
Abstract
Until now, no study has evaluated CXCL9 in hepatitis C virus (HCV) infection-related mixed cryoglobulinemia (MC) patients in presence/absence of autoimmune thyroiditis (AT). Serum CXCL9 and CXCL10 have been measured in 60 patients with MC (MCo), in 35 patients with MC and AT (MC-AT), in sex and age-matched controls: 60 healthy (Control 1); 35 patients with AT without cryoglobulinemia (Control 2). CXCL9 and CXCL10 were higher in MC-AT patients than Control 2 (P<0.0001) and MCo (P=0.01), in MCo than Control 1 (P<0.0001), and in Control 2 than Control 1 (P<0.001). By defining a high CXCL9 level as a value>2 SD above the mean value of the Control 1 (>122 pg/mL), 5% of Control 1, 34% of Control 2, 91% of MCo, and 97% of MC+AT had high CXCL9 (P<0.0001, chi-square). By simple regression analysis CXCL9 and CXCL10 were related to each other in MCo (r=0.426, P=0.001) and in MC-AT (r=0.375, P=0.001). We first demonstrate high serum levels of CXCL9 in cryoglobulinemic patients, especially with AT. Further, a strong association between serum CXCL9 and CXCL10 has been observed in patients with MC in presence/absence of AT.
Introduction
M
Recent evidence has shown that CXC alpha-chemokines (Th1), especially CXCL10, have a key role in mixed cryoglobulinemia (MC), in particular in MC patients with active vasculitis (Antonelli and others 2008d).
Moreover, CXCL10 has an important role in the initial phases of autoimmune thyroiditis (AT), as it is elevated in patients with newly diagnosed AT, especially in the presence of a more aggressive thyroiditis and hypothyroidism (Antonelli and others 2004c).
We have previously demonstrated that autoimmune thyroid disorders are frequently present in cryoglobulinemic patients (Antonelli and others 2004a). Further, it has been suggested that the basis of this association could be linked to the activation of a Th1 immune response, as high levels of the Th1 CXCL10 chemokine are present both in patients with MC-AT such as in patients with MC alone (Antonelli and others 2008b, 2008c).
To our knowledge, CXCL9 has not been evaluated in patients with MC (and vasculitis), while few studies have suggested the involvement of CXCL9 in AT (Kimura and others 2004; Antonelli and others 2009a, 2009d, 2010a, 2011a, 2011b).
Therefore, in this study we measured serum CXCL9 levels, in comparison with CXCL10, in a large sample of cryoglobulinemic patients with/without AT, with respect to normal controls.
Materials and Methods
Patients with MC without AT (MCo)
Sixty MC patients were recruited into the study, who consecutively referred to the Rheumatology Unit of the University of Modena. The diagnosis of MC was done evaluating the presence of a specific core set of clinical and laboratory parameters, and the presence of serum mixed (IgG-IgM) cryoglobulins (Ferri and others 2002; Ferri 2008). Hepatitis C virus (HCV) infection was systematically evaluated in all patients (HCV-negative patients were excluded). MC+HCV subjects without liver cirrhosis (by histology, laboratory evidence of liver damage, and/or ultrasound-proven portal hypertension) (Antonelli and others 2004b, 2005) and without hepatocellular carcinoma, and in whom the presence of associated thyroid autoimmune disorders were excluded [after a thyroid screening evaluating history, physical examination, thyroid-stimulating hormone (TSH), free triiodo-thyronine (FT3), free thyroxine (FT4), antithyroglobulin (AbTg) and antithyroperoxidase (AbTPO) antibodies measurements, and ultrasonography], were included in this group.
Table 1 reports the main demographic and clinicoserological features of MC patients. Among them, 25 had been previously treated with IFN-alpha [average 6.5 months (range 1–12), mean dosage 11 MU/week (range 3–7); time elapsed from the last IFN-alpha treatment 4–75 months (mean 39)]. No statistically significant difference was observed in the main demographic and clinicoserological features of MC patients treated or untreated with IFN-alpha.
No significant difference was observed about the undermentioned characteristics in the 2 groups.
Serum creatinine >1.5 mg/dL and/or proteinuria >0.5 g/24 h.
Increase of the liver enzyme ALT and/or histological alterations.
MC, mixed cryoglobulinemia; AT, autoimmune thyroiditis.
Forty-two MC patients were taking corticosteroids (≤5 mg/day of prednisone equivalents) during the study, while 5 had previously been treated and 13 had never been treated. No MC patient had had plasma exchange treatment in the last year before the study. The presence of Raynaud's phenomenon, secondary Sjogren's syndrome, skin ulcers, peripheral neuropathy, and renal and liver involvement in MC patients was evaluated as previously described (Ferri and others 2002; Ferri 2008), such as routine blood chemistry (Antonelli and others 2004a).
