
Abstract
Oral lichen planus (OLP) is a chronic mucocutaneous condition that affects the oral mucous membrane as well as skin. It is a chronic cell-mediated autoimmune condition where the T-cell-mediated immune response plays an important part in the pathogenesis by causing damage to basal keratinocytes in oral mucosa. Cytokine gene polymorphisms have an unquestionable role in the orchestration of the immune response, leading to different functional scenarios, which in turn influence the outcome of the disease establishment and evolution. The purpose of this study was to understand the role of these cytokine gene polymorphisms in the tumor necrosis factor-alpha (TNF-α), interleukin-1β (IL-1β), and IL-6 genes with OLP in 101 individuals of Malayalam-speaking ethnicity from South India (Kerala). We further investigated the role of these polymorphisms in patients suffering from OLP with other comorbid factors. Genotyping was carried out by polymerase chain reaction–restriction fragment length polymorphism. The results demonstrate that the A allele in the TNF-α −308 polymorphism could play an important role in the susceptibility to OLP. IL-1β +3954 in OLP was associated with other comorbid factors in both allelic and genotypic combinations. However, when patients suffering from OLP were stratified to understand the involvement of other comorbid factors, we observed that the T and C alleles were independent risk factors for chronic periodontitits and diabetes mellitus. On the other hand, IL-6 −597 did not show any disease association with OLP in the study population. This study indicates that proinflammatory cytokines are an important factor in understanding the disease burden of OLP and their comorbid factors.
Introduction
Cytokines, the signaling proteins produced by a variety of cell types, are essential for the development and functioning of both the innate and adaptive immune response. Complex networks of cytokines interact in a dynamic way to homeostatically regulate the immune responses and other biological pathways. It is therefore not surprising that variation in the cytokine level has been correlated with disease susceptibility and development (Ollier 2004). Several single-nucleotide polymorphisms (SNPs) do not appear to affect the gene products, but others may have functional significance, since they affect gene transcription, RNA stability, or the coded protein itself (Shapira and others 2005; Takashiba and Naruishi 2006). Genetic and environmental influences play important roles in the variation of cytokine levels. Genetic variations that result in the structure or alternation in expression of a cytokine gene can potentially lead to a number of chronic diseases, increased risk of infection, and altered outcome of acute disorders or surgery (Smith and Humphries 2009). Even variations in the amino acid sequence of cytokines were described in healthy individuals, showing polymorphisms associated with changes of the expression of the protein and with interindividual differences on the profile of its production. This can be unraveled by investigating the cytokine gene polymorphism, thus establishing a genetic basis for cytokine dysregulation and its association with the disease (Ollier 2004).
OLP, which is a relatively common mucocutaneous disease, still has an unknown etiology. Many studies have suggested that there is a chronic, cell-mediated immune damage to basal keratinocytes in the oral mucosa that are recognized as being antigenically foreign or altered. The immune response is characterized by the accumulation and expansion of T-helper 1 (Th1) lymphocytes predominantly of the CD4+ phenotype, which further activates CD8+ cytotoxic T, leading to apoptosis of keratinocytes (Thornhill 2001; Khan and others 2003). Together, CD4+ and CD8+ T-cells are thought to produce and respond to a range of cytokines and inflammatory mediators, resulting in variations in the clinical presentation of OLP.
Immune deregulation in involving the cellular arm of the immune system and a complex cytokine network has been shown by lot of clinical and immunohistochemical studies (Walsh and others 1990; Porter and others 1997; Santoro and others 2003). Even in vitro and in vivo studies have demonstrated that the allelic variants of the cytokine genes were related to either higher or lower production of cytokines (Wilson and others 1992; Tagore and others 1999). Thus, some authors believe that this genetic variation can even contribute to disease susceptibility and may influence its course (Eijnden and others 2003).
