb rates for patients on Rebif (n=44) and Betaseron (n=22) were similar at 34.1% and 31.8%, respectively.
TRU, 10-fold reduction.
Discussion
The IFN-β reporter gene assay had 100% sensitivity and specificity when compared with the traditional CPE assay, correctly identifying 25 out of 25 samples as positive, and 58 normal controls as negative for NAbs. The CPE assay was performed in an independent laboratory in a blinded study.
The current gold standard for detecting antibodies to IFN-β is viral neutralization assays, the most commonly used being the CPE assay. Due to these assays being laborious, time consuming, and difficult to standardize, a screening assay for BAbs is usually performed in conjunction with viral neutralization assays (Pachner 2003; Pachner and others 2005; Sorensen and others 2005a). BAbs against IFN-β are induced in a majority of treated patients, but have no clinical significance, and only a subset of BAb-positive patients develops Nabs, which may result in a loss of drug bioactivity (Malucchi and others 2004; McKay and others 2006; Hartung and others 2007). Studies have shown however that only about 50% of patients positive for BAbs are positive for NAbs in the viral neutralization assay (Sorensen and others 2005a; Prince and others 2007). Furthermore, solid-phase screening assays, such as ELISA, may give false-negative results due to conformational changes of the epitope caused by the direct binding of IFN-β to the well (Pachner 2003). These limitations make the utility of a screening assay less than ideal. We used the IFN-β reporter gene assay to both screen directly for NAbs on all patient samples and also to titer the activity. We have set the cutoff value for the screening assay lower than the titering assay to assure that no low-positive samples are missed. Even so, >95% of screen-positive samples were positive upon titering when using this method. As the titering portion of the assay starts with the same dilution used by the screening assay, it allows for confirmation of the original positive screen result.
The human PIL5 cell line transfected with an IFN-regulated luciferase reporter gene employed in this assay is responsive to both recombinant human type I IFN (IFN-α and IFN-β) as well as type II IFN IFN-γ. Under the current conditions optimized for IFN-β, our studies showed that the transfected cell line had the best dynamic response to IFN-β, followed by IFN-γ and IFN-α with sensitivities being greater for IFN-γ, and about equal for IFN-β and IFN-α at 0.1 U/mL (Fig. 1). If properly optimized, this transfected cell line may be useful in measuring NAbs to Roferon and Intron A, two IFN-α preparations commonly administered for hepatitis C treatment, as well as IFN-γ, which is used in the treatment of is chronic granulomatous disease and osteopetrosis.
Titration curves generated using Avonex (IFN-β 1a), Rebif (IFN-β 1a), and Betaseron (IFN-β 1b) demonstrated that the transfected cell line was equally sensitive to the most commonly administered IFN-β treatments (Fig. 2).
The frequency of NAbs to the 3 most commonly used IFN-β products in the United States, Avonex, Rebif, and Betaseron, varies by the type of IFN-β preparation used as well as the frequency and site of injection. Studies have shown that IFN-β 1b (Betaseron) is the most immunogenic of the 3 preparations, possibly due to its lack of glycosylation, as it is produced in modified Escherichia coli. The frequency of NAbs in patients undergoing Betaseron treatment ranges from 25% to 40% in clinical studies (Bertolotto and others 2000; Ross and others 2000; Fernandez and others 2001; Bertolotto and others 2002; Pachner 2003; Bertolotto and others 2004; Perini and others 2004; Pachner and others 2005; Ross and others 2006). Both Avonex and Rebif (IFN-β 1a) are recombinant proteins produced by mammalian cells, and subsequently have lower reported incidences for the development of NAbs, 2%–7% for Avonex, and 15%–25% for Rebif (Bertolotto and others 2000; Ross and others 2000; Fernandez and others 2001; Bertolotto and others 2002; Pachner 2003; Bertolotto and others 2004; Perini and others 2004; Pachner and others 2005; Ross and others 2006). In our study, the Avonex-treated group (n=117) had a higher incidence of NAbs (26.5%) when compared to that reported in the literature. Only NAb titers of ≥100 TRU, however, have been consistently correlated to loss of therapeutic IFN-β efficacy (Perini and others 2004; Pachner and others 2006; Hartung and others 2007). In our Avonex-treated study group, 15.3% of patients had NAbs of ≥100 TRU. NAbs in Rebif-treated patients (n=44) showed a higher incidence (34.1%) than those treated with Betaseron (31.8%, n=22), though the differences were not statistically significant. The reason for the higher incidences of NAbs in our study population may be that the majority of subjects are patients with long-term MS. The mean disease duration for our Avonex-treated groups was 11.9 years for women, and 10.0 years for men. The mean treatment duration of the Avonex group for both men and women was 5.0 years (standard deviation 2.3).
In summary, the IFN-β reporter gene assay showed excellent correlation with the well-established CPE assay. Results can be reported within 20 h compared to 4–5 days for the CPE assay. The assay utilizes a well-characterized and cryopreserved cell line, eliminating the need for the constant maintenance of live cell and viral cultures, and their inherent variability. Patient samples can be screened and titered for NAbs in the same assay, greatly reducing the number of false-positive results observed with the current BAb screening assays. The use of this reporter gene assay should be a valuable tool for the monitoring of IFN-β-treated patients with MS for the presence of NAbs, leading to more effective therapeutic regimens.
Footnotes
Author Disclosure Statement
No competing financial interests exist.