
Abstract
To compare the early postarrest inflammatory cytokine response between animals administered amiodarone (AMIO) and lidocaine (LIDO) intra-arrest during resuscitation from ventricular fibrillation (VF). Domestic swine (n=32) were placed under general anesthesia and instrumented before spontaneous VF was induced by balloon occlusion of the left anterior descending coronary artery. After 7 min of VF, standard ACLS resuscitation was performed and animals were randomized to either bolus AMIO (5 mg/kg, n=13) or LIDO (1 mg/kg, n=14) for recurrent or refractory VF. A non-antiarrhythmic (n=5) was also used for comparison. Following return of spontaneous circulation (ROSC), tumor necrosis factor (TNF)-α levels were drawn at 30 and 60 min. Groups were comparable with respect to prearrest hemodynamics and resuscitation variables. In the postarrest period, the LIDO and non-antiarrhythmic group demonstrated virtually identical TNF-α response trajectories. However, TNF-α levels were significantly higher in AMIO- than LIDO-treated animals at 30 min (geometric mean 539 versus 240 pg/mL, 2.2-fold higher, 95% confidence interval [CI] 1.3–3.8-fold higher, P=0.003) and at 60 min (geometric mean 570 versus 204 pg/mL, 2.8-fold higher, 95% CI 1.1–7.0-fold higher, P=0.03). Significant differences in the postarrest TNF-α levels were observed between animals treated with AMIO as compared to those treated with LIDO. Improved rates of ROSC seen with AMIO may come at the expense of a heightened proinflammatory state in the postcardiac arrest period.
Introduction
Prolonged global ischemia and reperfusion injury contribute to the sepsis-like pathophysiology of myocardial dysfunction, hypotension, and coma that characterizes the postcardiac arrest syndrome in many survivors and is responsible for high inhospital mortality (Adrie and others 2004; Stub and others 2011). Inflammatory cytokines have been observed to mediate myocardial dysfunction in vitro (Kao and others 2010) and in animal models of cardiac arrest (Niemann and Garner 2004; Kern and others 2008) and to correlate with mortality in humans (Ito and others 2001).
Conflicting data exist regarding the immunomodulatory effects of AMIO in various settings in vitro and in vivo with some investigations measuring proinflammatory effects (Oral and others 1999; Nakajima and others 2001) and others measuring anti-inflammatory properties (Matsumori and others 1997; Ito and others 2002; Hirasawa and others 2009). To our knowledge, no data exist to measure its effects in the postarrest period when administered as part of cardiopulmonary resuscitation efforts.
The purpose of this study was to compare the serum response of tumor necrosis factor (TNF)-α, the master regulator of inflammatory cytokines, in the immediate postarrest period following administration of either AMIO or LIDO during arrest.
Materials and Methods
This study was approved by the Institutional Animal Care and Use Committee at LABioMed and conforms to the American Physiologic Society's Guiding Principals in the Care and Use of Animals.
The present report is a secondary analysis of 32 male Yorkshire and Yorkshire/Hampshire crossbreed domestic swine (mean weight 39.2±4 kg) that served as the control arm in a study of postresuscitation TNF-α blockade for the treatment of postcardiac arrest myocardial dysfunction. (32 animals, not represented in this analysis, failed to achieve ROSC or survive to a 60-min postarrest.) Animals were randomized to either AMIO or LIDO before the experiment using a permuted bloc design. We limited the study to male animals based on earlier work demonstrating a differential cytokine response following cardiac arrest by gender (Niemann and others 2008). With the exception of ad libitum access to water, animals were fasted overnight before the experiment. Animals were sedated with intramuscular ketamine (20 mg/kg) and xylazine (2 mg/kg) followed by isoflurane via nosecone to induce a general plane of anesthesia. Animals were then intubated and isoflurane and nitrous oxide in a 1:1 mixture with oxygen was administered to maintain general anesthesia. Minute ventilation was titrated to achieve an end-tidal CO2 at 35–45 mm Hg as measured by sidestream capnometry. Lead II of the surface ECG was monitored throughout the protocol.
