
Abstract
Preterm premature rupture of membranes (PPROM) is defined as a spontaneous membrane rupture that occurs before the onset of labor and 37 weeks gestation. Subclinical intrauterine infection has been suggested as a very important etiological factor in the pathogenesis and subsequent morbidity related with PPROM. This study was performed to assess the levels of maternal proadrenomedullin (pro-ADM) and serum amyloid A (AA) in PPROM and its association with fetomaternal infectious morbidity. A total of 63 pregnant women, of which 43 with PPROM between 24 and 34 weeks gestation and 20 normal pregnant women without PPROM were included in the study. The study group was separated into 2 subgroups as PPROM and PPROM-histological chorioamnionitis (PPROM-HC). The blood samples were taken before the administration of any medication. The mean serum interleukin-6 (IL-6), AA, and pro-ADM values in the PPROM-HC group were significantly higher than the PPROM and control group. The cutoff values of pro-ADM and AA were determined as 4.2 nM and 69 μg/mL, respectively. Both of them showed similar sensitivity, specificity to IL-6 and a better sensitivity and specificity as compared to C-reactive protein and white blood cell count. We determined the predictive value of pro-ADM and serum AA measurements in PPROM and PPROM with histological chorioamnionitis. We suggest using pro-ADM and serum AA biomarkers for detecting the histological chorioamnionitis at an earlier stage in PPROM without any clinical signs.
Introduction
P
Subclinical intrauterine infection has been implicated as a major etiological factor in the pathogenesis and subsequent morbidity associated with PPROM, but once clinical chorioamnionitis is present, there is a 4-fold increase in neonatal mortality (McParland and Bell 2004). MIAC has been found in 20%–50% of patients with PPROM, although clinical evidence of infection is present in as few as 12.5% of those women with positive culture results (Goldenberg and others 2008).
To determine the infection in the early stage by commonly used laboratory variables such as the sedimentation rate, C-reactive protein (CRP), white blood cell count, neutrophil count, or vaginal bacterial culture is usually difficult. Beside these difficulties, clinical signs such as fever and fetomaternal tachycardia usually occur late (Trochez-Martinez and others 2007).
Adrenomedullin plays an important role in regulating blood volume; it also has potential antimicrobial effects, which have a protective effect against organ damage, particularly in the setting of sepsis (Hinson and others 2000). Its serum levels show rapid elevations during sepsis, followed by rapid clearance from the circulation, which makes it difficult to detect because of its half-life of 22 min. Proadrenomedullin (pro-ADM), a more stable precursor molecule to adrenomedullin, was reported to correlate well with other markers such as interleukin-6 (IL-6) and CRP as a predictor of prognosis in patients with sepsis (Ehlenz and others 1997). Elevations of pro-ADM have been reported in systemic inflammatory response syndrome, sepsis, and septic shock in adults (Ueda and others 1999; Eto 2001).
Serum amyloid A (AA) has similar patterns in most inflammatory diseases, reaching a maximum serum concentration about 24 h after the inflammatory process sets in, and then slowly decreasing. The AA protein is an apolipoprotein that rapidly binds to high-density lipoprotein after their synthesis, influencing cholesterol metabolism during inflammatory states, causing adhesion and chemotaxis of phagocitic cells and lymphocytes. Current studies showed that AA has been considered very effective and might be a better acute phase reactant than CRP to monitor or diagnose viral and bacterial infections (Patel and others 1998; Lannergard and others 2003).
Although there were intensive studies in finding an effective consensus to the management of PPROM, an enough satisfactory consensus for PPROM does not exist. To determine the infection in the early phase in PPROM will give us an opportunity to reduce the risk of maternal infections and neonatal complications. Therefore, this study was performed to assess the levels of maternal serum AA and pro-ADM in PPROM and its association with fetomaternal infectious morbidity.
