
Abstract
Graft-versus-host disease (GVHD) is associated with morbidity and mortality in the recipients of allogeneic hematopoietic stem cell transplants (allo-HSCTs). Interleukin-1β (IL-1β) is a potent inflammatory mediator involved in different inflammatory conditions. Therefore, we aimed to investigate the association of IL1B gene polymorphism in recipients and donors in cases in which acute GVHD (aGVHD) has been reported and the impact of this gene polymorphism on the level of cytokines in the blood and saliva. Fifty-eight consecutive allo-HSCT recipients and their donors were prospectively studied. Saliva and/or blood samples were obtained from the recipients and donors to identify the IL1B gene polymorphism, and cytokine levels were assessed by ELISA. Samples were collected weekly from 7 days before transplantation (day −7) to 100 days after allo-HSCT (day+100), for a total of 16 weeks or until death. aGVHD occurred in 27 individuals evaluated. A significant association was identified between the IL1B polymorphism in the donor and aGVHD development in the corresponding recipients. However, no significant association was detected between the IL1B polymorphism in recipients and the development of aGVHD. In the recipients who were diagnosed with aGVHD, the level of IL-1β in the saliva and blood were increased. In the saliva, IL-1β levels increased progressively from the time before the diagnosis of aGVHD until weeks after the diagnosis, whereas in the blood, IL-1β peak levels could be observed within the time allotted for diagnosis, followed by a decrease in the levels. In addition, we observed a significant association between the IL1B genotype of the recipient (CC) and high IL-1β levels in the saliva at week 13. In conclusion, IL-1β could be considered a useful predictor of aGVHD development.
Introduction
A
Cytokines are important mediators and regulators of GVHD (Ferrara 2008; Correia-Silva and others 2011). aGVHD reflects an exaggerated response of the normal inflammatory mechanisms that involve donor T cells and multiple innate and adaptive cells and mediators (Choi and others 2010). Reddy and Ferrara (2003) classified the pathogenesis of the disease into 3 sequential phases: (1) activation of antigen-presenting cells; (2) donor T cell activation, proliferation, differentiation, and migration; and (3) target tissue destruction.
Interleukin-1 (IL-1) is a proinflammatory cytokine that plays an essential role in several diseases. This cytokine is a primary activator of early chemotactic cytokines as well as the expression of adhesion molecules that facilitates the migration of leucocytes into tissues (Nicklin and others 1994). The 3 genes that regulate the production of IL-1 are IL1A, IL1B, and IL1RN (Nicklin and others 1994), which are located on chromosome 2q13. Genes IL1A and IL1B control the production of the IL-1α and IL-1β proinflammatory proteins, respectively (Greenstein and Hart 2003). The polymorphism at the +3954 locus of the IL1B gene has been associated with increased production of the cytokine (Greenstein and Hart 2003).
Previous studies have already demonstrated the association between cytokine polymorphisms and the occurrence of aGVHD (Middleton and others 1998; Cullup and others 2001; Socié and others 2001; Dickinson and others 2007; Markey and others 2008; Resende and others 2010; Resende and others 2012). However, the effects of these polymorphisms on the levels of cytokines in the blood and saliva are not well addressed. Therefore, studying the relationship between gene polymorphisms and cytokine levels is important in understanding the contribution of genotypes and phenotypes to the pathogenesis of GVHD. Thus, we aimed to evaluate the association between IL1B polymorphisms and IL-1β levels in the blood and saliva as well as their relationship with the development of aGVHD in allo-HSCT recipients.
Methods
Subjects and collection of samples
Between October 2006 and October 2008, 58 consecutive allo-HSCT recipients and the respective donors from Hospital das Clínicas—Universidade Federal de Minas Gerais (HC-UFMG) were included in this prospective study. The genetic homogeneity of the group studied was compounded by the mixed nature of the population of Brazil. The Brazilian ethnic population is complex owing to the high rate of miscegenation between individuals of European, African, and indigenous descent. The Minas Gerais State represents a region where the population comprises individuals from all these geographical regions (Parra and others 2003). The recipients were conditioned for allo-HSCT according to the specific protocols of the Stem Cell Transplant Unit at HC-UFMG. The study was approved by the local Ethics Committee (Process ETIC 613/07). Cyclosporin, combined with methotrexate or mycophenolate mofetil, was used for GVHD prophylaxis, whereas methylprednisolone, combined with cyclosporin, was used for GVHD treatment. Saliva and/or blood samples were collected from recipients and donors 1 week before allo-HSCT, and DNA was extracted for analysis. The saliva samples were collected from the floor of the mouth, tongue, and labial and buccal normal oral mucosa of the study subjects by using cotton swabs. The samples were placed immediately in sterile tubes containing 500 μL of the Krebs buffer (20% NaCl, 2% KCl, 2% CaCl2·2H2O, MgSO4, KH2PO4, and C6H12O6) and stored at −20°C until processing. Sites with localized injuries were not included. Peripheral blood (4 mL) was collected in BD Vacutainer® blood collection tubes (Becton Dickinson, Franklin Lakes, NJ) containing ethylenediaminetetraacetic acid (EDTA) and stored at −70°C until processing.
