
Abstract
To present the relationship between high CD8+ T-cell activation and poor outcome in HIV-1 pathogenesis. We hypothesized that the decrease of interleukin-21 (IL-21) levels would lead to alterations in survival of elevated immune activation with disease progress. Fifty-eight HIV-1-seropositive subjects and 21 uninfected healthy control volunteers were recruited in this study. The serum IL-21 concentrations and the levels of expression of CD38, HLA-DR, and IL-21 receptor in CD8 T cells were detected by flow cytometry. The percentages of both CD38 and HLA-DR cells in CD8 T cells were significantly inversely related to the serum IL-21 levels. IL-21 plays an important role in the mechanism of elevated CD8+ T cell immune activation leading to poor outcome in HIV-1 pathogenesis, which will be helpful for the development of current and future anti-HIV strategies.
Introduction
E
Interleukin-21 (IL-21) is a relatively recently identified member of the common-γ chain family of cytokines that includes IL-2, IL-4, IL-7, IL-9, and IL-15 (Iannello and others 2008; Yue and others 2010). This cytokine is mainly produced by activated CD4 T cells (Iannello and others 2008), including follicular helper T cells (Williams and others 2011), as well as natural killer T cells (Chevalier and others 2011), and plays a critical role in the control of both innate and adaptive immune responses (Yue and others 2010). CD8+ T cells are the primary responders to IL-21. CD8+ T cells also increase their expression of the IL-21 receptor (IL-21R) in response to T cell receptor (TCR) stimulation, showing that IL-21 primarily affects activated CD8+ T cells (Pesce and others 2006; Silver and Hunter 2008). In mice, Novy and others (2011) showed that IL-21 signaling is required for the survival of activated CD8 T cells, In addition, CD8 T cells deficient in IL-21 signaling failed to develop into long-lived memory cells and ineffectively contained these chronic viral infections, leading to poor outcome in HIV-infected individuals. However, the relationship between IL-21 and CD8 T cell activation in Chinese HIV-infected individuals has not been described. In this article, we first present the relationship between the IL-21 and cytotoxic lymphocytes activation in HIV-infected patients in China and study the mechanism of IL-21 in HIV infection.
Materials and Methods
Study subjects
Fifty-eight HIV-1-seropositive subjects (32 men, 26 women; median age 37 years, range 25–56 years) and 21 uninfected healthy control volunteers (13 men, 8 women; median 35 years, range 23–46 years) were recruited at the Second Xiangya Hospital, Central South University (CSU), after informed consent and CSU institutional review board approval were obtained. Peripheral blood mononuclear cells (PBMCs) were isolated from anticoagulated peripheral blood by Histopaque density-gradient centrifugation and cryopreserved for later use. The patients were clinically classified according to the 1993 revised criteria from the Center for Disease Control and Prevention and comprised 20 asymptomatic HIV-1 infected patients (CD4 ≥200/μL, A1, A2), 30 AIDS patients (CD4 <200/μL, A3, B3, C3), and 8 long-term nonprogressors (LTNP; infected for >7 years, CD4 >500/μL not receiving HAART, and without having any AIDS-defining condition; Table 1).
The correlations were nonsignificant (P>0.05) between CD8 counts and viral loads counts and between CD8 counts and viral loads for all groups of patients.
Viral load (VL) is shown as the number of HIV-1 RNA copies/mL at the time of sample collection.
LTNP, long-term nonprogressors; HIV, asymptomatic HIV-1-infected patients; N/A, not applicable.
Viral load, CD4 T cell, and CD8 T cell count determination
HIV-1 viral load was measured in thawed plasma samples by quantitative reverse transcription–polymerase chain reaction assay (Shenzhen PG Biotech/Qiagen) according to the protocol provided with the test kit, using a Gene-Amp 7300 system (Applied Biosystems). The available range of detection was 50–10,000,000 HIV-1 RNA copies/mL of plasma. The absolute CD4 T cell and CD8 T cell counts were measured by flow cytometry using the flow count method and analyzed on a FACScan/FACSort instrument using MultiSET software (BD Biosciences).
IL-21 concentrations
The concentration of IL-21 was determined in plasma from healthy donors and HIV-infected individuals using a human interleukin ELISA kit test provided by 4A Biotech Co. Ltd., following the manufacturer's instructions. The lowest test sensitivity was 7 pg/mL.
