
Abstract
Antibodies to interferon-beta (IFNb) may occur during treatment with this drug and can be measured at several levels, the totality of antibodies referred to as antidrug antibodies (ADA) or binding antibodies, and in case of interference with the drug activity referred to as neutralizing antibodies (NAB). Antibodies can also interfere with the biological activity of IFNb as measured by pharmacodynamic markers. To get a complete picture of the interference between IFNb as a drug and the ADA, all the 3 above levels need to be considered. Furthermore, the interaction of these biomarkers changes over time with a shift of antibody properties with respect to immunoglobulin subtypes, affinity, and titers of antibodies. In case of persistent NAB, the clinical benefit of IFNb in the treatment of multiple sclerosis is abolished. In this report, the current knowledge on these issues will be reviewed. The data have been presented at a meeting in Coral Gables, Florida on April 18–21, 2012.
Introduction
A
The occurrence of ADA in a patient on treatment with a BP does not necessarily lead to a loss of the drug's efficacy; however, if there is a loss of efficacy due to antibodies, one can assume that the antibodies block, or neutralize, the drug and then are referred to as neutralizing antibodies (NAB; in the less recent literature, one will also find the term blocking antibodies). The distinction between ADA and NAB is difficult because there is no assay measuring ADA and NAB at the same time. This dichotomy is illustrated in Fig. 1 for the example of interferon-beta (IFNb) antibodies.
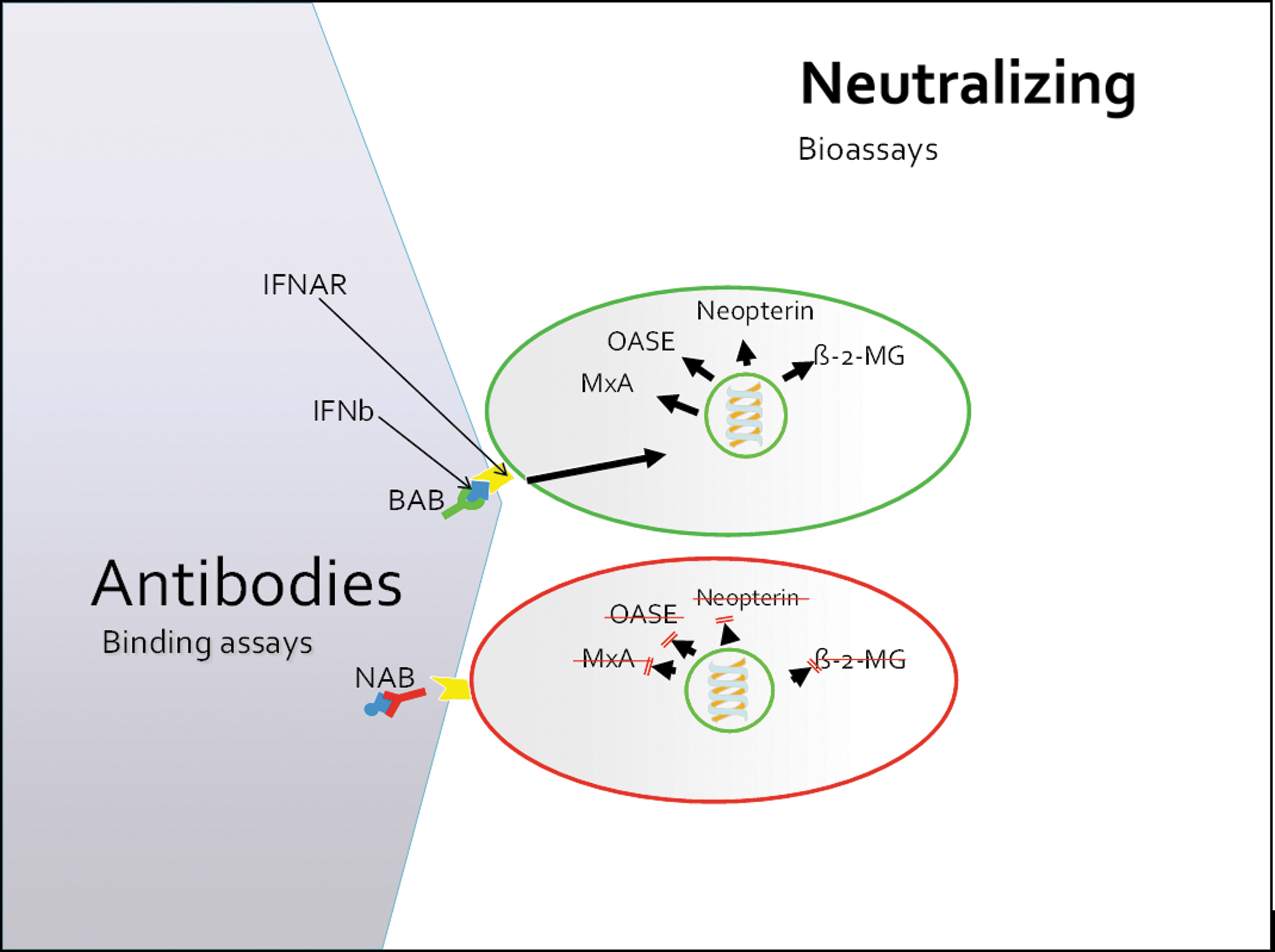
This figure illustrates the dichotomy of neutralizing antibody testing. On the left, the antibody side of testing is depicted. Binding of type I interferons (IFN alpha and beta) to the type I interferon receptor (IFNAR) induces the upregulation of several hundred gene products, such as myxovirus resistance protein (MxA), oligo-A-synthetases (OASE), Neopterin, and beta-2-microglobulin (β-2-MG). Antibodies against interferon may not interfere with binding of the IFN molecule to its receptor and are then referred to as binding antibodies (BAB). On the other hand, if antibodies block binding of interferons to the receptor, they are referred to as neutralizing antibodies (NAB). Simple antibody tests such as enzyme linked immunosorbent assay or Western blot are not able to distinguish between BAB and NAB. Therefore, for evaluation of the biological effect of IFN antibodies, the bioactivity of IFN needs to be assessed, which is shown on the right-hand side of the figure. Principally, all IFN-induced gene products may serve as outcome measure of IFN activity, but their sensitivity and specificity vary substantially.
