
Abstract
Immunogenicity of biological agents leads to the development of antidrug antibodies (ADA) and it may be associated to hypersensitivity reactions. Immediate infusion reactions occur during or within 1 h after infusion, and their clinical manifestations vary considerably, ranging from mild to severe and life-threatening. Recent studies show that different mechanisms sustain hypersensitivity reactions toward biologics, and the application of novel methods for detecting ADA has demonstrated the involvement of specific IgE isotypes. Considering the severity of the reactions, it is important for clinicians to recognize their symptoms, to know their pathophysiological mechanisms, and to take risk assessment and prophylactic procedures. This review summarizes the clinical manifestations of antibody and nonantibody-mediated reactions as well as the humoral and cellular mechanisms of antidrug responses. Last, the management of patients at risk is discussed. The definition of diagnostic and prophylactic strategies represents an unavoidable need in the management of potentially reactive patients to improve the safety profile of biologics.
Introduction
T
The administration of any foreign drug is likely to be able to elicit both humoral and cellular responses from the immune system. In this review, we examine the clinical manifestations of antibody and nonantibody-mediated reactions as well as the humoral and cellular mechanisms of antidrug responses. Last, the management of patients at risk is discussed.
Clinical Manifestations of Acute Infusion Reactions to BA
Generally, AEs are defined as any untoward medical occurrence associated with the use of a drug in humans, whether or not considered drug related. Whereas any AE caused by a drug is defined as an infusion reaction. The term hypersensitivity refers to antibody- or cellular-mediated infusion reactions (Fig. 1). Infusion reactions may be divided into local and systemic. In the case of subcutaneous BA local infusion reactions are referred to an injection site reaction (ISR). The use of a BA carries potential risks of infusion reactions, including hypersensitivity manifestations (Borchers and others 2011; Pascual-Salcedo and others 2011). Acute infusion reactions occur during or within 1 h after infusion, whereas delayed reactions occur from 1 h to 14 days (Pichler 2006). The clinical manifestations of both acute and delayed reactions vary considerably, ranging from mild to severe and life-threatening, thus important clinical consequences such as drop out therapy or fatal cases may occur. Among acute HRs, anaphylaxis represents the most severe event which may occur, characterized by respiratory distress, laryngeal edema, bronchospasm, accompanied by skin, gastrointestinal, and cardiovascular involvement. Increased vascular permeability, a hallmark sign of anaphylaxis, may allow a transfer of up to 50% of intravascular fluid into the extravascular space within few minutes. Acute infusion reactions may occur at the first dose or during the course of treatment, thus suggesting different underlying pathogenic mechanisms. In fact, they may be sustained by an antibody-dependent or independent pathogenic mechanism. Concerning antibody-dependent mechanisms, different antidrug antibody (ADA) isotypes may be involved (IgE and non-IgE). We usually define an Ig-dependent AE as being an HR. It is important to underline that IgE- and IgG-mediated reactions may be clinically indistinguishable. Although pre-existing cross-reacting ADA may be involved as in the case of cetuximab-induced reactions, the development of ADA usually results from repeated exposure to BA and it is associated to reactions occurring after initial doses. In particular, infliximab infusion reactions cluster around the first 8–10 infusions and thereafter become sporadic (Vultaggio and others 2008; Lee and others 2011; Matucci and others 2013). On the other hand, among non-antibody-dependent events, the cytokine release syndrome (CRS) due to a massive release of cytokines by several mechanisms is the best characterized condition. In most cases, CRS is a first dose effect sustained by several immune effector cells (monocytes, macrophages, cytotoxic T cells, natural killer cells [NK]) and complement molecules. The above cells bind to the Fc portion of monoclonal antibodies (mAb) thus leading to cell destruction and subsequent release of cytokines. Sometimes, the CRS raises concern for immediate antibody-mediated hypersensitivity (Brennan and others 2009) (Fig. 2). We know that clinical manifestations of ADA-mediated reactions and CRS partially overlap: indeed, rash, hypotension, nausea, tachycardia, shortness of breath, and fever have been described in both types of reactions (Bugelski and others 2009; Vogel 2010). In addition, FcɛRI engagement may also play a role in the induction of CRS. In fact, FcɛRI-mediated mast cell/basophil activation leads to the release of inflammatory mediators such as TNF-α and other cytokines, involved in the CRS. Thus, CRS may belong to and amplify the classical IgE-mediated anaphylaxis.
