
Abstract
Multiple sclerosis (MS) is the most common prototypic inflammatory demyelinating disease. Neuromyelitis optica (NMO) is another inflammatory demyelinating disease of the central nervous system that exhibits clinical symptoms mainly associated with optic neuritis and myelopathy. The inflammatory reaction in MS is associated with an upregulation of a variety of T helper 1 (Th1)- or Th17-mediated cytokines. However, NMO and MS are intertwined both clinically and pathologically, which complicates their diagnosis and treatment. The aim of this study was to evaluate the differences in serum cytokine levels in patients with NMO and MS. We collected peripheral serum from patients with these central nervous system demyelinating diseases for the study. A cytometric bead array was used to assess the cytokine levels using flow cytometry. We found more inflammatory [interleukin (IL)-2 and interferon-γ) and anti-inflammatory (IL-4 and IL-10) cytokines in NMO than in MS. The differences in the optimal cutoff points of serum cytokines, including IL-2 ≥5 pg/mL, can differentiate NMO from MS. In conclusion, patients with NMO had an increased Th1-mediated inflammatory response, but similar Th17-mediated inflammation changes compared to patients with MS. Serum cytokine studies can differentiate NMO cases from MS.
Introduction
M
The primary effector T cell in the pathology of MS was originally thought to be a CD4+ T helper 1 (Th1) cell (McFarland and others 1992; Adorini and Trembleau 1997; Sinigaglia and others 1997). The inflammatory reaction in MS is indeed associated with upregulation of several Th1-mediated cytokines, including interleukin (IL)-2, interferon (IFN)-γ, and tumor necrosis factor (TNF)-α (Aktas and others 2009). In contrast, CD4+ T helper 2 (Th2) cells produce IL-4, IL-6, and IL-10 to mediate Ab production, and downregulate Th1 cellular responses (Adorini and Trembleau 1997). Thus, one of the major goals of IFN-β treatment for MS is to shift the Th1 response to the Th2 response to improve the patient's prognosis (Nicholson and Kuchroo 1996; Kozovska and others 1999). MS has also been considered by some as a CD4+ T helper 17 (Th17) cell-mediated disease recently, but the matter is still under debate (Matusevicius and others 1999). NMO with Ab and complement activation is considered as a humoral response (ie, Th2 cells) predominates (Correale and Fiol 2004), although a major controversy exists with regard to this particular point of view. It has been suggested that NMO is instead a Th1- or Th17-predominated disease (Horiuchi and others 2000; Wu and others 2000; Li and others 2011). To investigate this issue, we conducted a study to survey the cytokine changes that occur in both MS and NMO.
Materials and Methods
Patients
Eighty patients with central nervous system (CNS) demyelinating disorder with a history of more than 2 relapses and followed up at the MS Clinic in Taipei Veterans General Hospital, Taipei, Taiwan, from 2007 to 2008 were consecutively enrolled in our study. The final diagnosis was made according to the continuous 2-year clinical and serial imaging follow-up. At last, a total of 34 patients fulfilled the diagnostic criteria of NMO (Wingerchuk and others 2006). Briefly, optic neuritis and acute long-spinal-cord myelitis (>3 segments), but without traditional MS imaging patterns, constituted the diagnosis of NMO. Exclusion criteria included Sjögren's syndrome or systemic lupus erythematosus-related neurological disorder, recurrent myelitis, or recurrent optic disease. Twenty-four patients were found to have MS using the Poser criteria with 2 clinical attacks, and by not fulfilling the diagnosis of NMO and related disorders (Poser and others 1983). The remaining 20 patients were excluded because of an uncertain diagnosis of NMO or MS based on the clinical course, such as recurrent optic neuritis or myelitis. Thirty healthy controls were also enrolled. Blood samples were drawn at the initial enrollment and >1 month after any previous episode, that is, during disease remission. Since circulating adhesion molecules and inflammatory cytokines were greatly elevated during the acute phase of the demyelination process, whether in MS or NMO (Moreau and others 1996; Li and others 2011), we wanted to clarify the state of cytokine expression during remission, to provide distinguishable data for reference.
This study was approved by the Institutional Review Board of Taipei Veterans General Hospital. All patients were subjected to a thorough neurological examination, routine laboratory tests, and clinical evaluation at regular intervals in the clinic. Clinical characteristics of the patients, including current age, age at symptom onset, and annual relapse rate, were recorded and analyzed together with the results of the Expanded Disability Status Scale (EDSS) disability score at the 2-year follow-up.