CD38, HLA-DR, and IL-21R expression on CD8+ T cells determined by flow cytometry
Cryopreserved PBMCs were thawed, resuspended at 1×106 cells/mL in an R10 medium, and rested for 2 h at 37°C with 5% CO2. Cells were then washed with phosphate-buffered saline–2% fetal calf serum and stained for intracellular amino groups to discriminate between live and dead cells (violet viability dye; Invitrogen). After an additional wash, the following surface antibodies were added: CD38-PE (Biolegend)/CD8-APC-Cy7 (BD Biosciences)/CD3-FITC (Biolegend), anti-IL-21R–PE (Biolegend)/CD8-APC-Cy7/CD3-FITC, and HLA-DR-PE (Biolegend)/CD8–APC-Cy7/CD3-FITC. Cells were washed and fixed with 1% paraformaldehyde. Samples were acquired on a BD LSRII (BD Biosciences) multicolor flow cytometer and analyzed using FACSDiva software. Initial gating was on the lymphocyte population; a plot of forward-scatter width versus height was used to remove doublets. Expression of IL-21R, HLA-DR, CD38, was measured on CD8+ T cells (CD8+CD3+ cells).
Statistical analysis
Data were analyzed with SPSS 13.0 (SPSS). The variables were compared using one-way analysis of variance or paired samples t-test. Association between continuous variables was tested using a nonparametric Spearman rank correlation test. P<0.05 was considered as statistical significance.
Results
CD4 and CD8 counts and viral loads in different subjects
Fifty-eight study patients were enrolled (Table 1), which included 20 asymptomatic HIV-1 infected patients, 30 AIDS patients, and 8 LTNP. The median CD4 T cells for LTNP, asymptomatic HIV-infected patients, and AIDS patients were 750 (range 560–954) counts/μL, 420 (range 360–652) counts/μL, and 156 (range 98–260) counts/μL, respectively. The median CD8 T cells with LTNP were 1,063 (range 754–1,537) counts/μL, and those with the asymptomatic HIV-infected patients were 950 (range 660–1,250) counts/μL, and those for AIDS patients were 814 (range 645–1,360) counts/μL. LTNP have a viral load below 50 copies/mL. The median plasma viral loads were 326 (range 82–947) copies/mL in AIDS patients and 62,800 (range 11,200–560,800) copies/mL in asymptomatic HIV-infected patients, respectively. The median CD4 T cells and CD8 cells for healthy were 812 (range 675–985) counts/μL and 640 (range 356–562) counts/μL. The correlations were nonsignificant (P>0.05) between CD8 counts and CD4 counts and between CD8 counts and viral loads for all groups of patients.
Levels of circulating IL-21 and IL-21R expression on CD8
We found that the serum IL-21 levels for LTNP were 401.8±212.7 pg/mL (mean±standard deviation), which were significantly higher than those for either asymptomatic HIV-infected patients (232.1±98.4 pg/mL; P<0.05) or AIDS patients (105.5±54.8 pg/mL; P<0.01; Table 2). However, the serum IL-21 levels from LTNP were not significantly different from those of healthy controls (468.4±120.5 pg/mL; Table 2). The serum IL-21 levels and CD4 cell counts showed a statistically significant correlation for AIDS patients (r=0.670; P<0.001; Fig. 1A), for asymptomatic HIV-infected patients (r=0.590; P=0.002; Fig. 1B) and for all HIV-infected patients (r=0.56, P<0.001; Fig. 1C). For the small number of patients, no relationship between the serum IL-21 levels and CD4 cell counts was seen in LTNP (P>0.05) (data not shown). The correlations were nonsignificant (P>0.05) between IL-21 levels and viral loads. The IL-21R expression on CD8 with LTNP was 11.21%±1.75%, those with asymptomatic HIV-infected patients was 13.01%±2.72%, and those with AIDS patients were 15.24%±3.10%. Although the differences were not statistically significant, there was a tendency for the IL-21R expression on CD8 increase with the severity of HIV infection.

Pearson's correlation between interleukin-21 (IL-21) and CD4 cells in different groups for AIDS patients
P values were calculated by Mann–Whitney test.
P<0.05 for LTNP versus asymptomatic HIV-infected patients.
P<0.05 for LTNP versus AIDS patients.
P<0.05 for AIDS patients versus healthy controls.
P<0.05 for LTNP versus healthy controls.
P<0.05 for asymptomatic HIV-infected patients versus healthy controls.
P<0.05 for AIDS patients versus asymptomatic HIV-infected patients.
IL-21, interleukin-21; SD, standard deviation.