High-fidelity, micromanometer tipped catheters (Millar Instruments, Houston, TX) were then surgically placed under fluoroscopic guidance with transducers positioned in the ascending aorta, left ventricle (LV), and the right atrium (RA). A thermistor-tipped catheter (Edwards Lifesciences, Irvine, CA) was placed in a branch of the pulmonary artery for the measurement of thermodilution cardiac output (CO). Standard adhesive defibrillation electrode patches were applied to the left and right lateral aspects of the shaved thorax. A tetrapolar constant current impedance measuring system (THRIM®, Morro Bay, CA) was used to measure transthoracic impedance and a small-value noninductive resistor (30Ω) was placed in series with a biphasic defibrillator (LifePak 12; Medtronic Emergency Response Systems, Redmond, WA). Following instrumentation, the heart rate and intravascular pressures were recorded continuously (Power Lab Chart v. 5.2; ADInstruments, Colorado Springs, CO). Arterial blood was drawn to measure control TNF-α values and perform blood gas analysis (I-Stat CG8+; I-Stat Corp, Princeton, NJ).
To induce VF, a standard angioplasty catheter with balloon was positioned in the left anterior descending coronary artery just distal to the first septal perforator and inflated to 8–12 atmospheres. The site of coronary occlusion and confirmation of complete cessation of coronary flow distal to the balloon was confirmed with manual contrast injections. VF followed spontaneously in all animals in this study. On induction of VF, ventilation was discontinued.
After 7 min of untreated VF, a time interval chosen to model a reasonable emergency medical services response interval for witnessed arrest, manual chest compressions at a rate of 100/min with force sufficient to depress the sternum 1.5 to 2.0 inches were initiated with the animal in the supine position. After 1 min of chest compressions, a 200 J biphasic shock was delivered and followed by additional shocks in an escalating energy sequence (300, 360 J) with interposed chest compressions if the first shock failed to terminate VF. Subsequent shocks were delivered at 360 J with 1–2 min of compressions between each shock. Positive pressure ventilations with FiO2 1.0 were initiated at a rate of 8 ventilations/min after the first shock. Adrenaline 1 mg IV was administered via the RA catheter after the first three shocks and repeated every 3–5 min unless ROSC occurred. For refractory or recurrent VF not responsive to the first three escalated shocks, we administered either AMIO (5 mg/kg, n=13) or LIDO (1 mg/kg, n=14). Five animals were resuscitated after 1 to 3 shocks and did not receive antiarrhythmic therapy. These animals served as a control group. The investigators were not blinded to antiarrhythmic administered. After 30 min, animals remaining in a nonperfusing rhythm (VF, asystole, and pulseless electrical activity) were considered resuscitation failures and the resuscitation efforts were terminated.
For the purposes of these experiments, ROSC was defined as an arterial systolic blood pressure of at least 60 mm Hg for >20 min. Only those animals achieving ROSC and surviving 60 min were included in this experiment. Once ROSC was obtained, hemodynamic monitoring and cytokine sampling occurred at 30 and 60 min. Arterial blood samples were placed in sterile, chilled (0°C), heparinized tubes, and centrifuged at 5000 rpm for 10 min. The supernatant plasma was separated and refrigerated at −80°C until analysis. TNF-α concentrations were measured using a quantitative sandwich ELISA specific for this porcine cytokine (R&D Systems, Inc., Minneapolis, MN).
Data analysis
Data were entered into an Excel Spreadsheet (v. 12.0; Microsoft Corp, Redmond, WA) and imported into SAS statistical software (v. 9.2; SAS Institute, Cary, NC) for analysis. Summary measures are reported as means and standard deviations (SD) or medians and interquartile ranges, as appropriate for the underlying distribution. Control values were compared using the Kruskal–Wallis test or analysis of variance. Generalized linear mixed models were used to compare TNF-α responses between groups over time during the post-ROSC period. Due to a right-skewed distribution, TNF-α values were natural log transformed before analysis. Time was entered into the model as a random effect along with its squared value to allow for curvature of the response trajectory, based on inspection of scatter plots and a better model fit as assessed by Akaike's Information Criterion. We assumed an unstructured covariance matrix for random effects. Antiarrhythmic assignment was entered into the model as a fixed effect. Due to the potential for residual confounding by resuscitation time (time from resuscitation onset to ROSC), we categorized resuscitation times into quartiles and modeled their independent association with TNF-α trajectories without respect to the antiarrhythmic assignment. All P-values used in the analysis are two sided.