Anti-AQP4 study method
Sera were harvested and stored at −20°C. Serum AQP4 Ab was detected using a cell-based assay with AQP4-transfected HEK293 cells, as previously described by Matsuoka and others (2007).
Cytometric bead array immunoassay of Th1, Th2, and Th17 cytokines
Serum samples were stored at −80°C for the cytometric bead array (CBA) analysis. The CBA technique is based on microparticles, which are dyed to 7 different fluorescence (FL) intensities, matched with Abs. The dye has a maximum emission wavelength of ∼650 nm (FL-3). The particles were matched by covalent linkage with Abs (Pharmingen, SanDiego, CA) against each of the 7 cytokines (IFN-γ, TNF-α, IL-2, IL-4, L-6, IL-10, and IL-17). The Ab particles served to capture each cytokine, and the cytokines were directly detected using an immunoassay with 7 different Abs matched with phycoerythrin (PE), which emits at 585 nm (FL-2). The PE-conjugated detector Ab was used to complete the sandwich, and the medium intensity in FL-2 was proportional to the concentration of the cytokine in the sample, which was quantified using a calibration curve. Seven standard curves (ranging from 0 to 5,000 pg/mL) were obtained from the set of calibrators, and 7 results were obtained for test samples.
Serum samples from the MS and NMO controls were incubated with each Ab-bead reagent and Ab-PE detector in the dark at room temperature for 160 min, briefly washed, and subjected to flow cytometry for data acquisition. Two-color cytometric analysis was carried out using an FACSCaliber flow cytometer (BD Biosciences) in the Medical Institute of the National Defense Medical Center, Taipei, Taiwan. Data were obtained and analyzed with CBA software.
Statistical interpretation
Due to the small sample size in the 2 disease groups, including MS (n=24) versus NMO (n=34) and NMO with IFN (n=20) versus NMO without IFN (n=14), continuous data were presented using the median and interquartile range (the range between the 25th and 75th percentile), and the differences between the 2 groups were tested with the nonparametric Mann–Whitney test. Categorical data were all presented using count and percentage, and the differences between the 2 groups were tested with the Fisher's exact test. The associations between the cytokines and the disease groups were described using odds ratios (ORs) with 95% confidence intervals (CI) from the univariate logistic regression analyses, and multivariate logistic regression analyses were conducted to evaluate the independent associations, controlling for EDSS score and annualized relapse rate. The area under the receiver operating characteristic (ROC) curve (AUC) was determined to evaluate the diagnostic value of the cytokines, and the optimal cutoff point of the ROC curves was determined using the Youden index (sensitivity+specificity −1). A P value<0.05 represented statistical significance for all statistical hypothesis tests. Statistical analyses were performed using SPSS 15.0 software (SPSS, Inc.).
Results
Baseline characteristics
The 24 patients with MS, 4 men and 20 women, had a median age of 42.0 years, and the 34 patients with NMO, 2 men and 32 women, a median age of 47.0 years. There was no significant difference in age or gender between the patients with MS and patients with NMO. The patients with NMO had significantly higher EDSS scores and annualized relapse rates than the patients with MS (median EDSS: 4.5 versus 2.5, P=0.001; annualized relapse rate: 1.0 versus 0.6, P<0.001). No significant difference was observed in the treatment of IFN between the 2 disease groups. In addition, 15 (44.1%) patients with NMO, but no patients with MS, were positive for AQP4 Ab (P<0.001) (Table 1). The 30 enrolled healthy controls included 1 man and 29 women, with a median age of 43.0 years, and none showed the existence of AQP4 Ab.
Indicates a significant difference as compared to the MS patients.
MS, multiple sclerosis; NMO, neuromyelitis optica; IFN, interferon-β.