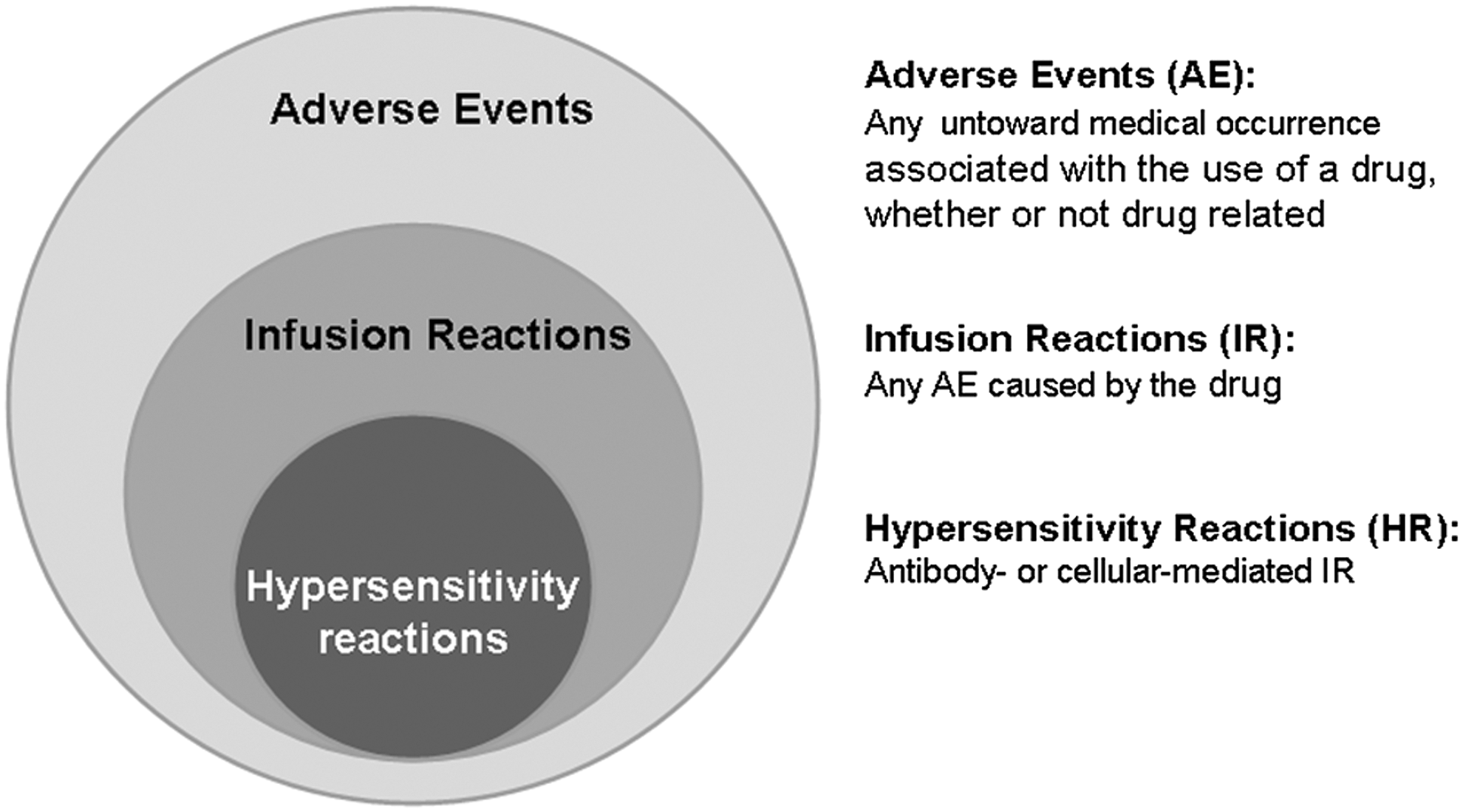
Definitions of adverse events, infusion reactions, and hypersensitivity reactions.