As an additional feature in the interaction between the drug, ADA, and NAB, pharmacokinetics (PK) and/or pharmacodynamics (PD) can add to the understanding of the effect of ADA and NAB. If the BP is a monoclonal antibody, PK can be measured with relative ease, whereas BP made of, for example, cytokines such as IFNb, PK measurement can be troublesome, and in such cases, PD needs to be assessed, which has its limitations by various factors such as sensitivity and specificity of the PD read-out as well as individual differences of the expression and the kinetic of the PD marker.
In this article, the relationship between ADA, NAB, and PK/PD by the example of IFNb will be reviewed, and finally, the context with clinical effects of IFNb antibodies will be addressed.
ADA, NAB, and PK/PD Measurements
ADA against IFNb can be measured by various methods, but enzyme linked immunosorbent assay (ELISA) techniques are applied by most investigators. Two different formats have been reported, a simple direct binding assay (dELISA) in which the antigen (ie, IFNb) is directly coated onto the plate followed by patients serum incubation and a conjugated anti-human antibody for ADA detection versus a slightly more complex assay in which the plates are coated with an anti-IFNb capture antibody (cELISA) followed by essentially the same procedure as in the above direct binding method. Some authors find the cELISA to be more sensitive and specific (Pachner 2003), others find the dELISA somewhat more useful than other ADA detection methods (Gneiss and others 2008). In the sequence of IFNb antibody testing in clinical routine as well as clinical trials, ADA assays are sometimes as a screening method before proceeding with a more elaborate and time-consuming NAB assay (Francis and others 2005; Kappos and others 2005; Sorensen and others 2005a).
The detection of NAB against IFNb is methodically somewhat more challenging. Use of cell cultures is inevitable because testing the biological effect (or the neutralization of it) requires the expression of the IFNb receptor, that is, the type I interferon receptor (IFNAR), on a cell surface. The read-out of the IFNAR activation can be performed at several levels. In earlier times, the global antiviral effect of IFNb has been assessed in the cytopathic effect assay, which required an additional viral culture to challenge cells after stimulation with IFNb. This method was recommended by the World Health Organization (WHO) until the advance of easier test systems (WHO Tech. Report Ser. 1996), such as the MxA induction assay, still recommended by the European Medicines Agency (2008). The latter does not use viral cultures but relies on the quantification of an IFNb-specific gene product, the myxovirus resistance protein A (Files and others 1998). More recently, the procedure of NAB testing has been further simplified by using a much quicker read-out by transfecting cells with a luciferase reporter gene, which emits light almost immediately on stimulation (Lam and others 2008). This method is the first NAB assay commercially available making result easier comparable across different laboratories.