Serum concentration of cytokines
Patients with NMO had significantly higher levels of serum concentrations of IL-4 and IL-10 than patients with MS (median IL-4: 3.6 versus 0 pg/mL, P=0.013; median IL-10: 7.0 versus 2.9 pg/mL, P=0.038) (Fig. 1A). Patients with NMO also had significantly higher levels of serum concentrations of IL-2 and IFN-γ than patients with MS (median IL-2: 5.4 versus 0 pg/mL, P=0.006; median IFN-γ: 6.4 versus 0 pg/mL, P=0.019). No significant difference was observed in TNF-α and IL-17 levels (Fig. 1B). However, the cytokine surveys in both groups showed significantly higher levels than those of the healthy controls (Supplementary Table S1; Supplementary Data are available online at
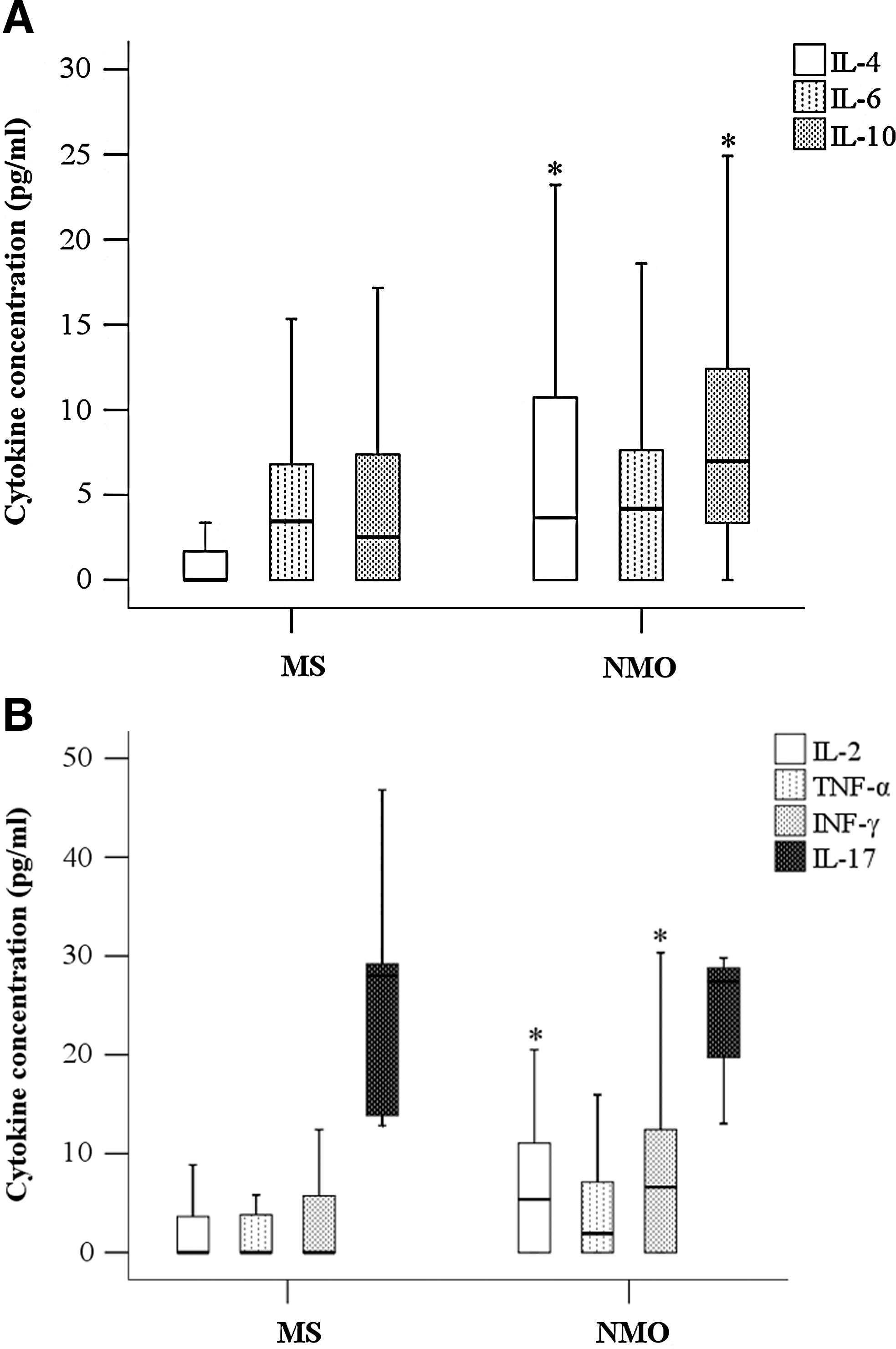
Analysis of serum cytokines of multiple sclerosis and neuromyelitis optica (NMO).