Patients with MC and AT (MC-AT)
Thirty-five MC patients were recruited into the study, who consecutively referred to the Rheumatology Unit of the University of Modena and in whom a thyroid screening (see above) revealed the presence of thyroid autoimmune disorders.
Table 1 reports the main demographic and clinicoserological features of MC patients. Among them, 12 had been previously treated with IFN-alpha [average 5.4 months (range 1–13); mean dosage 10 MU/week (range 3–7); time elapsed from the last course of IFN-alpha treatment 3–76 months (mean 41)]. No statistically significant difference was observed in the main demographic and clinicoserological features of MC patients treated or untreated with IFN-alpha.
Twenty-six MC patients were taking corticosteroids (≤5 mg/day of prednisone equivalents) during the study, 3 had been previously treated and 6 had never been treated. No MC-AT patients had had plasma exchange treatment in the last year before the study.
Controls
Two control groups were evaluated, who were extracted from a random sample of the general population from the same geographic area (Antonelli and others 2005), coupled by sex and age with MC patients, without HCV infection or other liver disorders.
Control 1 involved 50 subjects (41 females and 9 males; age, 60±11 years), in whom a complete thyroid screening excluded the presence of thyroid or autoimmune disorders, or any kind of immunomodulant therapy.
Control 2 consisted of 40 subjects (33 females and 7 males; age, 61±12 years), in whom a complete thyroid screening demonstrated the presence of thyroid autoimmune disorders, but excluded the presence of other autoimmune disorders and any kind of immunomodulant therapy.
A blood sample was collected in the morning in all patients and controls, after overnight fasting.
Informed consent was obtained from all patients and controls, and the study was approved by the local Ethical Committee.
Laboratory studies
Cryocrit, cryoglobulin composition, C3-C4 fractions were measured as previously described (Ferri 2008; Antonelli and others 2012); antinuclear, antismooth muscle, and antimitochondrial autoantibodies were detected by current techniques (Ferri 2008; Antonelli and others 2012). Sera with a titer >1:80 were considered positive. Antiextractable nuclear antigen antibodies, including anti-Scl70, anti-Sm, -RNP, -SSA/SSB, -PCNA, -SL, and -Jo1 specificities, were detected by counter-immunoelectrophoresis (Antonelli and others 2004a, 2009b, 2012).
Anti-HCV antibodies and HCV RNA were determined as previously reported (Zignego and others 1990; Ferri and others 1993; Antonelli and others 2012).
Thyroid evaluation, thyroid blood flow, FT3, FT4, TSH, AbTPO, and AbTg determination, were performed as previously described (Antonelli and others 2004c).
Circulating CXCL9 levels were measured by a quantitative sandwich immunoassay commercially available kit (R&D Systems, Inc., Minneapolis, MN; sensitivity 1.1–10.2 pg/mL; mean minimum detectable dose 3.2 pg/mL; intra- and inter-assay coefficients of variation 4.0% and 7.1%).
Circulating CXCL10 levels were measured by a quantitative sandwich immunoassay commercially available kit (R&D Systems; sensitivity 0.40–4.51 pg/mL; mean minimum detectable dose 1.71 pg/mL; intra- and inter-assay coefficients of variation 2.9% and 6.4%).
Data analysis
Normally distributed variables are given as mean±SD, otherwise as median and interquartile range. One-way analysis of variance (ANOVA) for normally distributed variables were used to compare mean group values, otherwise by the Mann–Whitney U or Kruskal–Wallis test. Chi-square test was used to compare proportions. Bonferroni–Dunn test was used for post hoc comparisons on normally distributed variables. Univariate and multivariate analysis were performed by simple or multiple linear regression analysis. Statistical power (ex post analysis; stat-power) was calculated.
Results
The clinical phenotype of cryoglobulinemia was not significantly different in MCo and MC-AT patients (Table 1). The demographic and clinical thyroid features of patients and controls are reported in Table 2. MC-AT patients and Control 2 showed significantly higher thyroid autoantibodies levels, hypoechogenicity and hypervascularity of the thyroid gland, and subclinical hypothyroidism, with respect to Control 1 and MCo.
Mean group values were compared by using one-way analysis of variance (ANOVA) for normally distributed variables, otherwise by the Mann–Whitney U or Kruskal–Wallis test. Post hoc comparisons on normally distributed variables were carried out using the Bonferroni–Dunn test. Proportions were compared by the chi-square test.