The quantification of interferon neutralization has been a constant source of confusion. In this context, there are 3 terms that require some attention. Those are the neutralizing unit (NU), the 10-fold reduction unit (TRU), and the laboratory unit (LU), very nicely reviewed by Grossberg and others (2001a, 2001b). In brief, the least standardized term is NU, which has been used by various authors arbitrarily, for example, the amount of antibodies neutralizing 1 U of IFN, or the highest serum dilution that completely inhibits 5 U of IFN per mL (Protzman and others 1984; Antonelli and others 1991), just a few examples among many others.
The TRU has been introduced to make titer calculations more comparable across different methods and laboratories. If a bioassay system uses a standard curve with 5 international units (IU)/mL IFN as the highest concentration, the serum dilution reducing the IFN activity to 0.5 IU/mL would then correspond the TRU titer. In a different laboratory or assay, the standard curve might start at 20 IU/mL and the corresponding TRU titer would then be the serum dilution that reduces the IFN activity to 2 IU/mL. To make titer calculations better comparable across laboratories and assay systems, the highest concentration of the standard curve will be set as 10 LU/mL with 1 LU/mL as the titration endpoint, which can then be used for titer calculations according to the Kawade formula (1980) that corrects to some extent for the differences of absolute IFN concentrations. In clinical studies, a cutoff titer of 20 NU or TRU is often used because lower titers are hard to reproduce and the IFN activity may be reduced in samples with higher titers (see section “PD and NAB”).
PK measurements are very difficult due to the short half-life and the very low concentration of IFNb after subcutaneous application (Alam and others 1997). Therefore, at least in clinical settings, PD has been used to assess the bioavailability of IFNb. There is a vast array of PD markers available with varying sensitivity and specificity as well as very different temporal kinetics, the latter mainly depending on whether it is measured at the protein or the RNA level. One of the most frequently used PD markers is MxA and appears to stand for all other IFNb-induced gene products (Hesse and others 2009).
How Do ADA and NAB Relate to Each Other?
As illustrated in Fig. 1, there is no way to date to assess ADA and NAB in one single assay. Since drug interference in IFNb treatment can be neglected, it is assumed that ADA assays detect all circulating antibodies against IFNb according to the immunoglobulin (Ig) subtype of the secondary antibody used in the assay, which is mostly IgG (Deisenhammer and others 2001). Some authors suggested that all antibodies possess certain capacity of neutralization, and it is only a matter of NAB assay sensitivity to detect those (Ross and others 2000). There are, however, a few pieces of evidence hinting at a difference between ADA-positive samples in which NAB can be detected as opposed to samples without detectable NAB as outlined in the next paragraph.
Using linear peptide epitopes of IFNb, it could be shown that NAB-positive and NAB-negative sera recognize different peptides and the binding strength as well as the influence on the bioactivity of IFNb differs. In one study, the N-terminal end seemed to have the strongest binding capacities for NAB-positive samples and NAB titers correlated significantly with antibody titers against the peptide sequence close to the N-terminal end of the IFNb molecule (Gneiss and others 2004). Interestingly, a study introducing point mutations at different sites found that mutations at the alpha helix including the N-terminus did not change the binding and activity properties of IFNb (Runkel and others 2001; Gneiss and others 2004). Together with the finding of NAB binding to the N-terminus, this might indicate that NAB do not inhibit receptor binding by blocking the binding site but probably by other mechanisms, such as conformation changes or steric hindrance.
The binding strength between IFNb and ADA has been investigated by dividing samples in NAB-positive and NAB-negative sera by measuring relative affinity values or dissociation rates (Gneiss and others 2006a; Gibbs and Oger 2008). The studies showed concordantly that the affinity was higher in NAB-positive samples and that it increased over time indicating affinity maturation.