Associations between cytokines and diseases
The univariate logistic study showed that both gender and age were insignificant predictors for MS/NMO. The 4 ORs in the univariate logistic regression analyses of IL-4 (OR=1.14), IL-10 (OR=1.10), IL-2 (OR=1.24), and IFN-γ (OR=1.12) reached a statistically significant level. In the multivariate analyses, independent associations with the disease groups were observed for the IL-2 and IFN-γ cytokines, which implies that those with higher levels of IL-2 and IFN-γ were more likely to have NMO, rather than MS, at the same EDSS and annualized relapse rate, with ORs of 1.36 and 1.15. (Table 2).
With adjustments for annualized relapse rate and EDSS.
Female as reference group.
Indicates a significant odds ratio, implies those with higher levels of the corresponding variable were more likely to be NMO patients.
Diagnostic value of cytokines
The AUC for diagnosing NMO by IL-2 reached 0.701, with a 95% CI of 0.566–0.814, and that by IFN-γ was 0.674 with a 95% CI of 0.538–0.791, and that by IL-2 and IFN-γ together was 0.7000 with a 95% CI=0.551–0.854 (Fig. 2).
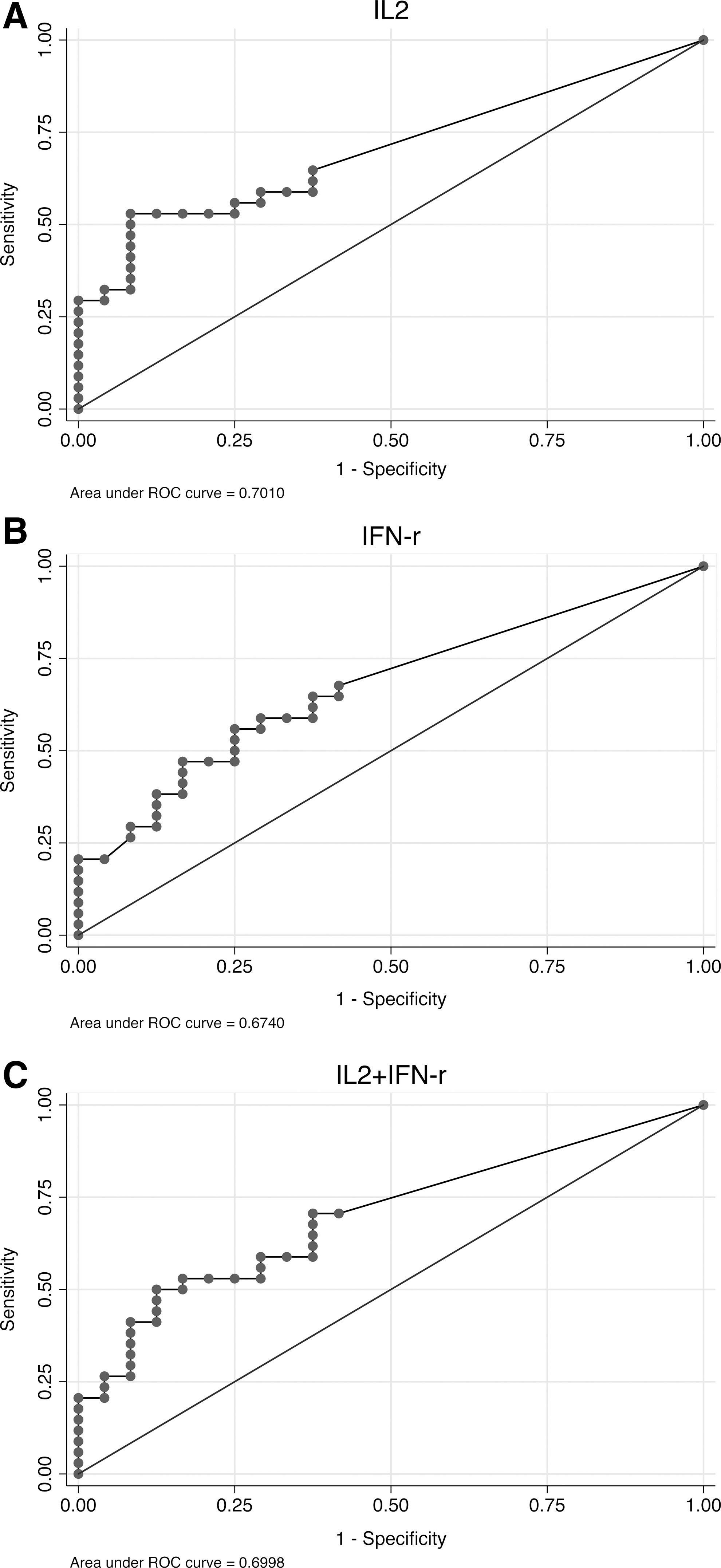
The area under the receiver operating characteristic (ROC) curves (AUC) for diagnosing NMO by cytokine.