Materials and Methods
A total of 63 pregnant women, of which 43 pregnant women presenting with PPROM between 24 and 34 weeks gestation and 20 normal pregnant women without PPROM (matched for age, parity, and gestation age with the study group), were included in the study. Subjects with confirmed PPROM not in labor, not having clinical chorioamnionitis, were enrolled in the study. PPROM is diagnosed when visualization of a pool of fluid in the posterior vaginal fornix with evident fluid passing from the cervical canal. Patients with hypertension, immunological disorders, antepartum hemorrhage, multiple gestation, medical disorders, polyhydramnios, heart disease, and diabetes mellitus and patients with evidence of any other infection, such as urinary tract infections, were excluded from the study. The study group was separated into 2 subgroups as only PPROM and PPROM-histological chorioamnionitis (PPROM-HC). Hematoxylin and eosin-stained slides of placental tissues were reviewed by a pathologist blinded for laboratory levels. Histological chorioamnionitis was diagnosed as proposed by the Amniotic Fluid Infection Nosology Committee. The Institutional Review Committee approved the study, and parents signed a written informed consent.
The control group consisting of 20 cases of normal pregnancy with intact membranes was enrolled. The samples were taken before the administration of any medication. All patients with PPROM were given injection ampicillin 500 mg 6 hourly for 48 h, followed by oral capsule amoxicillin for 7 days. Venous blood was collected from subjects and controls for total leucocyte count (TLC), CRP, IL-6, AA, and pro-ADM.
TLC was performed using an automatic counter, Cell Dyn 3700 (Abbott Diagnostics Division). CRP determination was performed by using Roche-Hitachi® 912 analyzer (Roche Diagnostics). The samples for IL-6 were studied by the enzyme-linked immunosorbent test (Bender Medsystems®) according to the manufacturer's instructions. Samples of serum were diluted 1:20, 1:500, or 1:5,000, and then tested through ELISA on 96-well microtiter plates (Phase Range Serum Amyloid A Assay, Tridelta Development Limited). MR-proADM was measured using a new sandwich immunoassay (MR-proADM; BRAHMS). Intra-assay imprecision was under 10% over the entire measuring range, and the functional assay sensitivity (interassay coefficient of variation <20%) was 0.12 nM. pro-ADM levels were considered normal when <4 nM based in the median value of pro-ADM observed in healthy adults (Christ-Crain and others 2005).
Statistical analysis
Statistical analysis was performed with SPSS 12.0 software (IBM). Data are expressed as mean±standard deviation. The Chi-square or Fisher's exact test was used to compare categorical variables, and the Wilcoxon Rank Sum test was used to compare continuous variables. The correlations among numerical data were analyzed by the Pearson correlation coefficient (r). For TLC, CRP, IL-6, Pro-ADM, and AA variables that showed a statistically significant difference between the 2 groups, receiver operating characteristic (ROC) curves were obtained to calculate the cutoff values optimized to reach the best compromise in the prediction of increased IL-6, serum AA, and pro-ADM values. Optimal cutoff was defined as a threshold, where the sum of sensitivity and specificity was maximum. A P value<0.05 was considered statistically significant.
Results
Clinical characteristics of the study groups
The characteristics of the 43 study groups and 20 control groups are summarized in Table 1. Both the study group and control group showed no significant differences in terms of maternal age (years), gravity, parity, and gestational age at admission. The study group was separated into 2 subgroups as only PPROM and PPROM-HC.
P<0.05 Control versus PPROM.
P<0.05 Control versus PPROM-HC.
P<0.05 PPROM versus PPROM-HC.
AA, amyloid A; CRP, C-reactive protein; IL-6, interleukin-6; PPROM, preterm premature rupture of membranes; PPROM-HC, PPROM-histological chorioamnionitis; TLC, total leucocyte count.
TLC, CRP, and IL-6 measurements
The PPROM group had significantly higher TLC (12800±1370 vs. 11200±1550/mm3), CRP (9.2±3.4 vs. 0.6±0.52 mg/dL), and IL-6 (2.23±2.52, 6.22±1.58 pg/mL) measurements than controls; however, in the PPROM-HC group, the mean serum TLC (14500±1280 vs. 12800±1370/mm3), CRP (19±2.1 vs. 9.2±3.4 mg/dL), IL-6 (14.91±13.8 vs. 6.23±3.41 pg/mL) measurements were significantly higher than the PPROM group (Table 1). The cutoff of CRP in the present study was determined as 10.3 pg/mL and this value was found to predict infectious morbidity in PPROM with a sensitivity of 78% and specificity of 72%. The cutoff of IL-6 in the present study was determined as 9.6 pg/mL and this value was found to predict infectious morbidity in PPROM with a sensitivity of 91% and specificity of 90%. The area under the curve (AUC) values was 0.687 for TLC, 0.883 for CRP, and 0.938 for IL-6.