Furthermore, the Ig profile of NAB-positive versus NAB-negative (but ADA positive) samples differs with a clearly higher proportion of IgG2 and IgG4 in NAB-positive sera. There was also a strong correlation between NAB and IgG4 titers, which was not seen with other subtypes and total ADA titers (Deisenhammer and others 2001). This observation is in line with data from other chronic exposure studies showing a shift toward IgG4 in long-term immunization (Aalberse and others 1983). IgA and IgM do not appear to play a relevant role in the neutralization of IFNb (Deisenhammer and others 2001).
PD and NAB
As mentioned above, there is a great variety of PD markers that are more or less specific for IFNb. So far MxA quantification, be it on RNA or protein level, has been used most widely. Overall, there is a clear negative correlation between NAB titers and MxA levels.
It is however difficult to determine a clear cut-point between IFNβ response and nonresponse. Previously, a cut-point between NAB positivity and negativity in a single test of 20 NUs was often used (The IFNB Multiple Sclerosis study group and others 1996; Francis and others 2005; Kappos and others 2005). Later, it turned out that the grey zone between NAB negativity and positivity cannot be drawn at a certain NAB titer but rather lies between 20 and 600 NU (Deisenhammer 2009). The use of different antigens in the NAB assay is at least partially responsible for this finding. If a sample is tested against IFNb 1a, a 3- to 6-fold higher NAB titer is obtained compared with testing the same sample against IFNb 1b. This can be explained by the higher absolute amount of protein load in IFNb 1b at a comparable unitage. One unit of IFNb-1b has a roughly 5- to 10-fold higher protein concentration compared to various IFNb-1a preparations. Therefore, 1 U of IFNb-1b is able to bind more antibodies than IFNb-1a resulting in above-mentioned difference of calculated NAB titers (Bertolotto and others 2000). Therefore, using comparable weight units of IFNb in different assays results in less interassay variation than using comparable IU of different interferons.
A lack of PD expression in a given IFNb-treated patient does not necessarily indicate the presence of and especially persistency of NAB. Samples for PD measurements need to be collected close to the injection because most PD markers reach peak levels within 12 h (Pachner and others 2006) and decrease rapidly thereafter. Patients sometimes forget or refuse to inject, which would then result in low or nonexistent levels of the PD marker (Twork and others 2007) and one might falsely conclude that NAB were responsible. If IFNb injection and timing can be ascertained, a lack of PD induction very likely indicates the presence of NAB above a certain titer but does not allow to estimate NAB titers beyond this level and can therefore not be used for the prediction of NAB persistency.
In practical terms, PD markers can be used particularly in patients with constant intermediate NAB titers to determine the individual level of neutralization. Such titers may be due to background noise in the assay, and in these patients, PD expression will be detected.
NAB and Type of Interferon Preparation
IFNb in the treatment of multiple sclerosis (MS) comes in 3 different licensed products not to mention biosimilars that are mostly marketed in developing markets. Here, only the licensed products in the United States and European Union will be discussed. IFNb-1b is produced in Escherichia coli, therefore lacks glycosylation, is truncated by one amino acid at the N-terminus, and has a cysteine-to-serine substitution at position 17. It is injected at a dose of 250 μg every other day subcutaneously (sc). IFNb-1a produced in Chinese hamster ovaries has an identical primary structure as human IFNb and is glycosylated. Two different IFNb-1a preparations are available, one in 30 μg portions and once weekly intramuscular (im) application, another in 22 or 44 μg portions for sc application trice weekly. Their immunogenic potential differs substantially with IFNb-1a for im application showing the lowest NAB prevalence of up to 5% (Gneiss and others 2006b). IFNb-1a for sc application induces NAB in around 19% of patients (this figure applies for patients who were exclusively treated with the new formulation of this product) (Giovannoni and others 2009), and∼31% of IFNb-1b-treated patients develop NAB during exposure to this drug (Hegen and others 2011). These NAB prevalence rates need to be put in context as NAB titers and kinetics as well as persistency rates are important factors for the clinical effects. Particularly in terms of NAB kinetics and persistency, IFNb-1a and 1b products need to be separated. NAB induced by IFNb-1a products tend to have higher average peek titers, which occur somewhat later (at year 3) than NAB induced by IFNb-1b at around year 2 (Hegen and others 2011). Consequently, NAB induced by IFNb-1b revert earlier and in a higher proportion of patients to negativity (Sorensen and others 2005b).