At present, there are very few studies demonstrating the influence of the cytokine gene polymorphisms on OLP (Carrozzo and others 2004; Bai and others 2007, 2008, 2009; Xavier and others 2007). The polymorphisms that affect the expression of a given cytokine gene associated with susceptibility in one population may behave differently in individuals of distinct ethnic backgrounds. The South Indian Dravidian population is quite distinct genetically from other ethnicities as demonstrated by HLA studies conducted in the same area (Thomas and Banerjee 2005; Thomas and others 2006). Thus, this study was undertaken in an attempt to verify the association of SNPs at the tumor necrosis factor-alpha (TNF-α) (−308G/A), interleukin-1β (IL-1β) (+3954C/T). and IL-6 (−597G/A) genes in OLP of Malayalam-speaking ethnicity from South India (Kerala) and to further understand the genetic association of these polymorphisms with other comorbid factors of the disease.
Materials and Methods
Subjects and controls
A case–control study was conducted in the Government Dental College, Trivandrum, in collaboration with the Rajiv Gandhi Centre for Biotechnology, Trivandrum, with a total of 101 subjects, including 50 patients suffering from OLP and 51 controls. Subjects reporting to the OPD of the Government Dental College, Trivandrum, were clinically screened for OLP. A proforma was formulated to record the patient's personal details as well as clinical examination of the lesion. The diagnosis of OLP was confirmed clinically as well as histopathologically by the WHO (1978) criteria. No patient was suspected to have drug- or restoration-related lichenoid reaction. Individuals with severe systemic diseases such as autoimmune disorders, hemorrhagic disorders, and chronic hepatitis C were excluded. Even subjects belonging to any other ethnic group were also not included in the study. Ethnicity of subjects was determined by self-report and linguistic affiliation. On the other hand, healthy individuals from same geographical area who were not associated with OLP, chronic periodontitis (CP), and diabetes mellitus (DM) were selected randomly as controls. The study protocol was approved by the Institutional Ethics Committee, and informed consent was obtained from the subjects.
SNP selection
Selection of SNPs in the cytokine gene was based on its functionalities and variation in the distribution of alleles in the global population. Cytokines such as TNF-α, IL-1β, and IL-6 have been reported to be associated with inflammatory processes, and OLP being a chronic inflammatory condition, we selected these cytokines and their most relevant functional SNPs for the study.
DNA isolation and genotyping
Five milliliters of peripheral blood sample was collected by venipuncture from both patients and controls. Genomic DNA was isolated by a modified method of ac standard organic extraction method (phenol–chloroform DNA extraction method) by Sambrook and others (1982).
Polymerase chain reaction (PCR) was done with diluted DNA samples and the specific primers designed to amplify the area of interest of the TNF-α −308, IL-1β +3954, and IL-6 −597 genes. The amplified products were further digested using specific restriction enzymes to screen the polymorphism at these sites. PCR was carried out using a master mix containing Taq buffer, dNTPs, forward primer, reverse primer, Taq polymerase (3U), and sterile water along with extracted DNA. The thermal cycles for each gene were performed according to the following protocol.
TNF-α −308
The cycling conditions included denaturation for 5 min at 94°C, followed by 30 cycles of 30 s at 94°C, 30 s at 61°C, and 30 s at 72°C, with a final extension at 72°C for 5 min.
IL-1β +3954
The PCR cycle began with an initial denaturation step at 95°C for 2 min, followed by 35 cycles of 30 s at 95°C, 30 s at 50°C, and 30 s at 72°C, with a final extension at 72°C for 5 min.
IL-6 −597
The conditions for amplification consisted of denaturation at 95°C for 5 min followed by 35 cycles of 95°C for 30 s, 56.7°C for 30 s, and 72°C for 30 s. The run was terminated by final elongation at 72°C for 10 min.
The PCR products were further digested with a restriction enzyme for respective gene as shown in Table 1. The resulting digestion products of IL-1β +3954 and IL-6 −597 were visualized by 2% agarose gel electrophoresis at 75V to determine the genotype, whereas for TNF-α −308, a high-resolution 3.5% agarose gel was used, as shown in Figs. 1 –3.