Pro-ADM and AA measurements
The PPROM group had significantly higher pro-ADM (6.22±1.58 vs. 1.22±1.52 nM) and AA (69±9 vs. 8.2±4.52 μg/mL) measurements than controls; however, in the PPROM-HC group, the mean pro-ADM (13.2±2.2 vs. 6.22±1.58 nM) and AA (179.2±22 vs. 69±9 μg/mL) levels were significantly higher than the PPROM group (Table 1) (Fig. 1). Maternal and perinatal outcome (cesarean section for fetal distress, gestational age at birth, birthweight, stillbirth, puerperal sepsis, neonatal sepsis, neonatal mortality, spontaneous preterm labor, spontaneous delivery <7 days of admission) with pro-ADM <4.2 nM and AA <69 μg/mL as the cutoff (Table 2). The AUC values for pro-ADM and AA were 0.912 and 0.917, and the ROC curve of all markers are shown in Fig. 2.

IL-6, serum AA, pro-ADM levels in groups. The PPROM-HC group had significantly higher serum IL-6, pro-ADM, AA measurements levels than the PPROM and control groups. IL-6, interleukin-6; SAA, Serum Amyloid A; PPROM, preterm premature rupture of membranes; PPROM-HC, PPROM-histological chorioamnionitis; pro-ADM, proadrenomedullin.
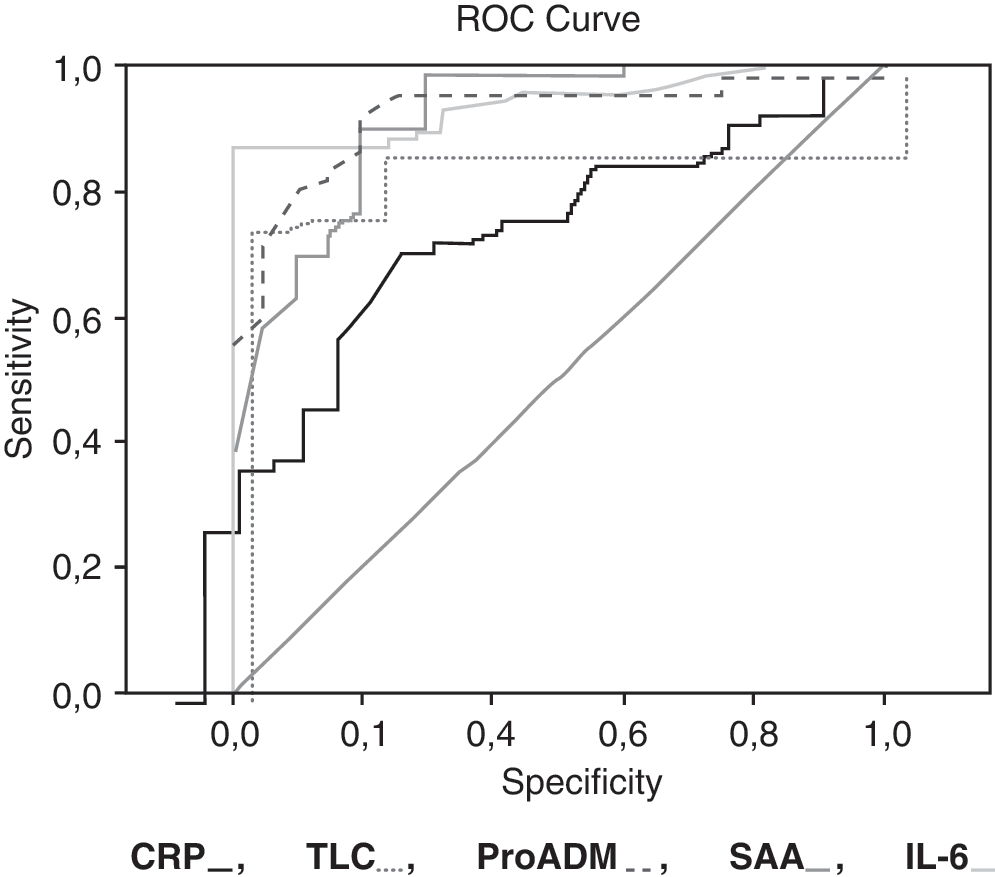
Receiver operating characteristic (ROC) curves of pro-ADM, serum AA, CRP, IL-6, and total leucocyte count (TLC) measurements according to prediction of chorioamnionitis. The cutoff values for predicting infectious morbidity in PPROM was determined as 4.2 nM for pro-ADM (sensitivity of 87% and specificity of 88.2%), 69 μg/mL for serum AA (sensitivity of 88% and specificity of 90%), 10.3 pg/mL for CRP (sensitivity of 78% and specificity of 72%), 9.6 pg/mL for IL-6 (sensitivity of 91% and specificity of 90%). CRP, C-reactive protein.