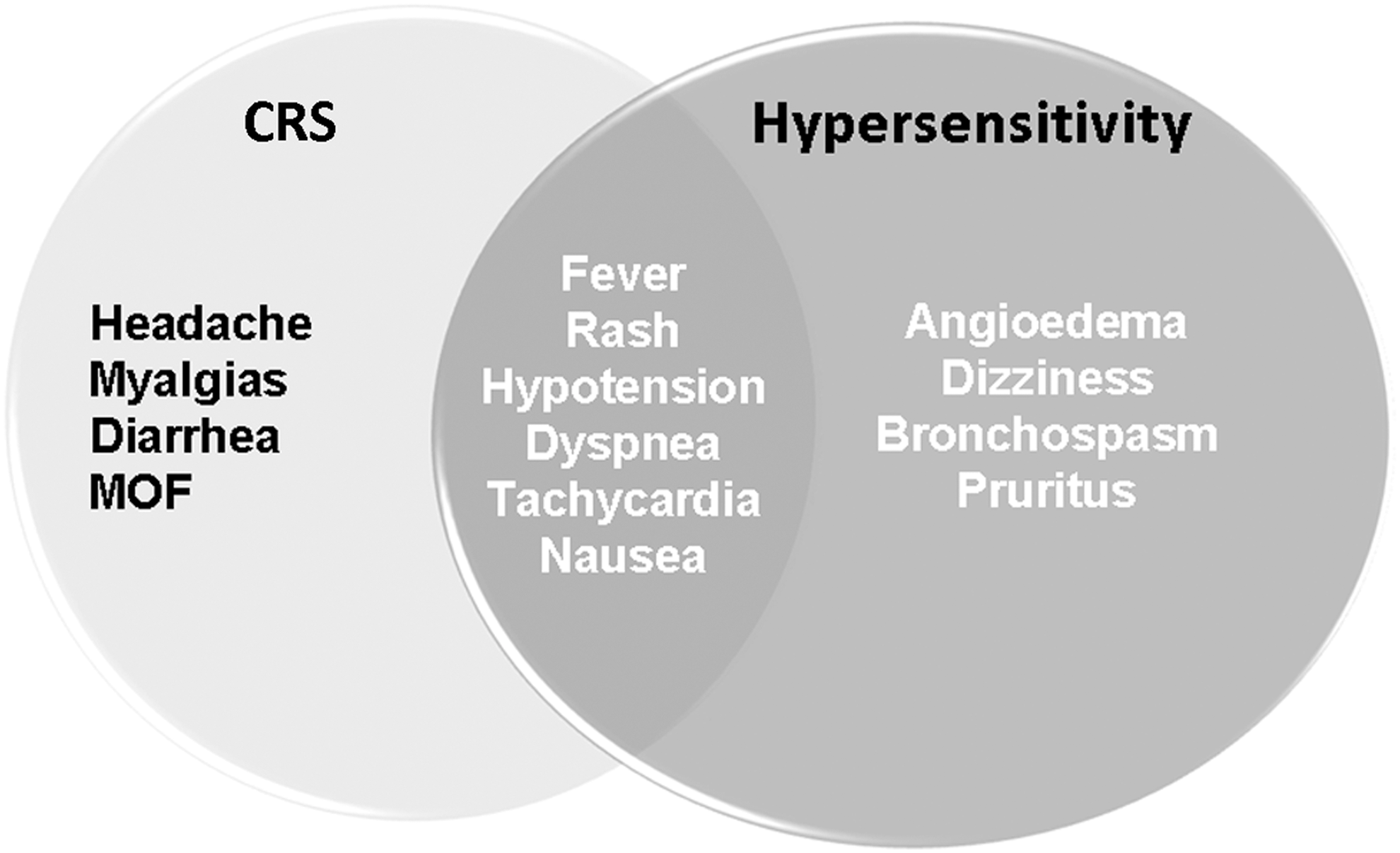
Clinical overlap between cytokine release syndrome (CRS) and antibody-mediated hypersensitivity. MOF, multiorgan failure.
Regarding subcutaneously administered BA, even if they can also induce systemic reactions, the most common AEs are represented by ISR, characterized by erythema, swelling, itching, or infiltrated plaques. ISR may occur within a few minutes (immediate reactions) or later (delayed reactions). ISR are not usually associated with the development of ADA.