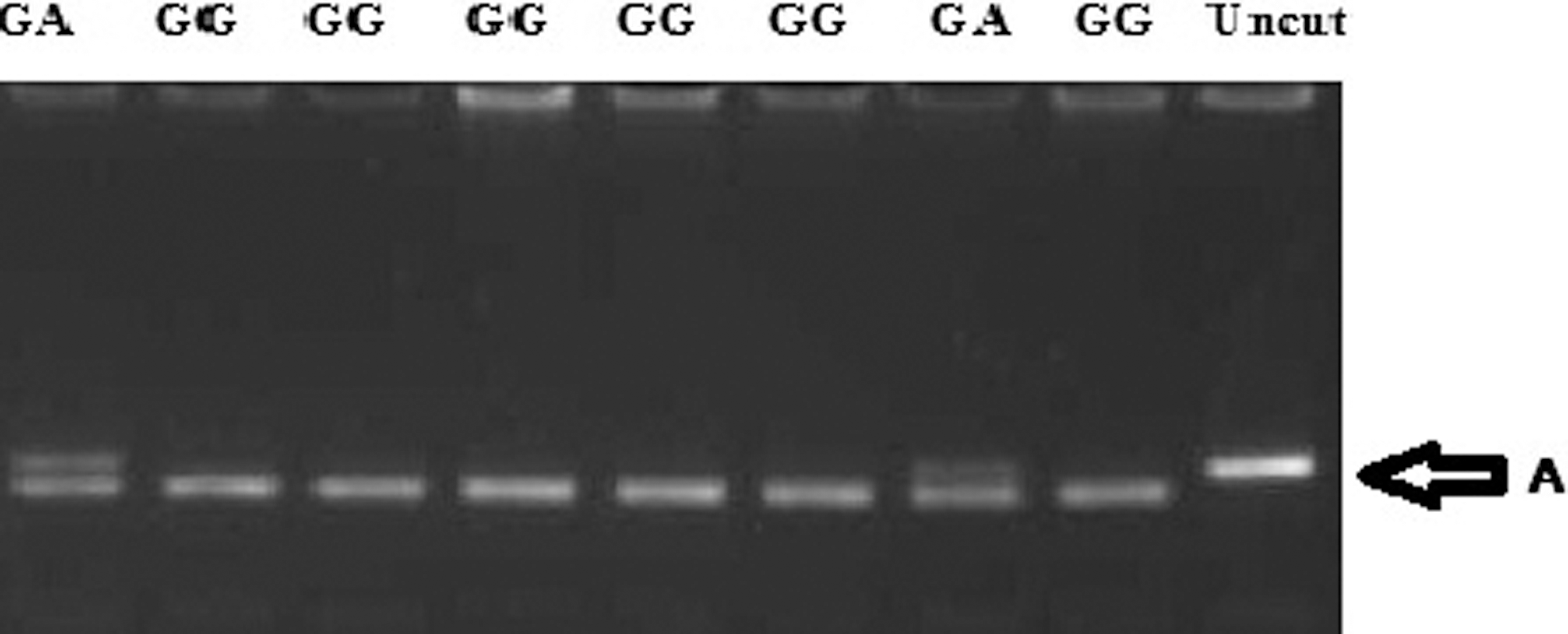
Genotyping for tumor necrosis factor-alpha (TNF-α) −308.