To determine the cytokine levels, 1 blood sample and 1 saliva sample were obtained once a week from 7 days before transplantation (day −7) up to 100 days after allo-HSCT (day +100), for 16 weeks or until death. Saliva samples were collected in Salivette® tubes (Sarstedt AG & Co, Numbrecht, Nordrhein-Westfalen, Germany) according to the manufacturer's instructions. The saliva samples were diluted (1:1) in a phosphate-buffered saline solution containing protease inhibitors (0.1 mM phenylmethylsulfonyl fluoride, 0.1 mM benzethonium chloride, 10 mM EDTA, and 0.01 mg/mL aprotinin A), together with 0.05% Tween-20, and subsequently stored at −20°C until analysis. Serum samples were obtained from venous blood samples that where centrifuged within 2 h after blood collection and stored at −20°C.
The total protein content in the saliva was determined using the Bradford Reagent (Sigma, St. Louis, MO) and bovine serum albumin standards (Fermentas Life Sciences, Vilnius, Lithuania). The total protein content was used to correct the cytokine values for the saliva samples.
DNA isolation
Total genomic DNA was extracted from the saliva and blood samples using the QIAamp DNA Blood Mini Kit (Qiagen, Valencia, CA) according to the manufacturer's instructions. The final elution of the saliva and blood DNA was performed in 50 μL of the specific AE buffer from the kit and stored at −20°C until use.
Cytokine gene polymorphism analysis
Recipient/donor genotypes for the IL1B (+3954) polymorphism were analyzed via polymerase chain reaction (PCR) amplification and digestion, as previously described (Kornman and others 1997). The PCR products were separated via polyacrylamide gel electrophoresis in a 6.5% gel and visualized by staining with silver. The sequences of the PCR primers and restriction enzymes used are listed in Table 1. The phenotypes for the IL1B gene were grouped into low and high producers, predicted according to the genotypes as defined previously: TT or CT (high producer) and CC (low producer) (Walker and others 2000).
IL, interleukin.
Cytokine analysis
The cytokine concentration was determined by means of a quantitative sandwich enzyme-linked immunosorbent assay by using the Human IL-1β DuoSet (DY201) Kit (R&D Systems, Minneapolis, MN).
Diagnosis of aGVHD
aGVHD was clinically diagnosed (with or without histopathological confirmation) by the attending physician. All recipients were evaluated to determine the occurrence of aGVHD in the skin, liver, and gut, as previously described (Glucksberg and others 1974). If the disease was detected in 1, 2, or all 3 of these sites, aGVHD was considered present. If no clinical or histopathological signs were detected, aGVHD was considered absent.
Statistical analysis
Categorical variables (IL1B genotypes and the presence and absence of aGVHD) and continuous variables (IL-1β levels) were summarized. Univariate analyses were performed using the Chi-squared test for categorical variables. The Mann–Whitney and Wilcoxon tests were used to compare 2 related continuous variables, using the SPSS software (version 17.0; SPSS, Inc., Chicago, IL). A P value≤0.05 was considered statistically significant.
Results
Clinical outcomes
The median age for the recipients and donor was 31.5 years (range: 5–56 years) and 35.4 years (range: 6–69), respectively. Clinical data from the recipients and donors are presented in Table 2. aGVHD was observed in 27 recipients, who had developed aGVHD at ∼6.5 weeks (range 4–12 weeks).
Impact of IL1B gene polymorphisms in recipients and donors on development of aGVHD
The details of donor and recipient gene polymorphisms, their prevalence, and corresponding phenotypes, as well as the impact of the polymorphisms on the incidence of aGVHD, are shown in Table 3. Significant association was found between the occurrence of aGVHD and the presence of the allele T (T+ [TT+CT]) in donors (P=0.002). In recipients who received transplants from T allele-carrying donors, the likeliness of developing aGVHD was 8.84 times that of the recipients who received transplants from donors not carrying the T allele. No significant association was found between the IL1B polymorphism in the recipients and development of aGVHD.
Chi-square test.
Associated phenotype: blow producer; chigh producer.
NS, not significant; P, present; A, absent; GVHD, graft-versus-host disease.