Results
There were no differences in the prearrest TNF-α levels, hemodynamics, or LV function between groups (Table 1). Summary measures of resuscitation characteristics were likewise similar (Table 2).
Values are mean (Standard Deviation) or median (Interquartile Range).
MAP, mean arterial pressure; LVSW, left ventricular stroke work; TNF, tumor necrosis factor.
Reported as mean (Standard Deviation) or median (Interquartile Range).
ROSC, return of spontaneous circulation.
In the early postarrest period, TNF-α levels followed a similar trajectory among LIDO-treated animals and those that received no antiarrhythmics (Fig. 1). By contrast, levels were, on average, higher in animals treated with AMIO when compared to LIDO-treated animals at 30 min (geometric mean 539 versus 240 pg/mL, 2.2-fold higher, 95% CI 1.3–3.8-fold, P=0.003) and at 60 min (geometric mean 570 versus 204 pg/mL, 2.8-fold higher, 95% confidence interval 1.1–7.0, P=0.03).
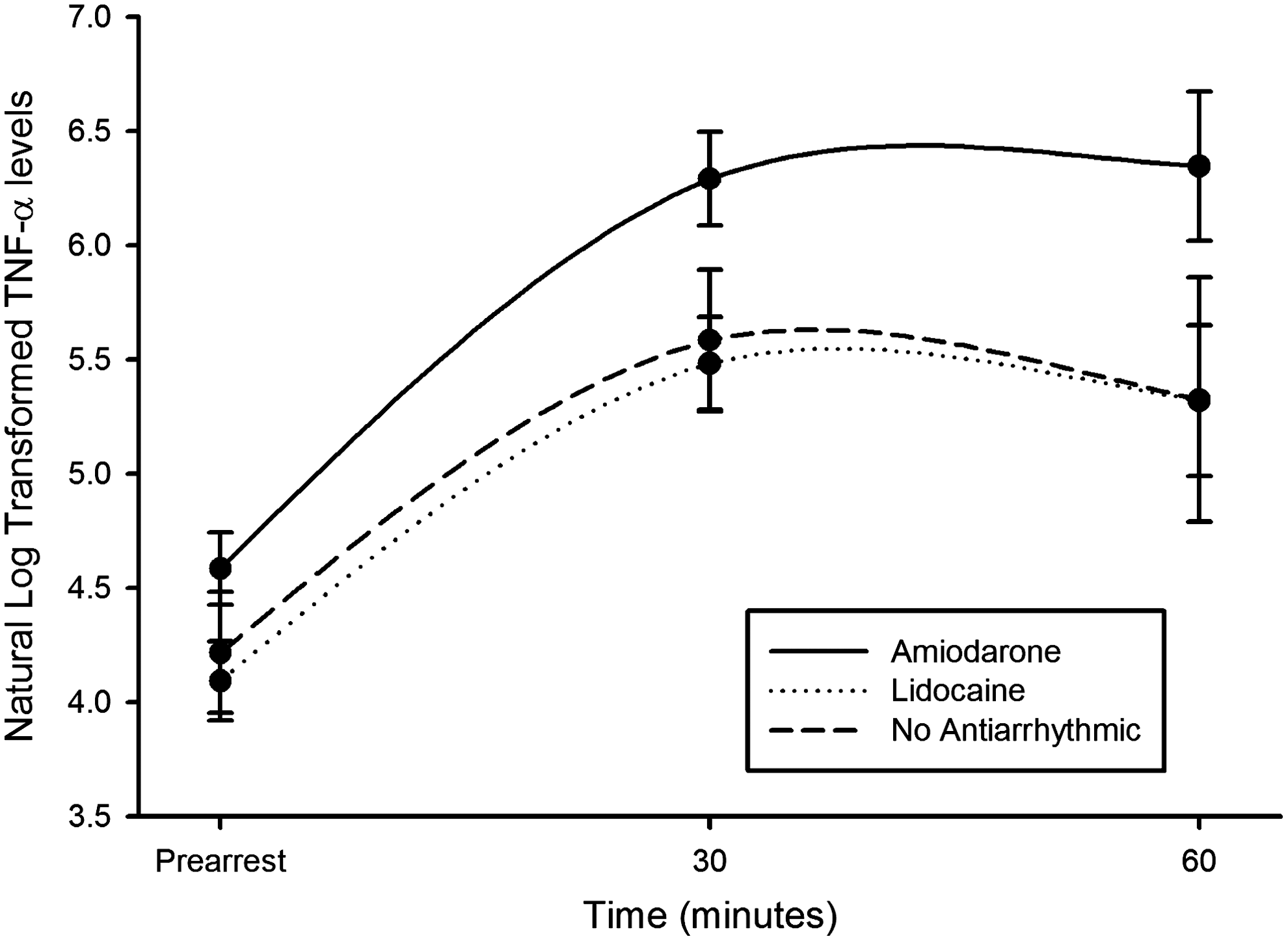
Mean natural log transformed values for tumor necrosis factor (TNF)-α during the early postarrest period between animals administered amiodarone or lidocaine for refractory or recurrent ventricular fibrillation (VF) or non-antiarrhythmic in a swine model of ischemic VF (original scale in pg/mL).