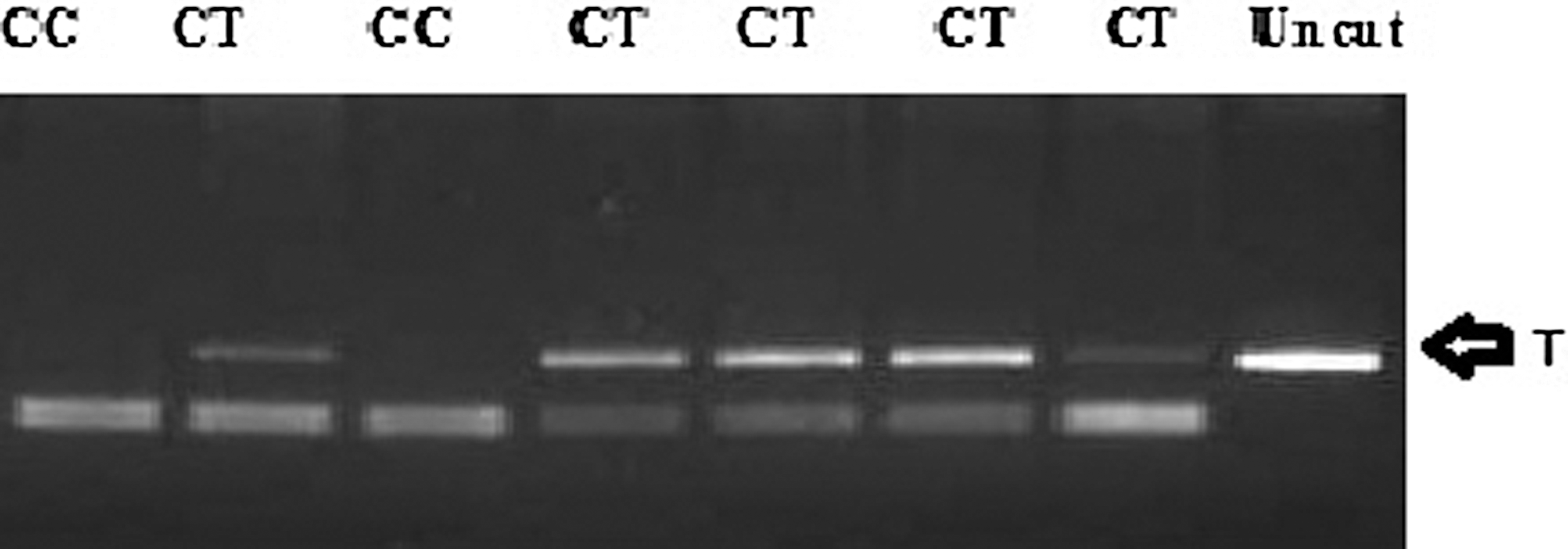
Genotyping for interleukin-1β (IL-1β) +3954.

Genotyping for IL-6 −597.
IL-1β, interleukin-1β; RFLP, restriction fragment length polymorphism; SNP, single-nucleotide polymorphisms.
Statistical analysis
A case–control association study was carried out to investigate the role of the polymorphisms at the TNF-α (−308G/A), IL-1β (+3954C/T), and IL-6 (−597G/A) genes with OLP in a genetically homogenous Malayalam-speaking ethnicity from South India (Kerala). To further understand the genetic association of these polymorphisms with other comorbid factors of the disease, the 50 patients suffering from OLP were further divided into 3 subgroups:
Subgroup A (OLP+CP+DM)): patients suffering from OLP with both CP and DM
Subgroup B (OLP−CP−DM): patients suffering from OLP without CP and DM
Subgroup C (OLP+LP): patients suffering from OLP with dermatological manifestations (LP).
The data were analyzed using Statistical Package for Social Sciences (SPSS), version 10. The data were expressed in terms of frequency and percentage. The frequency of the individual alleles as well as the homozygous and heterozygous genotypes of the TNF-α, IL-1β, and IL-6 gene polymorphisms was determined in both the patient groups and controls. To elucidate the associations and comparisons between different parameters, chi-square (χ 2) test was used as a nonparametric test. The risk factors (odds ratio) of different factors for each group were assessed by a multivariate logistic regression analysis. For all statistical evaluations, a 2-tailed probability of value <0.05 was considered significant. The Hardy–Weinberg equilibrium analysis was also carried out in the control population.
Results
The demographic details signifying the sex, age, site of clinical manifestation, clinical phenotype, and associated comorbid factors of OLP in the patient group are shown in Table 2. In our patient group, we had both an erosive and reticular phenotype with an over-representation of the reticular phenotype. The patient group was further stratified based on the associated comorbid factors, such as diabetes, CP, and dermatological manifestations. These comorbid factors within the patient group were structured into 3 subgroups based on their presence of one or more factors.