IL-1β levels according to the time of aGVHD diagnosis
The kinetics of IL-1β levels in the saliva and blood, depending on the time of aGVHD diagnosis, is presented in Fig. 1. The IL-1β levels in the saliva increased progressively from before aGVHD diagnosis up to weeks after the diagnosis (Fig. 1a), whereas in the blood, the levels of this cytokine presented a peak upon diagnosis and decreased subsequently (Fig. 1b). Comparing the cytokine levels in the saliva over time, significant association was identified between the cytokine levels at the moment of aGVHD diagnosis and the levels at the first and second weeks following aGVHD diagnosis (P=0.04 and P=0.04, respectively) (Fig. 1a). When the cytokine levels in the blood were compared over time, significant association was observed between the first cytokine levels in the week before and at the moment of aGVHD diagnosis (P=0.01), as well as between the moment of aGVHD diagnosis and the second week after diagnosis (P=0.03) (Fig. 1).
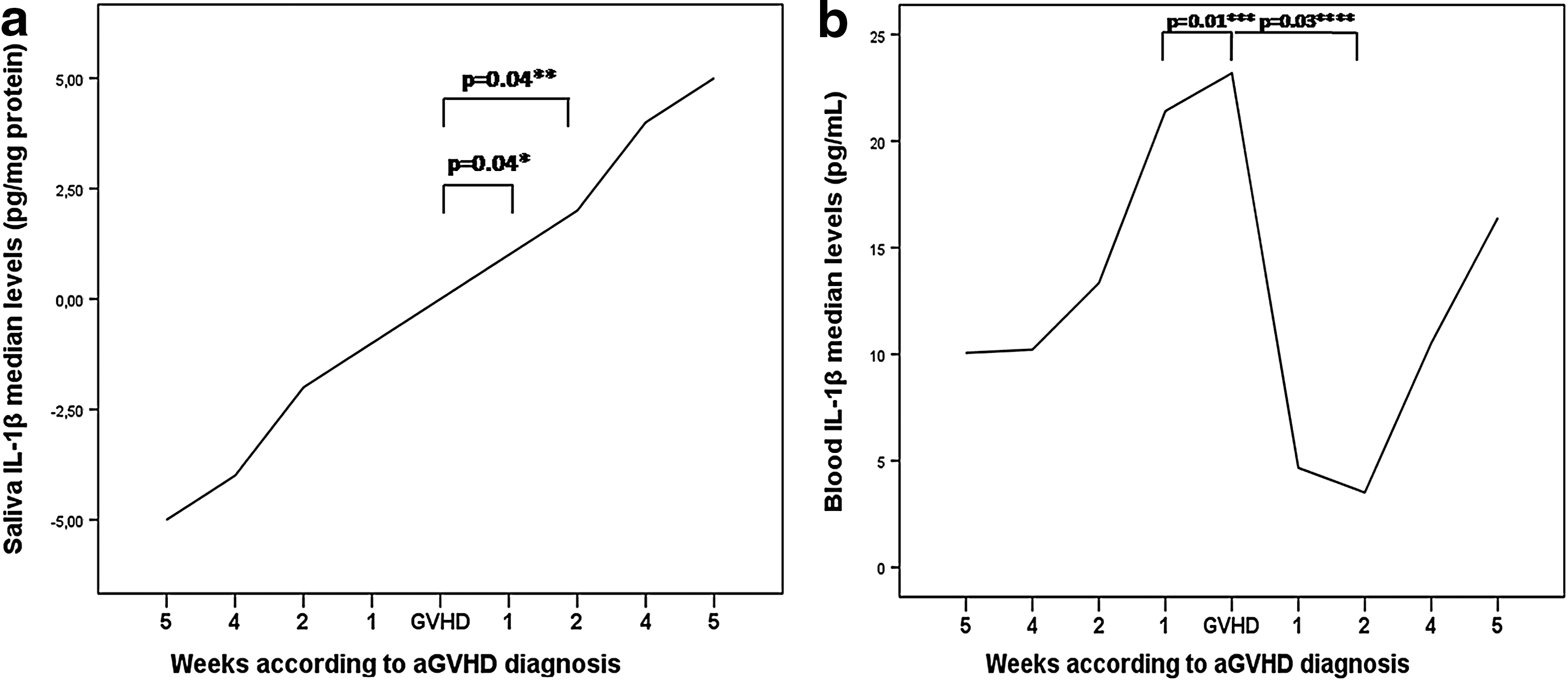
Kinetics of interleukin (IL)-1β saliva and blood levels in patients with acute graft-versus-host disease (aGVHD) according to the time of the diagnosis:
IL-1β levels in blood and saliva and IL1B polymorphisms in recipients and donors
Significant association between the IL1B genotypes and the IL-1β levels in the saliva of the recipients was observed at week 13, where high levels of IL-1β were related to the CC genotype. The median level of IL-1β in recipients who presented CC genotypes at week 13 was 25.97 pg/mg protein, whereas the median level in individuals with CT/TT genotypes, reported as high-producer phenotypes, was 8.92 pg/mg protein (P=0.01) (Fig. 2). No association was found between recipients with the IL1B genotype and the IL-1β levels in their blood (data not shown). IL-1β levels in the blood and saliva were not associated with IL1B polymorphisms in donors (data not shown).