Humoral and Cellular Antidrug Response in HRs
Virtually all BA are immunogenic, due to sequences that may be recognized by the recipient as nonself epitopes stimulating the immune system (Presta 2006; Hansel and others 2010) and inducing both cellular and humoral responses. The nonself epitopes mainly include xenoantigens present in the murine part leading to the production of anti-mouse antibodies. However, anti-allotypic-, anti-idiotypic, or anti-oligosaccharide chain antibodies have also been described. Among BA, the immunogenicity of mAbs has been well characterized. They are classified as chimeric (made from variable regions of a murine source and constant regions of a human immunoglobulin) or humanized (containing only the complementarity-determining regions of a murine immunoglobulin with the remaining part from a human source) and fully human (completely of human origin). It is important to note that also humanized or fully human mAbs induce antibodies against the idiotypic or allotypic sequence of the mAb. Patients developing ADA are more likely to show acute HRs, whereas definitive data on the role of ADA in the induction of delayed reactions are still lacking. Our previous data showed that the majority (72.7%) of patients suffering from an acute infliximab-related reaction resulted positive at the detection of ADA (Vultaggio and others 2010). Although ADA are mostly represented by IgG class (Svenson and others 2007), multiple isotypes (IgM, IgE, IgG) and subclasses (IgG1–4) can be produced during humoral antidrug responses. In fact, the presence of circulating BA-specific IgE antibodies, as well as skin testing positive for BA, have been described in a proportion of reactions to biologicals (Vultaggio and others 2010). Using the CAP system platform (ThermoFisher, Phadia, Uppsala, Sweden), we confirmed the hypothesis that infliximab-specific IgE Abs are involved in a proportion (27.2%) of reactive patients with immediate reaction associated with ADA positivity (Vultaggio and others 2010). The IgE-positive patients developed also a positive intradermal test at immediate lecture, thus confirming the biological activity (skin mast cells activation) of IgE ADA. Recent data correlate HRs with the outgrowth of serum IgE ADA for several mAbs, such as cetuximab, tocilizumab, natalizumab, and muromonab (Georgitis and others 1991; Chung and others 2008; Munoz-Cano and others 2010; Stubenrauch and others 2010; Timm and others 2010). In addition, for rituximab and trastuzumab, the positive results of skin testing supported an IgE-mediated mechanism of HRs, at least in some patients (Brennan and others 2009). As for rituximab, we recently showed that it can induce adverse reactions through an IgE-mediated mechanism, thus suggesting that type I hypersensitivity may be an additional pathway to CRS in the development of rituximab-related reactions. As observed in infliximab reactive patients, we also showed positivity of the intradermal test for rituximab. Furthermore, the appearance of rituximab-specific IgE ADA strictly correlated to the development of the AE (Vultaggio and others 2012a). Since the initial exposure is required for sensitization, IgE-mediated HRs cannot occur during the first infusion of a BA. However, pre-existing cetuximab-specific IgE antibodies have been detected that are directed against galactose-α-1,3-galactose residues (α3gal) present in the Fab portion of this mAb. Some studies report that α3gal is present in the gastrointestinal tract of ticks (Hamsten and others 2013) and that tick bites can induce IgE antibodies to a3gal thus suggesting that tick bites may be a cause of IgE response to cetuximab (Commins and others 2011).
Even if IgE have been clearly associated with anaphylaxis to biologicals, many results indicate that this classical pathway does not account for all HRs. Indeed, murine models revealed that neither mast cells nor IgE are essential for the development of allergen-induced anaphylaxis. In contrast, an alternative pathway driven by IgG and FcγRIII, has been shown in mice (Khodoun and others 2011). This latter mechanism is induced when high levels of antibodies are produced in response to high amounts of antigen administration and it is significantly improved upon in vivo depletion of basophils, but not macrophages, NK, or neutrophils, thus demonstrating that basophils are the main contributor to IgG-mediated anaphylaxis. In addition, murine models show that basophils are activated by an IgG receptor-driven mechanism and that they release PAF rather than histamine, upon stimulation (Tsujimura and others 2008). It is not feasible to directly demonstrate that IgG-mediated anaphylaxis occurs in humans, but it would be interesting to evaluate this pathway in individuals who have experienced adverse reactions to BA and with high levels of serum IgG, but not IgE specific to biologics. Taking into account that basophils usually circulate in the bloodstream, they are easily triggered by intravenously administered agents such as BA. The development of BA-specific IgG may lead to another effector mechanism involving the complement system with subsequent production of anaphylatoxins and then direct unspecific mast cell activation. To date, human markers that distinguish IgE- from IgG-mediated anaphylaxis have not been identified.