OLP, oral lichen planus; CP, chronic periodontitis; DM, diabetes mellitus; LP, dermatological manifestations.
All the patients and controls were genotyped for the TNF-α (−308G/A), IL-1β (+3954C/T), and IL-6 (−597G/A) polymorphism. The control population was found to be in the Hardy–Weinberg equilibrium for the TNF-α (−308G/A), IL-1β (+3954C/T), and IL-6 (−597G/A) polymorphism. The allelic frequency distribution of the TNF-α (−308G/A), IL-1β (+3954C/T), and IL-6 (−597G/A) genes in different populations is also graphically presented in graphs 1 –3. While comparing the genotype and allele frequencies of the TNF-α (−308G/A), IL-1β (+3954C/T), and IL-6 (−597G/A) polymorphism in the OLP patient and control population, we observe that the TNF-α −308(G/A) polymorphism is significantly associated with OLP at both the allelic and genotype level (Table 3). There was a higher frequency of the genotypes GA (24%) and allele A (12%) with an odds ratio of 13.77 in patients with OLP. However, none of the other SNPs was found to have any association with OLP.
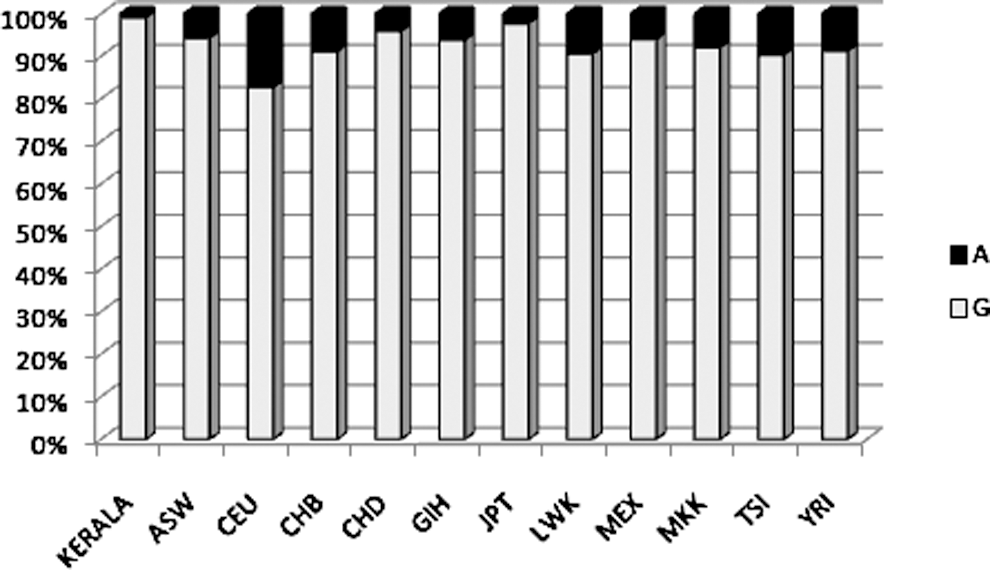
Allele frequency distribution graph of TNF-α −308G/A. Population descriptors: ASW, African ancestry in the Southwest United States; CEU, Utah residents with the Northern and Western European ancestry from the CEPH collection; CHB, Han Chinese in Beijing, China; CHD, Chinese in Metropolitan Denver, CO; GIH, Gujarati Indians in Houston, TX; JPT, Japanese in Tokyo, Japan; LWK, Luhya in Webuye, Kenya; MEX, Mexican ancestry in Los Angeles, CA; MKK, Maasai in Kinyawa, Kenya; TSI, Tuscan in Italy; YRI, Yoruban in Ibadan, Nigeria.