There are differing physicochemical characteristics that might explain some of these observations. The binding site of NAB against IFNb-1a and 1b seems to be different. NAB induced by IFNb-1a showed stronger binding patterns at the CD loop and D helix regions of IFNb, whereas NAB induced by IFNb-1b bound predominantly at the AB loop (Brickelmaier and others 1999). Others found titers of ADA from NAB-positive samples to have higher titers against the N-terminal peptides of IFNb when induced by IFNb-1a compared with IFNb-1b (Gneiss and others 2004). Also, IFNb antibodies obtained from NAB-positive patients have higher binding strength to IFNb compared with ADA-positive but NAB-negative patients. The affinity of ADA increases over time on treatment indicating an affinity maturation process. Furthermore, antibodies induced by IFNb-1a have an higher affinity than antibodies induced by IFNb-1b specifically when tested against the originally inducing INFb product, that is, antibodies induced by IFNb-1a bind stronger to IFNb-1a than 1b and vice versa (Gneiss and others 2006a). It is likely that this is controlled by the individual's antigen-processing pathways in antigen presenting cells (Hoffmann and others 2008), although the link to affinity maturation has not been formally investigated.
Another well-known factor contributing to immunogenicity is the drug formulation. One of the IFNb-1a preparations induced a relatively high NAB rate of 22% (at week 104 after treatment initiation) in the first clinical trial (Jacobs and others 1996). Subsequently, the manufacturing process has been modified including the removal of human serum albumin and other changes leading to the reduction of aggregation and oxidation (Barnard and others 2013) and consequently to a low rate of NAB (Jacobs and others 2000). A successful formulation change has been introduced for another IFNb-1a preparation with subcutaneous application, again removing HAS (Giovannoni and others 2007).
NAB Evolution
A model of how NAB and ADA develop over time with respect to their physicochemical characteristics is shown in Table 1.
ADA, antidrug antibodies; NAB, neutralizing antibodies; IgG, immunoglobulin G.
The temporal kinetics of NAB against IFNb is relatively slow with antibodies evolving over roughly 2 years and starting to revert in the following years. Transient antibodies occurring in some patients revert usually at earlier time points (Bellomi and others 2003). The generally accepted but formally not proven theory for the late development and reversion of NAB in IFNb therapy is breaking followed by re-induction of tolerance.
The important criterion for clinical relevance of NAB is their persistency and, because of the very long-term kinetics, the prediction of persistency at earlier time points. As pointed out above, antibody kinetics differ between IFNb-1a- and 1b-treated patients, and therefore, predictors of persistency need to be separately analyzed and determined. Prediction of NAB using NAB titers has been reported by several authors and consistently shown that cutoff titers for the prediction of NAB persistency in patients on IFNb-1a are lower than in patients on IFNb-1b. Cutoff titers for NAB prediction lie between 400 and 500 NU for IFNb-1b and around 250 NU for IFNb-1a (Petkau and others 2004; Herndon and others 2005; Sorensen and others 2005b; Hegen and others 2011). This fact has not been considered in earlier version of NAB guidelines (Sorensen and others 2005a) but was recommended in a recent position paper of the NABINMS group (
As NAB occur late after initiation of IFNb therapy one might be interested if total ADA occur earlier and if they might be predictive of NAB development. In a small series, it could be demonstrated that in patients who eventually turn NAB-positive ADA titers boosted earlier during therapy and then paralleled with NAB titers. This could not be observed in patients who remained NAB negative and had constantly low ADA levels (Mayr and others 2003). This finding was followed up during the NABINMS project, and it turned out that ADA titers at 3 months into IFNb treatment had a very high predictive value of NAB positivity at 2 years (work submitted).