Association between IL-1β levels in saliva at week 13 and IL1B genotypes. **Mann–Whitney test.
Discussion
The impacts of IL1B genotypes on IL-1β levels in the blood and saliva, as well as their association with the occurrence of aGVHD, have yet to be clarified. In addition, the impact of cytokine levels in the saliva in aGVHD has not been determined. Cytokines are an important component of saliva and regulate oral cavity homeostasis. Altered salivary cytokine levels have been observed in patients with various diseases, and it may reflect oral and/or systemic conditions (MacMillan and others 2003; Boras and others 2006; Resende and others 2010). Thus, salivary cytokine levels represent an important noninvasive diagnostic tool (Cullup and others 2001).
IL-1 is a cytokine that is released by monocytes and macrophages before transplantation, as they have been primed during the development phases of GVHD (Nicklin and others 1994; Choi and others 2010). This release can induce direct target-cell damage by activating caspase-I inflammasome. IL1 gene polymorphisms have also been associated with results from transplants (Gao and others 2009).
Many studies have reported associations between IL1B gene polymorphisms and several chronic diseases. Among these are studies that evaluated the polymorphism in the +3954 (C/T) locus of IL1B in a Brazilian population with periodontal disease (Moreira and others 2005) and in recurrent aphthous stomatitis (Guimarães and others 2007). In these studies, the authors reported an association between these chronic diseases and the presence of the polymorphic allele. Few studies have evaluated IL1B gene polymorphisms together with GVHD outcomes. Other authors did not find an association between the occurrence of aGVHD and IL1B polymorphisms in donors and/or recipients in both American and British populations (MacMillan and others 2003; Gao and others 2009). However, MacMillan and others (2003) showed that the presence of the IL1B T allele in both donors and recipients was associated with improved survival and decreased treatment-related mortality. In the present study, we observed an association between the presence of the T allele in donors and the occurrence of aGVHD. Therefore, the IL1B polymorphism could be associated with the development aGVHD in the Brazilian population.
Few studies have assessed IL-1β levels in the blood of patients with aGVHD (Li and others 2009), and none to date have evaluated cytokine levels in the saliva. Gao and others (2009) observed that IL-1β is closely related to aGVHD. These authors also reported that serum IL-1β levels in patients with aGVHD did not change during preconditioning, but the levels increased when aGVHD was diagnosed (Gao and others 2009). Other work showed that IL-1β might be involved in the damage to the thymus by aGVHD (Luo and others 2009).
In the present study, we observed that IL-1β levels in saliva increased progressively from the time before aGVHD diagnosis up to weeks after the diagnosis, when the kinetics of the cytokine in aGVHD patients was evaluated. By contrast, in the blood, a peak of IL-1β level could be observed upon diagnosis, followed by a significant drop. This difference could be explained by the application of immunosuppressive drugs used to treat aGVHD, which can inhibit the transcription of cytokine genes and alter the course of the disease. This effect is initially more evident in the blood, owing to the bioavailability of the drug, which may well explain the drop in serum cytokine levels during the weeks following the diagnosis.
In the present study, we also observed that higher levels of IL-1β in the saliva were associated with CC genotypes in the recipient, previously described as a low-producer phenotype, which could be observed at week 13. It is also important to note that the patients of this study developed aGVHD between weeks 4 and 12. This finding can be explained by the intense and permanent antigenic challenge to which the recipient may be subjected during the period of HSCT. This fact may be responsible for the increased release of the cytokine during the initial periods, which may not be sustained during the posterior phase, and this could in turn disrupt any association between polymorphisms and phenotypes. IL-1 production might also be affected by the levels of its specific antagonist (IL-1ra) (Dinarello and Thompson 1991). IL-1ra is an anti-inflammatory cytokine that acts competitively and inhibits the actions of IL-1β (Buchs and others 2001). Buchs and others (2001) reported a similar result in a study on rheumatoid arthritis patients. These authors observed that patients carrying the polymorphic allele (T) presented lower levels of IL-1β and suggested that the severity of the disease was associated with an imbalance of the levels of IL-1β and IL-1ra.
Conclusions
In summary, this study presents an association between IL1B polymorphisms and aGVHD, as well as between IL-1β levels, in both the saliva and blood, and aGVHD development. In addition, significant association was found between the CC genotype and high levels of IL-1β. The kinetics of IL-1β in both fluid types may be useful for monitoring the progression of the disease.
Footnotes
Acknowledgments
This study was supported, in part, by grants from Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) and from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazil. RS Gomez is research fellow of CNPq. We thank Daniele Ramalho da Silva for technical assistance.
Author Disclosure Statement
No competing financial interests exist.