The measurement of serum tryptase, the classical mediator accounting for mast cell activation, is currently used and high levels are consistent with a true anaphylactic reaction. In a cohort of 20 infliximab reactive patients, normal serum tryptase levels were found after infusion reactions, which have been defined inconsistent with an IgE-mediated event (Cheifetz and others 2003). However, tryptase levels within the normal range do not exclude IgE-mediated anaphylaxis, as described in the majority of patients with fatal or near-fatal food-induced anaphylaxis (Sampson and others 1992). In these cases, the attention has been focused on basophils that express high-affinity FcɛRI and, after stimulation, release mediators but not tryptase.
There has been considerable effort to establish the role of MHC class II-restricted T-cell epitopes present in protein sequences and the development of humoral immune responses against BA. Several studies have shown that many therapeutic proteins, including recombinant human proteins such as IFNβ1b, induce cellular and humoral responses and that the removal or modification of an immunodominant epitope was sufficient to avoid the immune response. ADAs represent the result of the adaptive immune response to the drug, which also implies the presence of drug-specific memory T cells. Evidence that T-cell help is a central component of the immune response against BA comes from a number of observations, including the prominence of high-affinity responses comprising multiple IgG isotypes, such as those observed against infliximab and adalimumab (Bartelds and others 2010). Rituximab-stimulated peripheral blood mononuclear cells from a reactive patient, but not from controls, displayed a dose-dependent proliferative response associated with a Th2 cytokine production profile, able to sustain the IgE humoral response (Vultaggio and others 2012a). Preliminary data show that also infliximab-specific T cells are detectable in peripheral blood mononuclear cells some weeks after the reaction (Vultaggio A, in preparation). Furthermore, the presence of mechanisms involving peripheral tolerance, such as regulatory T cells, able to prevent the formation of ADAs, can be envisaged. Furthermore, anti-TNF-α mAbs may “di per sè” induce reverse signaling on membrane TNF-α expressing cells (activated CD4+ T cells, NK cells, and monocytes/macrophages) by promoting silencing signals on some genes and amplifying regulatory mechanisms (Xin and others 2006).
Factors Inducing Immunogenicity
The immunogenicity profile of a BA cannot be accurately predicted, being due to both patient- and drug-related factors. The management of safety of these agents is highly dependent on the recognition, and if feasible, prevention of such risk factors.
The patient-related factors include the patient's disease state, since the diffuse and acute inflammation leads to the high expression of costimulatory molecules on dendritic cells thus accelerating the development of T- and B-cell responses (Anderson 2005). The cellular and molecular pathogenic mechanisms underlying the disease may represent a milieu favoring the tolerance breakthrough and the subsequent reactions toward BA. For instance, an increased incidence of infliximab reactions in patients suffering from rheumatoid arthritis (RA) compared to patients suffering from seronegative spondiloarthritis and vasculitis was found (Vultaggio and others 2008). In addition, rituximab seems to be poorly immunogenic in patients with lymphoma, while induces ADAs in patients with systemic lupus erythematosus (van Walle and others 2007).
BA-specific T cells can be targeted pharmacologically during treatment to reduce the immunogenicity of the protein. The most frequent method includes the use of immunosuppressive therapies such as methotrexate or azathioprine. Clinical data obtained in patients who received infliximab infusion for Crohn's disease and rheumatological disorders indicate that concomitant therapy with immunosuppressors was associated with a reduced incidence of ADA development and a decreased, even if not abolished, risk of reaction (Farrell and others 2003; Colombel and others 2004; Sany and others 2005; Moss and others 2008). Accordingly, 12% of patients treated with certolizumab for bowel inflammatory disease developed ADAs, whereas the percentage decreases to 2% in patients with a concomitant immunosuppressive therapy (Stallmach and others 2010).