We found no trend or statistical association between time to ROSC (resuscitation time) and TNF-α levels (Fig. 2).
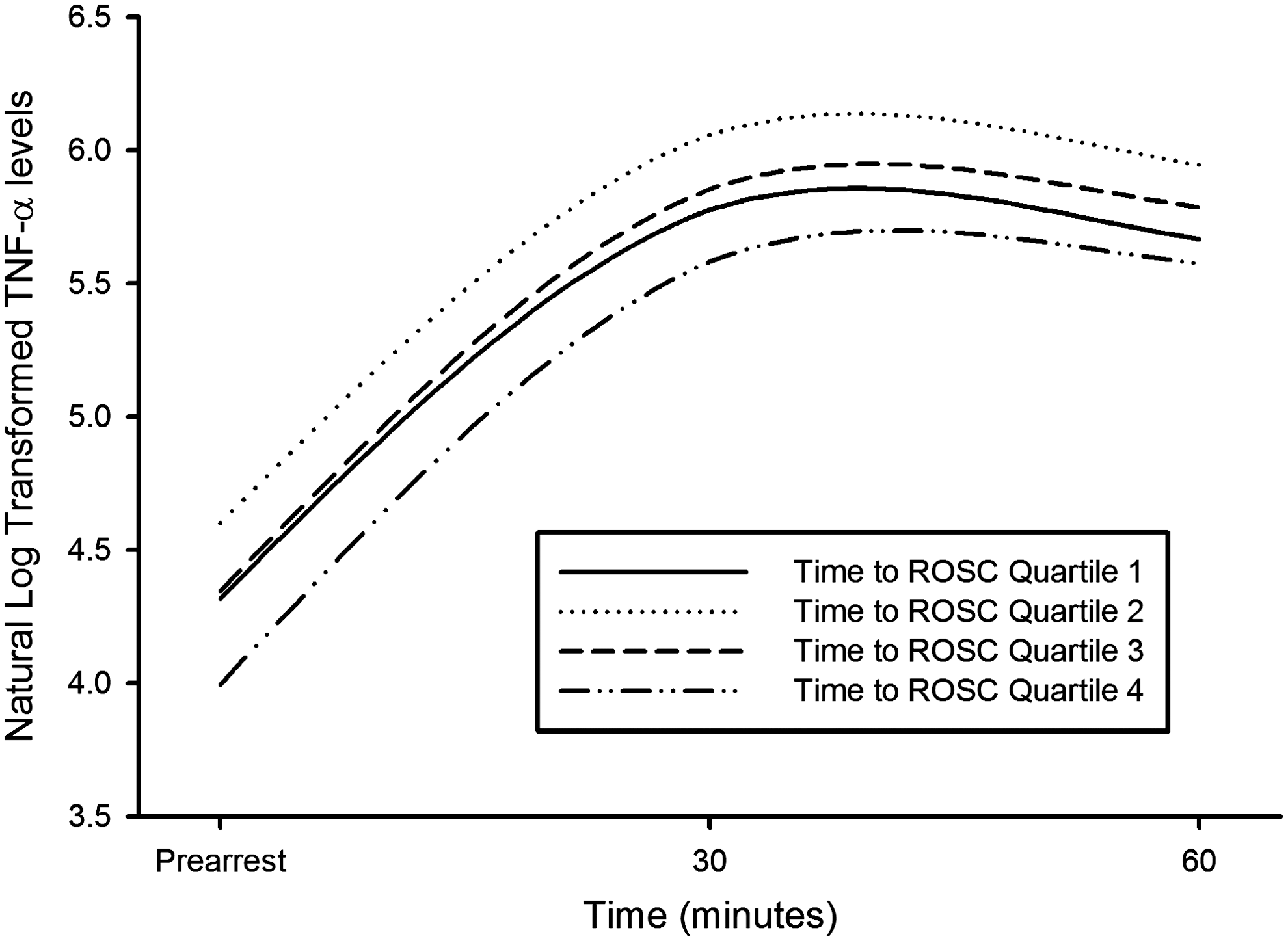
Mean natural log transformed values for TNF-α during the early postarrest period comparing quartiles of time to return of spontaneous circulation.