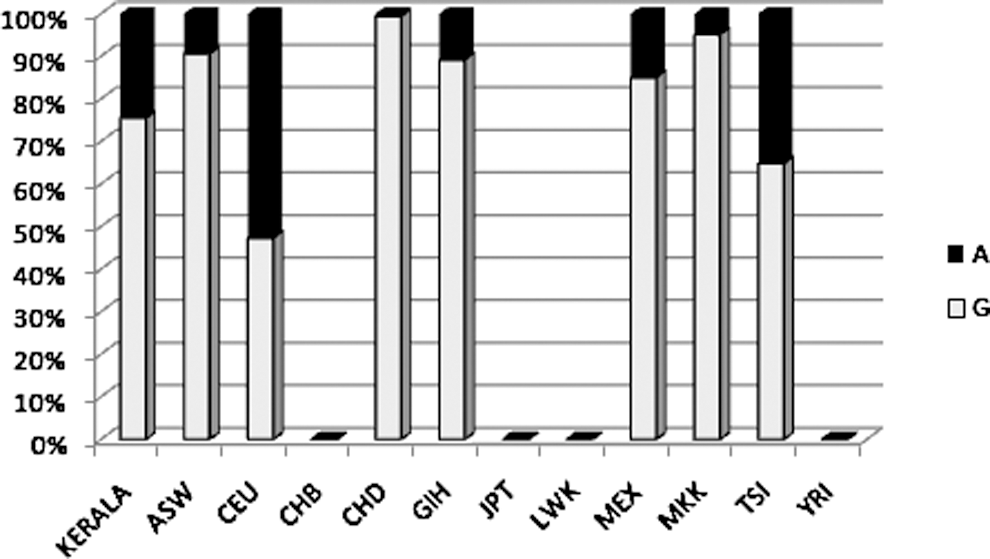
Allele frequency distribution graph of IL-1β (+3954C/T).
Allele frequency distribution graph of IL-6 (−597G/A).
The genetic association analyses were also carried out between different subgroups and controls and also within the subgroup. While comparing the genotypic and allelic distribution of TNF-α (−308G/A), IL-1β (+3954C/T), and IL-6 (−597G/A), we observed that IL-1β (+3954C/T) was significantly associated with subgroup A (patients suffering from OLP with both CP and DM) when the compared between subgroup A and control and between subgroup A and subgroup B (patients suffering from OLP without CP and DM) (Table 4), whereas TNF-α (−308G/A) was observed to be significantly associated with subgroup B (patients suffering from OLP without CP and DM) and subgroup C (patients suffering from OLP with dermatological manifestations) in comparison to the control (Table 5).
Discussion
Unraveling the pathophysiology of OLP is a major challenge. Currently, genetic factors causing imbalances in proinflammatory and anti-inflammatory cytokine production and the imbalance at the level of Th1 and Th2 immune responses are proposed to increase the susceptibility to OLP. Although, as of yet, most genetic studies in OLP have focused on the HLA (Carcassi and others 1994; La Nasa and others 1995), few reports have examined the association of the Th1/Th2 cytokine genes with OLP. Thus, genetic influence might be the basis of this Th1 bias in OLP, for different levels of cytokine production, which may reflect polymorphisms in the respective cytokine genes and influence disease development and progression.
We conducted a case–control study to understand the significance of functionally relevant variants at the TNF-α (−308 G/A), IL-1β (+3954 C/T), and IL-6 (−597 G/A) genes in 50 patients suffering from OLP and 51 ethnically matched controls. On comparing the allele frequency data of our control population for TNF-α (−308G/A), IL-1β (+3954 C/T), and IL-6 (−597 G/A) with the Hap Map allele distribution, our population was distinctly different when compared with other world population. On further investigation on the role of various polymorphisms, we observe a significant genetic association of TNF-α −308(G/A) and IL-1β (+3954 C/T) with patients suffering from OLP and its associated comorbid factors.