Other factors such as dosing and duration of treatment are also important in the development of ADA and HRs. The infliximab dosage in daily practice varies among different kinds of diseases. An inverse relationship between the drug dose and its immunogenicity has been reported in patients suffering from RA and Crohn's disease, indicating that high doses of infliximab are associated with low prevalence of ADA (Wasserman and others 2004; Moss and others 2008). Re-exposure following a long interval can trigger a secondary immune response and some reports indicate an increased proportion of BA reactions in patients who have discontinued therapy (Du Pan and others 2009). Adults and children with Crohn's disease experienced severe systemic reactions when a distant reinfusion interval was attempted (Kugathasan and others 2002). In our experience, intermittent therapy may favor ADA formation and increase the likelihood of infusion reaction. In our case series, 66.6% of infliximab-reactive patients displayed the infusion reaction during the second course of therapy after a variable period of discontinuation (Vultaggio and others 2008). Thus, the tolerance break toward the biological drug after a period of interruption may be hypothesized. It is likely that regular drug infusion may induce a high-dose tolerance through efficient peripheral mechanisms, which need the continuous antigen intake. Under a certain threshold concentration of circulating BA during treatment initiation or even after a therapeutic interruption, patients may be at high risk of immunization. Results obtained with desensitization for therapeutic mAbs (gradual reintroduction of small doses of drug at fixed time intervals until the delivery of the therapeutic dose), which are dependent on the ongoing antigen exposure, suggest the role for high-dose tolerance mechanism toward biological drugs and the relationship between HRs and the interruption of the therapy (Brennan and others 2009).
The role of prophylactic medication with acetaminophen and/or antihistamines and/or intravenous hydrocortisone in the prevention of ADA formation and HRs remains unclear. No randomized control study has been conducted comparing patients with or without this kind of pretreatment (Lecluse and others 2008). On the other hand, premedication with acetaminophen plus histamine blockers is recommended as prophylaxis for CRS induced by mAbs employed in cancer therapy (Vogel 2010). Furthermore, in contrast to antibody-mediated hypersensitivity, CRS may be managed by short-term cessation of the BA infusion and reduction of the rate infusion after restarting.
Monitoring Immunogenicity to Avoid HR
Although immunogenicity includes both humoral and cellular responses as described above, the immune response to biologicals is usually shown by the presence of serum ADAs. A multitiered testing strategy for assessment of immunogenicity is recommended. The initial ADA screening assay able to detect all ADA-positive samples must be followed by a confirmatory assay for distinguishing between true- and false-positive results. In addition, a further characterization of confirmed positive samples is needed to define the isotype and the neutralizing activity of the induced ADAs (Fig. 3).
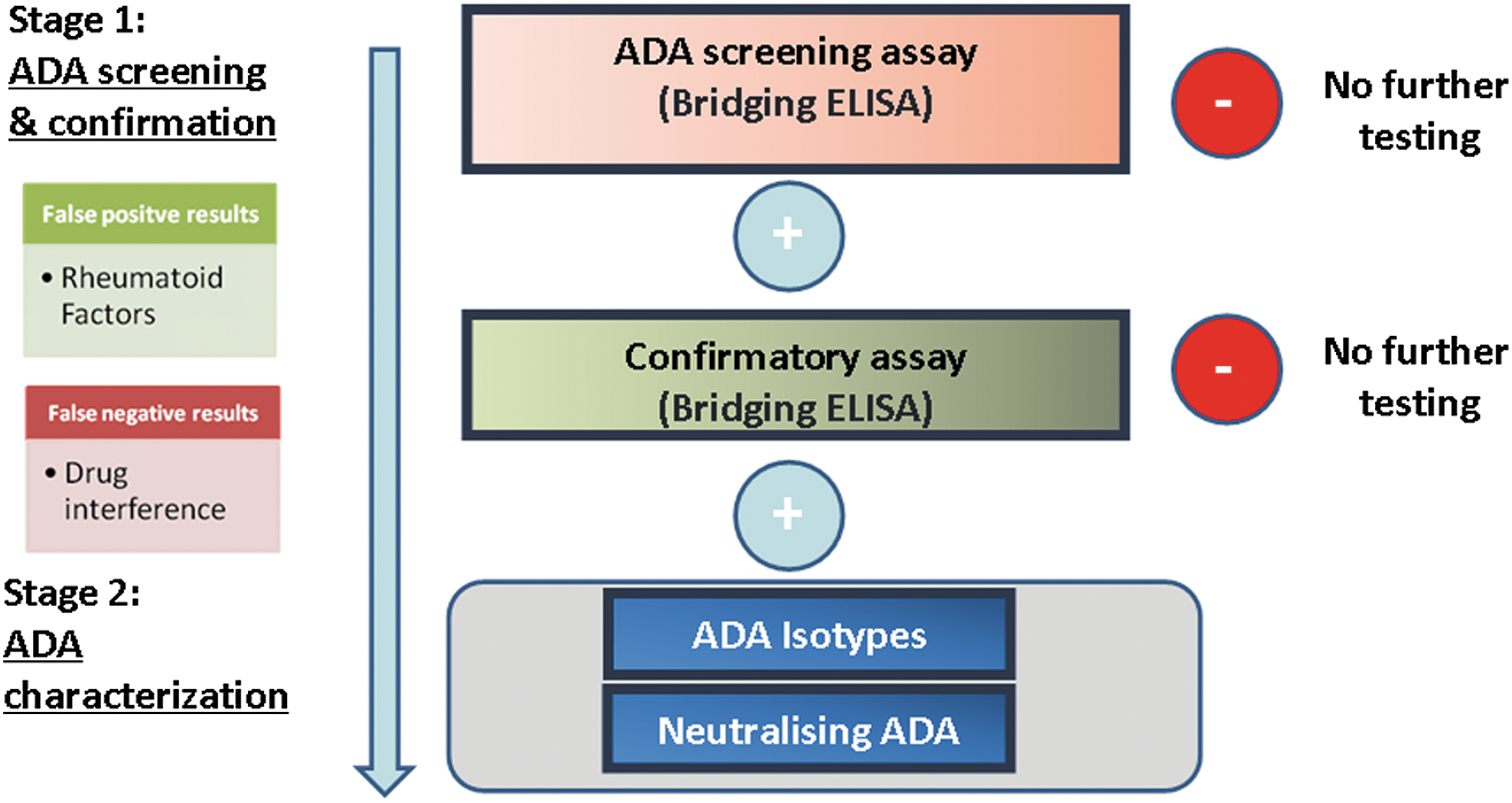
In vitro monitoring of immunogenicity.