P<0.05 or less versus Control 1 or versus Control 2, or versus MCo.
P<0.05 or less versus Control 1 and versus MCo.
P<0.05 or less versus Control 1.
P<0.05 or less versus Control 1 or versus Control 2.
AbTPO, antithyroperoxidase antibody; AbTg, antithyroglobulin antibody; TSH, thyroid-stimulating hormone; TRAb, antithyrotropin-receptor antibody.
CXCL9
Serum CXCL9 levels were significantly (Table 2) higher in Control 2 than Control 1 (P<0.001) and in MCo than Control 1 (P<0.0001; stat-power=1) (Fig. 1a). MC-AT patients have circulating CXCL9 levels significantly higher than Control 2 (P<0.0001; stat-power=1) (Fig. 1b), and than MC (P=0.01; stat-power=0.9). In MCo and MC-AT patients serum CXCL9 levels were not associated with any of the clinical features of cryoglobulinemia; for example: (1) CM-II or CM-III status: 398±164 versus 372±151 in MCo; 478±234 versus 503±191 in MC-AT; (2) HCV viral load (<1,000,000 versus >1,000,000): 404±171 versus 369±148 in MCo; 486±207 versus 498±217 in MC-AT; (3) previous treatment with IFN, yes versus no; 396±163 versus 377±143 in MCo; 497±222 versus 484±206 in MC-AT; (4) treatment with corticosteroids, yes versus never treated with corticosteroids; 358±171 versus 387±156 in MCo; 469±221 versus 489±234 in MC-AT.

In MC-AT patients and Control 2, CXCL9 was studied in relation to the clinical features of AT (age; gender; thyroid volume <6 mL; thyroid hypoechoic pattern or hypervascularity; AbTg or AbTPO positivity; and subclinical hypothyroidism). Serum CXCL9 levels were significantly increased in MC-AT patients with hypothyroidism with respect to those without hypothyroidism (615±321 versus 415±187; P=0.04, ANOVA), and in Control 2 with a thyroid hypoechoic pattern with respect to those without a hypoechoic pattern (187±134 versus 122±119; P=0.03, ANOVA).
By defining a high CXCL9 level as a value of at least 2 SD above the mean value of the control group 1 (>122 pg/mL), 5% of Control 1, 34% of Control 2, 91% of MCo, and 97% of MC-AT, had high CXCL9 (P<0.0001, chi-square).
No significant association was observed in relation to the duration of the disease.
CXCL10
Serum CXCL10 levels were significantly (Table 2) higher in Control 2 than in Control 1 (P<0.001). MCo have serum CXCL10 levels significantly higher than Control 1 (P<0.0001) (Fig. 2a). MC-AT patients have serum CXCL10 levels higher than Control 2 (P<0.0001) (Fig. 2b), and than MCo (P=0.01). In MCo and MC-AT patients, circulating CXCL10 levels were not associated with any of the clinical features of cryoglobulinemia; for example: (1) CM-II or CM-III status: 302±176 versus 319±159 in MCo; 399±167 versus 384±202 in MC-AT; (2) HCV viral load (<1,000,000 versus >1,000,000): 310±146 versus 318±178 in MCo; 408±212 versus 376±174 in MC-AT; (3) previous treatment with IFN, yes versus no; 321±178 versus 305±144 in MCo; 373±170 versus 398±214 in MC-AT; (4) treatment with corticosteroids, yes versus never treated with corticosteroids; 309±167 versus 334±161 in MCo; 392±193 versus 384±191 in MC-AT.