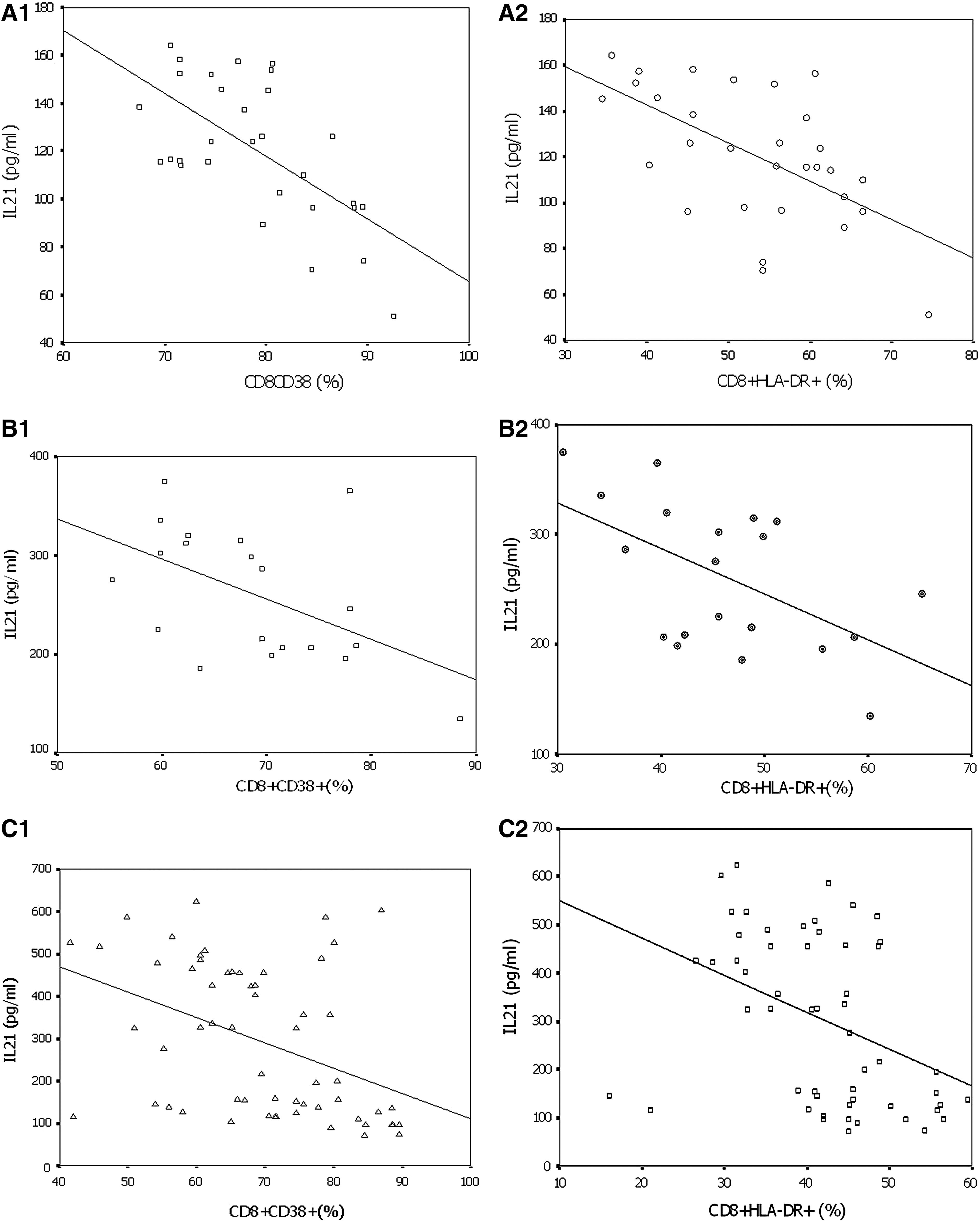
CD38 and HLA-DR expression in CD8 T cells
As shown in Table 2, a significant increase in the level of activation of CD8 T cells was observed in AIDS patients, asymptomatic HIV-infected patients, and LTNP when compared with healthy controls. The expression of CD38 and HLA-DR in CD8 T cells in AIDS patients was significantly increased in comparison with asymptomatic HIV-infected patients and LTNP. The expression of CD38 and HLA-DR in CD8 T cells in LTNP was significantly lower than those of asymptomatic HIV-infected patients and AIDS patients. No significant differences in absolute numbers of CD38 and HLA-DR were observed between different groups of the patients.
The proportions of CD8 T cell expression CD38 and HLA-DR were significantly inversely correlated with the level of IL-21 in AIDS patients (CD8/CD38: r=−0.633, P<0.001, Fig. 2A1; HLA-DR/CD8: r=−0.593, P=0.001, Fig. 2A2), in asymptomatic HIV-1 infected patients (CD8/CD38: r=−0.519, P=0.015, Fig. 2B1; HLA-DR/CD8: r=−0.552, P=0.013, Fig. 2B2); and in all HIV-infected patients (CD8/CD38: r=−0.39, P=0.009, Fig. 2C1; HLA-DR/CD8: r=−0.38, P=0.015, Fig. 2C2). For the small number of patients, the correlations were nonsignificant (P>0.05) between the proportions of CD8 T cell expression CD38 and HLA-DR and IL-21 levels in LTNP (data not shown). No relationship between the absolute numbers of CD8 T cell expression CD38 and HLA-DR and IL-21 was seen in all groups of patients (P>0.05).