The optimal cutoff points of IL-2 ≥5 pg/mL and IFN-γ ≥6 pg/mL were determined by the Youden index. Sensitivity reached 52.9% when using the optimal cutoff points of IL-2 and IFN-γ (ie, 18 of the 34 patients with NMO would be detected), which was higher than the 44.1% when using the AQP4 Ab. Specificity was 91.7% and 75.0% when using the optimal cutoff points of IL-2 and IFN-γ (ie, 22 and 18 of the 24 patients with MS would be detected), which was lower than the 100% when using the AQP4 Ab. Positive predictive values (PPVs) of IL-2 ≥5 pg/mL and IFN-γ ≥6 pg/mL were lower than that of AQP4 Ab (90% and 75% versus 100%). The negative predictive value (NPV) of IL-2 <5 pg/mL was lower than that of AQP4 Ab (42.1% versus 44.2%), but the NPV of IFN-γ <6 pg/mL was higher than that of AQP4 Ab (47.1% versus 44.2%) (Table 3). Furthermore, the combination of IL-2 ≥5 pg/mL and IFN-γ ≥6 pg/mL as a cutoff point showed an 88.9% PPV, but a higher (55.0%) NPV, compared to the others.
The optical cutoff point was determined by the Youden index (sensitivity + specificity −1).
PPV, positive predictive value; NPV, negative predictive value.
Comparisons between the use and nonuse of IFN in patients with NMO
There is a lot of debate about the use of IFN treatment in NMO. Thus, our patients with NMO were divided into 2 groups, those with (n=20) and without (n=14) IFN treatment, to compare the clinical pictures and related cytokine changes. There was no significant difference in age, gender, or annualized relapse rate between the 2 groups. However, a higher EDSS was noted in the NMO-with-IFN treatment group. The patients with NMO using IFN had significantly higher levels of IL-17 cytokines (median IL-17: 28.8 versus 20.2 pg/mL), but lower levels of IL-2 cytokines (median IL-2: 3.0 versus 11.1 pg/mL) than those not using IFN (Table 4).
Indicates a significant difference between the 2 groups.
IFN−, without IFN use; IFN+, with IFN use.
IL-6 correlated with EDSS in NMO
We found that the initial IL-6 expression correlated well with the later EDSS scores in the NMO group (Fig. 3).

The initial IL-6 expression correlated well with the later Expanded Disability Status Scale scores in the NMO group.
Discussion
In this study, we found increased inflammation in patients with NMO compared to patients with MS, based on a survey of serum cytokine levels. Mutual participation of Th1, Th2, and Th17 cytokines was found in both patient groups in the analysis. In general, proinflammatory (IL-2 and IFN-γ) and anti-inflammatory (IL-4 and IL-10) cytokines were increased in patients with NMO compared to patients with MS. Furthermore, we could use the optimal cutoff point of IL-2 ≥5 pg/mL to differentiate NMO cases from MS cases in the serum cytokine survey.
The levels of all study cytokines in each group were significantly higher than in the controls, indicating the mutual participation of Th1, Th2, and Th17 responses in NMO or MS. This supports past findings and suggests the complexity of autoimmune diseases with the involvement of multiple mechanisms (Amerio and others 2002), and also supports the involvement of IL-17 in the pathogenic mechanisms of NMO (Li and others 2011; Wang and others 2011a), which may be considered as a spectrum of MS. However, in our study, the Th17 response showed no significant change in these 2 diseases; therefore, we plan to perform future extensive studies, including a study of TH17-associated cytokines, to differentiate NMO from MS.