TNF-α is a potent immune modulator and a proinflammatory cytokine that has been implicated in the pathogenesis of many kinds of inflammatory or autoimmune diseases. The gene-encoding TNF-α is located in the major histocompatibility complex class III region of chromosome 6. Many studies have shown the central role of TNF-α in the pathogenesis of OLP (Sugermann and others 1996). It has also been demonstrated that the A allele at position −308 is associated with increased expression of TNF-α.
In the present study, we examined TNF-α at −308 G/A position and observed an increased risk with genotypes GA (24%) and allele A (12%) having an odds ratio=13.77 in patients with OLP. This observation is in accordance with the studies done in the North Italian and Brazilian populations. Carrozzo and others (2004) found that in Caucasian patients, A allele of the TNF-α −308 polymorphism was not only more frequent in patients suffering from OLP but was also significantly higher (82%) in OLP patients with skin involvement than patients with exclusive oral lesions (30%). Similarly, we also found a significant difference in the distribution of the genotype and allele frequency with GA (22.2%) and A (11.1%) in subgroup C of patients suffering from OLP with dermatological manifestations.
In the Brazilian population, TNF-α (A/A) homozygous genotypes were significantly more often detected in patients suffering from OLP who were associated with higher cytokine production (Xavier and others 2007). On the contrary, there were no significant differences in the TNF-α −308G/A polymorphism status between the OLP patient group and the healthy control group in Chinese Han ethnicity (Bai and others 2009). However, they found a significantly elevated allele A in the erosive OLP group, which indicated that the allele A of the TNF-α −308 polymorphism in Chinese origin may be associated with the development and severity of OLP through a microenvironment polarized toward Th1. However, in our study, there was no significant association in the distribution of the genotype and allele frequency among the erosive OLP group.
Earlier studies have not either mentioned or included the comorbid status in their patient group, which is also most likely to influence the development of OLP. The study on Caucasian patients (Carrozzo and others 2004) did not specify the periodontal as well as DM status in their OLP patient group. whereas in the Brazilian study (Xavier and others 2007), individuals with CP and other systemic diseases were not included. Even the Chinese study (Bai and others 2009) excluded the individuals with DM, but they have not mentioned the periodontal status in their patient group. In our study, the subgroup of OLP with both CP and DM against controls revealed no statistically significant difference of the allelic and genotypic distribution. Comparison of data between subgroup A (OLP+CP+DM) and subgroup B (OLP-CP-DM) also did not show any significant association. However, we observed the TNF-α −308 polymorphism with increased representation of the GA genotype and the A allele in subgroup B and subgroup C against controls, indicating that comorbid factors are likely to be influenced by TNF-α production as a secondary effect in patients suffering from OLP. Thus, genetically influenced TNF-α production could play an important role in the susceptibility to OLP as a primary effect and can also significantly influence comorbid factors.
IL-1β exerts a range of inflammatory and immunomodulatory activities that are important in host defense and autoimmune response. The IL-1 family consists of 3 homologous proteins: IL-1α and IL-1β, which are proinflammatory proteins, and IL-1 receptor antagonist, an antagonist protein. These proteins are encoded by the genes IL-1α, IL-1β, and IL-1 receptor antagonist, respectively, which are clustered on chromosome 2q13–21. It was proposed that a particular genotype of IL-1 could predispose individuals to disease by enhancing the inflammation processes (Taylor and others 2004).
We investigated the +3954 C/T polymorphism in the exonic region of the IL-1β gene in our study. We could not find any significant difference in the genotype and allele distribution of the IL-1β (+3954 C/T) polymorphism between the main group of patients suffering from OLP and normal controls. This result was similar to the findings in the Brazilian population where the IL-1β (+3954 C/T) polymorphism was not related to OLP development (Xavier and others 2007). The IL-1β gene polymorphism at the exonic region of +3962 also showed no association with OLP in the Caucasian population (Carrozzo and others 2004).