The correlation between CD8 T cells expressing CD38 and HLA-DR and IL21 levels for AIDS patients
Discussion
Progress in the fight against the HIV/AIDS epidemic is hindered by our failure to elucidate the precise reasons for the onset of immunodeficiency in HIV-1 infection. Increasing evidence suggests that elevated immune activation is associated with poor outcome in HIV-1 pathogenesis (Cohen Stuart and others 2000; Deeks and others 2004). However, the basis of this association remains unclear. Through ex vivo analysis of the relationship between cytotoxic lymphocytes activation and IL-21, we show that the activation level of CD8 and the level of IL-21 are closely related.
In this study, sera from all groups of HIV-infected patients showed that there was a tendency for the percentages of CD38+ and HLA-DR+ cells in CD8 T cell increase with the severity of HIV infection. Higher CD38+ and HLA-DR+ expression in CD8 T cells from AIDS patients and asymptomatic HIV-infected patients was observed compared to healthy controls. These results are comparable with the finding of Sousa and others (Cohen Stuart and others 2000; Sousa and others 2002), which showed that CD8+ T cell immune activation is a strong predictor of disease progression in HIV infection. While the reason for this occurrence is not straightforward, some explanations are plausible. One explanation for this may be that CD8+ T lymphocytes acquired persistent activation due to the continuous replication of HIV over the course of disease progression (Cohen Stuart and others 2000); as a result, the percentages of activation marker expression in CD8 T progressively increased. The absolute CD8+ T cells, however, gradually decreased with disease progression; thus, there appeared a tendency for lower CD38/HLA-DR expression in CD8 T cells with AIDS patients compared asymptomatic HIV-infected patients, indicating that despite the fraction of CD38/HLA-DR-expressing CD8 T cell continued to increase with HIV antigenic stimulation, but due to the decrease in the total number of cytotoxic lymphocytes, CD8+ T cell activation gradually becomes less as the infection progresses.
Still unclear, however, is the mechanism whereby elevated CD8+ T immune activation leads to poor outcome during untreated HIV-1 disease. Several studies have now convincingly demonstrated that IL-21 impacts HIV-1 disease chronicity and is related to disease progression. Our results are consistent with their reports that showed that the serum IL-21 concentrations gradually decreased with the severity of HIV infection (Iannello and others 2008; Yue and others 2010). Given the correlation between the serum IL-21 concentrations and disease progression, we were interested whether there is a causative link between the serum IL-21 concentrations and immune activation of CD8+ T cell. We observed that the percentages of CD38/HLA-DR-expressing CD8 T cell were getting higher and higher with the gradual reduction of serum IL-21 levels, and the upregulation of the frequency of CD38/HLA-DR was significantly correlated with a decreased plasma IL-21 concentrations. The highest serum IL-21 concentrations and the lowest percentages of CD38/HLA-DR-expressing CD8 T cell from LTNP were observed in these groups, suggesting that immune activation with HIV antigenic stimulation caused the upregulation of the frequency of CD38/HLA-DR. However, due to the reduction of IL-21, the continuous activation of CD8 cells will be gradually exhausted, and IL-21 is critical for CD8 T cell exhaustion and the maintenance of viremia control. These results are consistent with the finding of Novy and others (2011) that showed that IL-21 signaling is required for the survival of activated CD8 T cells. In addition, CD8 T cells deficient in IL-21 signaling failed to develop into long-lived memory cells and ineffectively contained these chronic viral infections, thus leading to poor outcome in HIV-infected individuals. We also evaluated the IL-21R expression on CD8 and found that although the differences were not statistically significant, there was a tendency for the IL-21R expression on CD8 increase with the severity of HIV infection, demonstrating that CD8+ T cells continued to increase their expression of the IL-21R with HIV antigenic and TCR stimulation (Pesce and others 2006; Silver and Hunter 2008).
In conclusion, this study demonstrated that IL-21 plays an important role in cytotoxic lymphocyte activation in Chinese patients. This may be part of the mechanism through which HIV-1-mediated immune activation exhausts the capacity of the immune system.
Footnotes
Acknowledgments
The authors acknowledge the participation of the following members of the Division of Infectious Diseases: Zeng Si, who helped collect the case data and blood samples in the experiments. This study was supported by Grants from the Central South University basic scientific research special funds of China (2011QNZT169).
Author Disclosure Statement
The authors declare that no competing financial interests exist.