The reported incidence of ADA formation, varies widely depending on the assay used (Poter 2001; Bourdage and others 2005). Sensitivity and specificity of the tests may be influenced by several factors, including sample handling and timing of sample collection (Ryff 1997). Serum levels of the drug can interfere with the ADA assay because of the residual presence of the circulating drug and formation of soluble immune complexes. In addition, the presence of free drug itself in the serum sample may interfere with the assay by competing with the secondary labeled antibody. This is true especially for the assay more sensitive to the effects of drug interference, such as the bridging ELISA test, which is the mainly used assay. It is highly recommended that the test be performed relatively distant in time from the infusion, taking into account the half-life of the drug. To reduce the incidence of false-negative results, it is mandatory to take sera before the beginning of therapy and immediately before each readministration. In addition, new immunoassay approaches, such as acid dissociation bridging ELISA, have been proposed to increase the sensitivity of ADA detection (Patton and others 2005). Bridging ELISA has gained in popularity because of its simplicity, but false-positive results may be also found due to cross-binding of IgG by rheumatoid factors or antihinge antibodies.
Using ImmunoCAP platform and other immunoassays, the presence of BA-specific IgE antibodies in a proportion of patients with anaphylaxis has been demonstrated (Georgitis and others 1991; Chung and others 2008; Munoz-Cano and others 2010; Stubenrauch and others 2010; Timm and others 2010). The identification of specific IgE may be difficult because these antibodies are usually quantitatively lower than all other isotypes, but showing the same specificity. As reported above, ADA mainly belongs to the IgG isotype and they can deeply interfere with the detection of the relatively low amounts of IgE. Furthermore, ADA IgE may be bound to the high affinity receptors on mast cells and basophils thus contributing to the low serum concentration challenging the performance of IgE assay in treated patients.
Since an IgE-mediated HR may occur, skin testing (prick and intradermal test) with BA can be performed, even if not routinely. However, up to now, no guideline has been proposed to check all patients who have been intolerant to BA and the exact clinical utility of in vivo tests in routine practice remains unexplored, especially concerning the prognostic values. Although skin tests for BA have not already been standardized, in our experience, patients with reactions to infliximab may represent a clinical model to show the usefulness of skin testing in the management of immunogenicity. Taking into account that the majority of infliximab reactions could be predicted by the appearance of both serum ADA and skin positivity, a possible algorithm must include the detection of these antibodies, at least at the beginning of the treatment, when most of the reactions occur, and in case of retreatment after discontinuation of therapy. This will allow identification of potentially reactive patients and will thus improve the safety profile. In our experience, ADA-positive patients have been submitted to skin testing with BA and if negative, mAb therapy has been performed and a clinical and serological follow-up has been carried out. Patients displaying both in vitro and in vivo positivity have been switched to alternative therapies (Vultaggio and others 2012b). If the therapy is required with no alternative, desensitization procedures may be considered. A proposal of in vivo and in vitro allergological evaluation of patients with IR to BA is reported (Fig. 4). Furthermore, no unexpected adverse reactions to skin testing were recorded in several published cases on biologicals (Brennan and others 2009).