Inflammatory mechanisms play an important role in MS lesions. For example, the overexpression of several proinflammtory cytokines, such as IFN-γ, is reportedly related to attacks that occur in patients with MS (Frohman and others 2006; Ubogu and others 2006). A correlation between EDSS scores and IFN-γ levels was noted in a previous MS study (Petereit and others 2000). The observation regarding our patients with NMO is consistent with that of reports of clinically frequent recurrent disease and disabilities more severe than MS (Chan and others 2009). The increased IFN-γ levels in our patients with NMO accounted for their greater clinical severity compared to patients with MS. The increased inflammation in patients with NMO suggests that clinicians should use more potent anti-inflammatory drugs and/or more intense treatment for NMO than for MS.
NMO expressed more humoral/Th2 responses, compared to MS, with elevated IL-4 and IL-10 levels. Existing evidence shows that both T-cell subsets and B cells can induce autoimmunity in the CNS (Caspi and others 2008; McLaughlin and Wucherpfennig 2008). Abs to both myelin–oligodendrocyte glycoprotein and myelin basic protein in the serum of patients with MS (Wajgt and Gorny 1983; Bernard and de Rosbo 1991) and AQP4 Ab in NMO patients are particularly expressed (Wingerchuk 2006). The humoral response involved in NMO is not only documented from serum study, but also supported by the clinical evidence of a good response to plasma exchange (Watanabe and others 2007; Wang and others 2011b).
Some reports suggested that IFN was not effective in reducing the relapse number and the disability progression in NMO (Tanaka and others 2009; Uzawa and others 2010). IFN may even trigger severe exacerbation in NMO cases (Warabi and others 2007), and increase the production of AQP4 Ab (Palace and others 2010). Our study found increased EDSS scores in our patients with NMO using IFN, consistent with past reports. The patients with NMO with elevated IL-17 and using IFN had more disability, compatible with recent reports that a higher IL-17 level is associated with nonresponsiveness to IFN treatment. (Axtell and others 2010).
Furthermore, we found that the IL-6 concentration correlates even more with the EDSS score in NMO (Fig. 3). It has previously been shown that elevated IL-6 was found in the cerebrospinal fluid of patients with NMO (Hamnik and others 2008; Uzawa and others 2009). IL-6 is a proinflammatory cytokine secreted by Th2 cells that causes potent B cell stimulation (Diehl and Rincon 2002; Correale and Fiol 2004). These findings collectively imply that IL-6 may be a candidate biomarker for active CNS autoimmune inflammatory diseases, especially in NMO.
The immunopathogenesis of both MS and NMO has been shown to be heterogeneous. As such, the results of our ROC analysis herein indicate that the optimal cutoff points of IL-2 ≥5 pg/mL may represent a good biomarker for discriminating NMO from MS. Such a biomarker may provide physicians with an overall direction, even without using AQP4 Ab or NMO IgG, when diagnosing NMO.
However, there are some limitations to our study. First, the titer of AQP4 Ab was not investigated in our study; thus, we could not correlate the level of cytokines with the titer of AQP4 Ab, which may be of benefit in studying the role of AQP4 Ab in NMO. Second, we did not check the cytokine changes during the active attack period compared to usual, which could provide more clues about the dynamic change. Third, the sample size in this study was small, but did demonstrate significant inflammatory responses in NMO. In the future, we plan to collect more study subjects to seek out more clues to help differentiate these 2 diseases at the outset.
CNS inflammatory demyelinating disease represents a broad spectrum of disorders, including prototypic MS, NMO, Balo's concentric sclerosis, and several others. There are many symptomatic similarities among these disorders, leading to uncertainty in the clinical diagnosis and even diverseness in treatment. Our study has shed some light on the underlying difference between MS and NMO, and thereby may be of help in providing more effective treatment.
In conclusion, the NMO patient group showed increased inflammation, and an anti-inflammatory response, compared to the MS patient group. Furthermore, the serum cytokine study suggested that the presence of IL-2 ≥5 pg/mL in patients with these CNS demyelinating disorders can differentiate NMO cases from MS when clinically obscure at the initial. It is our hope that our present finding, in combination with the findings of inflammatory inhibitors, might facilitate greater clinical efficacy in treating NMO by modifying the underlying immune response.
Footnotes
Acknowledgments
This work was supported by Research Grants of the Cheng Hsin General Hospital, Taipei, Taiwan.
Patient Consent
We confirm that we obtained patient consent.
Provenance and Peer Review
Not commissioned; externally peer reviewed.
Author Disclosure Statement
We declare no competing financial interests exist.