P value<0.05 was considered statistically significant.
Correlations between pro-ADM and the other markers
Previous studies have shown that pro-ADM measurements for prediction severity and outcome of sepsis found it was a very useful biomarker for using in sepsis (Oncel and others 2012; Suberviola and others 2012). We found significant correlations between pro-ADM and the other sepsis markers such as TLC (r: 0.211; P<0.05), CRP (r: 0.423; P<0.01), IL-6 (r: 0.521; P<0.01), and AA (r: 0.635; P<0.01). And the other marker in this study, AA, had significant correlations between TLC (r: 0.242; P<0.05), CRP (r: 0.488; P<0.01), and IL-6 (r: 0.583; P<0.01). All correlations are shown on Table 3.
Correlation is significant at the 0.05 level (2-tailed).
Correlation is significant at the 0.01 level (2-tailed).
Cutoff values for pro-ADM and serum AA
The cutoff of pro-ADM in the present study was determined as 4.2 nM and this value was found to predict infectious morbidity in PPROM with a sensitivity of 87% and specificity of 88.2%. Arnon and others (2007) showed that serum AA had an overall better diagnostic accuracy for predicting early onset sepsis in full-term infants. In this study, we found that serum AA was nearly effective as IL-6 to predict the subclinical chorioamnionitis in PPROM. The cutoff of serum AA in the present study was determined as 69 μg/mL and this value was found to predict infectious morbidity in PPROM with a sensitivity of 88% and specificity of 90%.
In literature, there are studies (Kacerovský and others 2009; Vousden and others 2011; Gulati and others 2012) with especially measurement of IL-6 to determine the subclinical chorioamnionitis in patients with PPROM. However, we found the cutoff value of pro-ADM of 4.2 nM and the cutoff of serum AA of 69 μg/mL showed similar sensitivity, specificity to IL-6, and the better sensitivity and specificity as compared to CRP and TLC in predicting infection in PPROM.
Discussion
This cross-sectional study provides evidence that pregnant women with PPROM exhibit increased levels of some inflammatory markers such as TLC, CRP, IL-6, pro-ADM, and AA. Among them, pro-ADM and AA were noted to be consistently higher in the PPROM with subclinical chorioamnionitis even if there are no clinical signs. To our knowledge, this is the first study that evaluates the increased early biomarkers such as pro-ADM and AA in the group of pregnant women with PPROM and PPROM with chorioamnionitis. Infection and/or inflammation secondary to histological chorioamnionitis has been well recognized to have a strong and casual link with preterm birth. Although chorioamnionitis has a more immediate impact in terms of triggering of preterm labor and birth, there have been multiple studies evaluating the short- and long-term effects on the fetus and premature neonate (Romero and others 2007). Many studies showed that chorioamnionitis caused multiorgan diseases (intraventricular hemorrhage, cerebral palsy, periventricular leukomalacia, mental retardation, psychiatric disorders, fetal growth restriction and poor neonatal growth, bronchopulmonary dysplasia, respiratory distress syndrome, early-onset sepsis, retinopathy of prematurity, necrotizing enterecolitis, dermatitis, etc.) (Williams and others 2000; Westas and others 2008; Dammann and others 2009; Shatrov and others 2010). Because of these reasons, it is vital to determine and treat chorioamnionitis even if there is no clinical sign before it is too late.