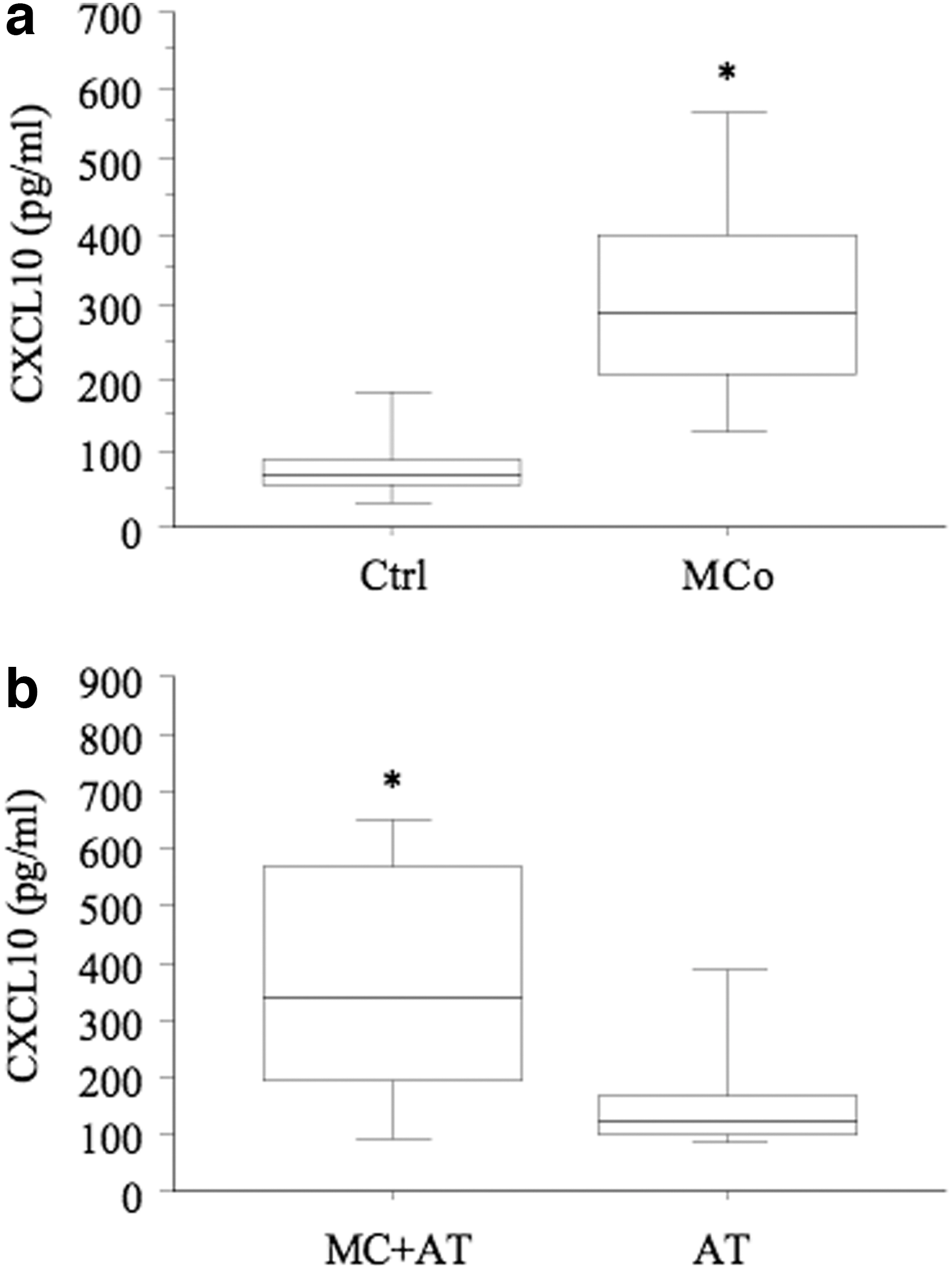
In MC-AT patients and control 2, CXCL10 was studied in relation to the clinical features of AT (see above). Serum CXCL10 levels were significantly increased in MC-AT patients with a thyroid hypoechoic pattern versus the ones without a hypoechoic pattern (412±156 versus 301±176; P=0.02, ANOVA) and hypothyroidism (387±145 versus 309±123; P=0.03, ANOVA), and in Control 2 with a thyroid hypoechoic pattern versus the ones without a hypoechoic pattern (111±131 versus 187±124; P=0.04, ANOVA).
By defining a high CXCL10 level as a value of at least 2 SD above the mean value of the control group (>188 pg/mL), 5% of Control 1, 24% of Control 2, 51% of MCo, and 83% of MC-AT, had high CXCL10 (P<0.0001, chi-square).
No significant association was observed in relation to the duration of the disease.
CXCL9 versus CXCL10
CXCL9 and CXCL10 were related to each other in MCo (r=0.426, P=0.001), and in MC-AT patients (r=0.375, P=0.001), by simple regression analysis.
Discussion
Our study first demonstrates high circulating levels of CXCL9 in MC patients, especially with AT and hypothyroidism. CXCL10 levels of MC-AT patients were significantly higher than those of MCo patients. Further, a strong association between serum CXCL9 and CXCL10 has been observed in patients with MC with/without AT.
The data regarding high level of CXCL9 in MC patients agree with the results obtained in patients with HCV chronic infection; in fact, most of the studies showed high serum levels of CXCL9 in HCV chronic infection (Butera and others 2005; Wan and others 2009; Wasmuth and others 2009; Zeremski and others 2009; Moura and others 2010). Only one study did not show any significant difference with controls (Helbig and others 2009).