Discussion
Our investigation provides evidence that the antiarrhythmic, AMIO, when administered during resuscitation of VF, results in a more vigorous TNF-α response to ischemia/reperfusion in the early postarrest period than does LIDO. This effect does not appear to be confounded by time required to achieve ROSC.
Few studies have investigated the association between AMIO administration and the inflammatory cytokine response. In vitro studies have demonstrated both inhibitory effects on TNF-α production in some cell lines (Matsumori and others 1997) and proinflammatory effects in others (Nakajima and others 2001). In a mouse model of viral myocarditis, AMIO administration demonstrated anti-inflammatory effects (Ito and others 2002). Observational data in humans when using AMIO 7 days before and 48 h after coronary artery bypass grafting or as a single dose at the onset of anesthesia did not seem to significantly alter the course of postoperative inflammatory cytokine production (Karth and others 2007; Rahman and others 2009). Peripheral blood mononucleocytes drawn from patients with dilated cardiomyopathy demonstrated less propensity to produce TNF-α in response to C-reactive protein stimulation ex vivo if the patient had been prescribed AMIO (Hirasawa and others 2009). However, in a randomized trial of AMIO versus placebo for treatment of patients with CHF and ventricular ectopy (CHF-STAT study), AMIO-treated patients with ischemic cardiomyopathy demonstrated higher levels of TNF-α at 12 months. This effect was not observed in patients with nonischemic cardiomyopathy (Oral and others 1999).
Given the wide variety of experimental protocols, settings, and timing of measurements, these earlier investigations are poorly suited for comparison with the current study. We are unaware of previous work describing the effects of AMIO on the postcardiac arrest inflammatory response in either animals or humans.
Human studies of AMIO have demonstrated higher rates of admission to hospital without concomitant improvements in survival to hospital discharge when compared with LIDO (Dorian and others 2002) or placebo (Kudenchuk and others 1999). It follows that increases in ROSC following AMIO must be offset by a higher than expected inpatient mortality for reasons that are, as yet, unknown. A heightened postarrest inflammatory state following resuscitation with AMIO, as suggested by the present investigation, may be expected to worsen postarrest hemodynamics and LV function and neurologic outcome, leading to higher rates of inpatient mortality.
Limitations
This study has several limitations. We used only male swine because previous work has demonstrated that the postresuscitation inflammatory response in males is more robust than that observed in female swine of similar age (Niemann and others 2008). The anesthetics used in this study may have affected the prearrest and postresuscitation innate inflammatory response (Wu and others 2012). However, the anesthetic regimen was the same for the two treatment groups. Only one dose of each antiarrhythmic was used. A smaller or greater weight-based dosing might yield different results. However, the selected doses are those used clinically. Lastly, the long-term outcome was not evaluated in this study. It is possible that differences in the TNF-α response observed in the early postarrest period would not have led to important differences in a neurologically intact survival.
Conclusions
In summary, the rise in TNF-α in the early postarrest period is accentuated in animals treated with AMIO during resuscitation as compared to LIDO or no antiarrhythmic. The clinical implications of this finding are unclear, but such differences in the inflammatory response may be a mechanism to explain the lack of a long-term survival benefit observed in controlled human trials.
Footnotes
Acknowledgment
Funded, in part, by a grant from the NIH NHLBI R01 HL076671.
Author Disclosure Statement
No competing financial interests exist.