In literature, there are studies with especially IL-6 to determine the subclinical chorioamnionitis in patients with PPROM. Gulati and others (2012) showed that a cutoff value of IL-6 of 8 pg/mL was found to correctly diagnose 19 out of 23 patients with infectious morbidity, showed the best sensitivity (82.6%) and specificity (86.3%), and found a significant association with puerperal sepsis and neonatal sepsis. Vousden and others (2011) showed that the measurement of vaginal IL-6 on bedside was useful in guiding patients with visible membranes and PPROM. Kacerovský and others (2009) found that amniotic fluid IL-6 concentration patients with PPROM with the presence of MIAC and histological chorioamnionitis were significantly higher than IL-6 concentration patients without histological chorioamnionitis and MIAC. Andrys and others (2010) evaluated the cord blood concentrations of IL-6, IL-8, and matrix metalloproteinase-8 and found that IL-6 was very effective in the diagnosis of histological chorioamnionitis and funisitis in patients with preterm PPROM. In another study, Lockwood and others (2010) examined decidual cell during chorioamnionitis and concluded that high expression of IL-6 during HC cause decidual monocyte differentiation to macrophages. Skrablin and others (2007) showed significantly higher IL-6 and CRP levels than PPROM with subclinical, but histopathological chorioamnionitis and found a strong association with periventricular leukomalacia and connatal infection. Canpolat and others (2011) examined the diagnostic sensitivity and specificity of CRP and procalcitonin in neonates who were born after PPROM, compared these with IL-6 and found that IL-6 was the most reliable marker for the detection of early-onset sepsis in preterm neonates with PPROM and early procalcitonin levels seemed to be more sensitive than early CRP in this population. In our study, we found that IL-6 was good predictor for determination of subclinical chorioamnionitis.
Adrenomedullin has a bactericidal activity, which is begun by its regulation and involving of complement and other immune system cell activities (Marutsuka and others 2001). In many studies, serum levels of adrenomedullin were shown to be increased in sepsis and mechanisms of this were thought that might be first, adrenomedullin is widely expressed and extensively synthesized, similar to other calcitonin peptides, including procalcitonin and calcitonin gene-related peptides, because adrenomedullin is a member of the CALC gene family and second, decreased clearance by the kidneys (Hirata and others 1996; Becker and others 2004). Pro-ADM is the stable active substance and has a longer half-life than adrenomedullin. Therefore, we selected pro-ADM for evaluation of determining chorioamnionitis and concluded that pro-ADM was nearly as effective as IL-6 to predict the subclinical chorioamnionitis in PPROM. Suberviola and others (2012) conducted a study in severe sepsis and septic shock and found that Pro-ADM levels correlate with increasing severity of illness and death. In a current study about evaluation of pro-ADM levels in neonatal sepsis, Oncel and others (2012) found that the use of pro-ADM in combination with other acute-phase reactants such as CRP and IL-6 for the diagnosis and follow-up of patients with neonatal sepsis had high sensitivity and specificity. Wang and Kang (2010) studied pro-ADM and pro-atrial natriuretic peptide for prediction severity and outcome of sepsis, and found that both of them were very useful biomarkers for using in sepsis.
Serum AA is another biomarker studied first in rheumatologic and chronic inflammatory diseases, but after then, many studies showed that it can be reliable in acute inflammatory diseases. CRP and AA display a similar pattern in most inflammatory diseases and serum AA concentrations usually parallel to CRP. Nakayama and others (1993) reported that AA appears to be a clinically useful marker of inflammation in bacterial or viral infection like CRP. Some authors showed that AA was a more sensitive marker than CRP in infections with a low-inflammatory activity (including many viral infections) and in other clinical conditions, especially those involving the lung tissue (Huttunen and others 2003; Lannergard and others 2003). Cetinkaya and others (2009) studied AA in neonatal sepsis and concluded that AA was a reliable marker for diagnosis and follow up of neonatal sepsis and it was especially useful at the onset of inflammation for rapid diagnosis of neonatal sepsis and could be safely used in combination with other sepsis markers such as IL-6, CRP, and procalcitonin in diagnosis and follow up of neonatal sepsis.
In summary, we found that serum pro-ADM and AA levels are significantly elevated in patients with PPROM and PPROM having subclinical chorioamnionitis, as compared with controls. And also, we determined the predictive value of pro-ADM and AA measurements for detecting the subclinical chorioamnionitis in women with PPROM. Although further confirmation is necessary in different cohort groups and infectious diseases, we would like to suggest that both of these markers can be used as reliable biomarkers to detect an infection without any clinical signs in pregnant women.
Footnotes
Author Disclosure Statement
The authors do not have any conflicts of interest to disclose.