Moreover, it has been evidenced that the most relevant changes in gene expression of HCV patients with first stage of liver fibrosis were mainly associated with the transcriptional network regulated by IFNs, including IFN-gamma-inducible genes (CXCL9, CXCL10, and CXCL11) (Bièche and others 2005). Moreover, circulating levels of CXCL9, sTNFR1, and sTNFR2 were associated with liver histology, suggesting a role of TNF activation and Th1-type cell-mediated immune response in the pathogenesis of HCV infection (Moura and others 2010).
These results suggest CXCL9 is produced by hepatocytes in the HCV-infected liver and is involved in T cell recruitment and in the pathogenesis of HCV chronic hepatitis infection.
In this respect, only patients without cirrhosis were recruited in the study, while the role of thyroid autoimmune disorders (that may influence CXCL9 serum levels) was specifically considered. Our study demonstrates high circulating CXCL9 in MC patients, at levels similar to those found in HCV chronic infection without cirrhosis, and suggests that CXCL9 is mainly sustained by the HCV chronic hepatitis in MC patients (Butera and others 2005; Wan and others 2009; Wasmuth and others 2009; Zeremski and others 2009; Moura and others 2010).
Our previous works demonstrated a correlation between CXCL10 and CXCL11 serum levels and presence of skin vasculitis (Antonelli and others 2008d, 2011c); consequently, we expected to find a correlation also with CXCL9. In fact, these 3 chemokines, which belong to the same CXC chemokines subfamily, are induced by IFN-gamma, recruit T cells, and bind the CXCR3 receptor; consistently, we find that CXCL10 and CXCL9 were related to each other in a simple regression analysis (see Results).
MC-AT have significantly higher circulating CXCL9 than MCo patients. This suggests the further increase of serum CXCL10 levels may be due to the thyroiditis itself (Antonelli and others 2008a), and to a predominance of the Th1 immune response in MC patients with AT (Antonelli and others 2010b).
In agreement with these data, recent results show higher CXCL9 serum levels in AT patients with respect to healthy controls (Antonelli and others 2011a, 2011b). Further, Kimura and others (2004) analyzed C57BL6 transgenic mice that aberrantly express IFN-gamma under control of the Tg promoter (Antonelli and others 2012). Transgenics exclusively expressed CCL4, CXCL9, and CXCL11, and showed increased expression of CCL5 and CXCL10. Further, the secretion of CXCL9 in primary cultures of human thyrocytes can be stimulated by IFN-gamma and TNF-alpha (Antonelli and others 2009a, 2009d, 2010a). Only one study showed discrepant results in a small number of patients with AT (Domberg and others 2008).
To our knowledge, this is the first study reporting a correlation between CXCL9 and CXCL10 levels in MC patients with/without AT. This correlation strongly reinforces the hypothesis that the immune process in chronic hepatitis C and AT (a Th1 immune response with secretion of IFN-gamma and TNF-alpha) might be responsible for the increase of both chemokines both in MC and AT. However, CXCL9 has some peculiarities with respect to CXCL10 (Loetscher and others 2001; Antonelli and others 2011b), suggesting that they may have, at least in part, a different role in MC and AT, that remains to be investigated.
More recently, it has been shown the high plasma CXCL10 levels correlate with a poor outcome of antiviral therapy in patients with hepatitis C (Antonelli and others 2009c, 2012); a low baseline CXCL10 level was associated with low viral load, rapid viral response, and a sustained viral response in HCV+ patients treated with IFN (Butera and others 2005; Diago and others 2006; Lagging and others 2006; Romero and others 2006). Since IFN is an effective therapy for MC, future studies will evaluate if pretreatment serum CXCL9 levels may be associated with virological response to IFN in MC patients (Antonelli and others 2012).
In conclusion, we first demonstrate high serum levels of CXCL9 in MC patients. Serum CXCL9 levels in MC-AT patients are significantly higher than in MCo patients. Further, a strong association between serum CXCL9 and CXCL10 has been observed in patients with MC with/without AT, strongly suggesting the importance of a Th1 immune response in the pathogenesis of both diseases. Future studies in larger series of patients will be done to evaluate the usefulness of serum CXCL9 dosage as prognostic marker in the follow-up of MC patients, especially with AT.
Footnotes
Author Disclosure Statement
The authors have no commercial associations that might create a conflict of interest in connection with the present article; the authors have no actual or potential competing financial interests to declare.