Clinical Relevance of NAB
The vast majority of studies investigating the clinical effects could show a clear association between NAB and loss of efficacy as measured by magnetic resonance imaging (MRI) outcomes. MRI is often used as primary endpoint in phase II and as secondary endpoint in phase III MS trials because it is more sensitive than clinical outcomes, although the relationship between MRI and clinical activity has still not been perfectly established (Hyland and Rudick 2011). Clinical outcomes in MS mainly include relapse rates and disease progression measurements by a scoring system called EDSS (standing for expanded disability status scale), which spans from zero (ie, no complaints and normal neurological examination) to 10 (death due to MS) (Kurtzke 1983). Relapse rates are less frequent than MRI activity, and disease progression evolves even slower. Consequently, these outcomes are less sensitive and therefore are less clearly associated with the loss of IFNb efficacy due to NAB (Table 2). One factor that needs to be considered is the observation period. As discussed above, NAB occur late and clinical effects are thus detectable even later. Accordingly, studies with longer observation periods more frequently show a negative effect of NAB on clinical endpoints rather than studies with observation times of less than 2 years (Deisenhammer 2009). Due to various factors, relapse frequencies (usually expressed as annualized relapse rate) in MS patients are lower in clinical trials conducted in the past 10 years compared to earlier studies (Goodin 2008) and so it becomes even more difficult to detect NAB effects on relapse rates. Another issue in the stratification of study populations into NAB-positive and NAB-negative cohorts is the definition of NAB positivity related to a group of patients over time as opposed to sample-related definitions. Some analyses stratified all patients into the NAB-positive group who had one single or 2 consecutive positive test results just above the cutoff titer. This leads to the inclusion of patients with short-term transient NAB in whom IFNb efficacy is only minimally affected in long-term analyses. This phenomenon has been nicely shown by setting different NAB cutpoints for patient stratification demonstrating clearly stronger effects in patients with higher NAB titers and persistently positive test results (Polman and others 2003).
+, statistically significant reduction of IFNb effects in NAB-positive groups.
(+), statistically nonsignificant reduction of IFNb effect in NAB-positive groups.
−, no measurable difference between NAB-positive and NAB-negative groups. +/−, equivocal results if more than one outcome variables were measured in this category (eg, effect on T2 lesions, but not on T1 gadolinium enhancing lesions).
Includes annual relapse rate, time to relapse, and proportion of relapse-free patients.
Does not relate to the difference between NAB-positive and NAB-negative patients but to the difference between NAB and placebo groups.
Relates to the whole study period of 0–48 months.
IFNb, interferon-beta; MRI, magnetic resonance imaging; sc, subcutaneously; im, intramuscular; RR, relapsing MS; MS, multiple sclerosis; SPR, secondary progressing relapsing MS; CIS, clinically isolated syndrome; NR, not reported.
It is, however, still widely accepted that high titer NAB negatively influences IFNb efficacy on clinical, paraclinical, and biological levels. This has been appreciated by guidelines of the American Academy of Neurology (AAN) as well as the European Federation of Neurological Societies (EFNS), although the AAN consortium found the level of evidence less compelling than the EFNS group (Sorensen and others 2005a; Goodin and others 2007). More recently, the NABINMS study group (
An overview of clinical NAB effects in the literature is shown in Table 2.
Conclusion
NAB against IFNb is a very complex issue with a few particular aspects. In most patients, they appear transiently even though they might persist over many years. Also, NAB occur relatively late during IFNb treatment, and therefore, the clinical effects were not detected in short-term studies. The incidence of NAB depends strongly on the IFNb preparation with a range of 2% to roughly 31% but different kinetics in terms of time to peak titer and rate of seroreversion. So far, high titer NAB is the best surrogate marker for IFNb (non)-response. Because NAB assays do not measure antibodies per se, one must not only measure NAB titers but also PD markers as well as total anti-IFNb antibody titers (ADA) to understand the complexity of IFNb neutralization on a group level. In individual patients, the NAB titer usually gives enough information about the current biological activity of IFNb and also predicts persistency of NAB. In uncertain cases (such as persistent low-to-intermediate NAB titers), one could additionally measure PD markers. There is a moderate positive correlation between ADA and NAB titers, if antibodies neutralize IFNb or not probably depend on many physicochemical characteristics of ADA such as affinity, Ig isotype, the binding site at the IFNb molecule. Although there is no worldwide agreement, I believe that the EFNS is right in recommending NAB tests for all patients irrespective of the clinical status because NAB usually precede the clinical nonresponse.
Author Disclosure Statement
I have received personal compensation for advising and speaking for pharmaceutical companies marketing interferon-beta products in the treatment of multiple sclerosis.