However, the subgroup A of OLP having both CP and DM (OLP+CP+DM) against controls showed a striking observation with a higher frequency of the T allele (40.9%) (odds ratio=4.015), whereas subgroup B of patients suffering from OLP without CP and DM (OLP-CP-DM) showed no significant difference at all. Even the comparison between these 2 subgroups (A & B) showed a significant association in the genotypes and allele distributions with an odds ratio of 9.692. In an earlier study on CP from the Malayalam-speaking Dravidian population from South India using a case–control strategy, a significant association of the IL-1β gene polymorphisms with CP in Kerala was reported (Shete and others 2010). They found a high frequency of the C allele and CC genotype for the SNP IL-1β +3954 in the group with CP compared to controls, suggesting allele C of IL-1β +3954 to be an important risk factor for CP. Later, another study was done in the same South Indian (Kerala) population to investigate the role of the IL-1β (+3954 C/T) polymorphism in CP patients with DM (personal communication). On comparison, a higher frequency of the TT genotype and the T allele was observed in patients with both CP with DM as compared to patients with CP alone. Analyzing these data with our subgroup A (OLP + CP + DM) result, it might be suggested that DM may influence the expression of the T allele of IL-1β +3954 in patients suffering from OLP. Thus, IL-1β +3954 may have secondary effects on OLP induced by predisposition to comorbid factors.
IL-6 is produced by many types of cells and is one of the most important mediators of the inflammatory response, in which it may play a proinflammatory or anti-inflammatory role. It is well known that IL-6 is a proinflammatory cytokine strongly generated in OLP lesions.
The present study investigated the −597G/A polymorphism located in the promoter region of the IL-6 gene. Although most of the studies have evaluated the association of the IL-6 −174G/C polymorphism in many inflammatory diseases, assessment of the nearby polymorphic sites at −597 is also crucial, as it is found in a perfect linkage disequilibrium with IL-6 −174 in the South Indian Kerala population. Thus, the −597G/A polymorphism influences the polymorphism at position −174, which might be associated with altered plasma levels of IL-6. It has been reported in few studies that the GG genotypes of −597 G/A are associated with increased expression of IL-6. Hence, studies with IL-6 −597 can also reflect the observation from IL-6 −174, as it is in a perfect linkage disequilibrium with IL-6 −174 in our study population. As of yet, no studies have investigated the direct role of IL-6 −597 or imputed role of IL-6 −174 in OLP among the South Indian populations or any other world population.
On analysis of the IL-6 −597 polymorphism, there was no significant difference in the allele or genotype frequency between the OLP subjects and healthy controls. Even the different subgroups did not show any significant difference. A similar observation was made with the IL-6 −174 polymorphism in patients suffering from OLP from the Northern Italian population (Carrozzo and others 2004). In contrast, patients suffering from OLP had a significantly higher frequency of the GG genotype of the IL-6 −174 polymorphism (high-producer genotype) in the Brazilian population (Xavier and others 2007). The reason for this discrepancy may be attributed to inherent differences in the genetic constitution of the population due to different ethnic background. A more recent study on OLP in the Japanese population also reports a lack of association of the IL-6 −572 polymorphism (Fujita and others 2009). The results of our study suggest a possible lack of genetic modification in the IL-6 gene for susceptibility to OLP.
Conclusion
Genetic associations are almost always race specific, and the genotype of an individual is greatly influenced by his/her ethnic background. Even the allelic frequency distribution also varies from ethnicity to ethnicity. It is clear that the cytokine gene polymorphisms have an unquestionable role in the orchestration of the immune response, leading to different functional scenarios, which in turn influence the outcome of the disease establishment and evolution.
Our study is possibly the first study in India that has attempted to understand the role of cytokines in OLP. It is not the genes alone, but the interplay of genetic and environmental factors, which determine the disease phenotype. The limitations and the strength of the present study are that it makes a strong observation in our study population, but it may not be interpretable for a pan-Indian scenario, as the samples were selected from a strong ethnic background with limited environmental influences. Further studies in larger and more diverse populations are required to confirm whether these polymorphisms either individually or in haplotypic combination can provide evidence for better diagnostic and therapeutic values in the future.
Footnotes
Author Disclosure Statement
No competing financial interests exist.