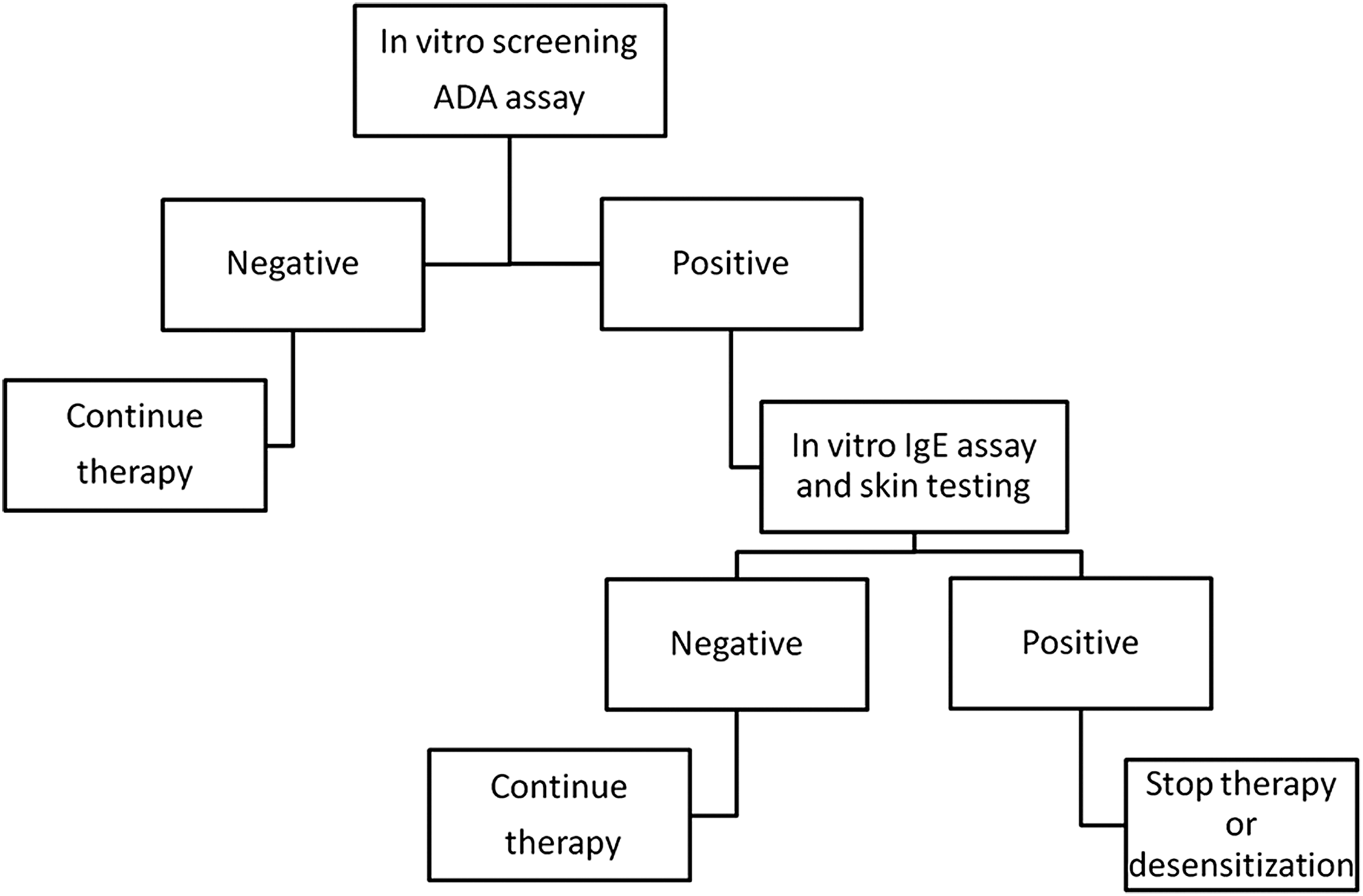
In vitro and in vivo combined evaluation of reactive patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.