
Abstract
Hepatitis C virus (HCV) infection is a major health problem worldwide. Egypt is the country with the highest HCV infection epidemic in the world. Interleukin (IL)-12 is a cytokine that has been shown to have a potent role as an antiviral cytokine. IL-12 is a heterodimer of the polypeptides p35 and p40. IL-12 B, the gene encoding IL-12 p40, is polymorphic, and a functional single-nucleotide polymorphism (SNP) of the 3′-untranslated region at position rs3212227 was associated with apparent resistance to HCV. The genotype distribution of this polymorphism differs by race. This study is sought to identify the genotype distribution of the IL-12 SNP rs3212227 polymorphism in Egyptians and to assess its role in susceptibility to chronic HCV infection alone or in a sex-dependent way. The study included 238 subjects: 100 healthy controls and 138 patients with HCV infection. The IL-12 SNP rs3212227 was genotyped by the polymerase chain reaction–restriction fragment length polymorphism method (PCR-RFLP). Results showed a genotype frequency of 46%, 39%, and 15% for AA, AC, and CC IL-12 genotypes, respectively. No significant result (P=0.5) was shown in the differential distribution of the IL-12 SNP genotypes between controls and patients with HCV infection. Nonetheless, this difference in the IL-12 genotype distribution was significant (0.005) when it was stratified according to sex; moreover, the C allele distribution in men and women differed with a statistically high significance (P=0.0001) in controls versus HCV patients. In conclusion, the IL-12 SNP rs3212227 polymorphism confers a susceptibility to HCV infection in a sex-dependent way in Egyptians.
Introduction
Studies have suggested that the susceptibility to HCV infection is variable, with ∼54%–86% of individuals infected with HCV developing persistent (chronic) infections. Women and individuals infected at a younger age have lower rates of chronicity (Alter and others 1982; Alter and others 1997; Rodger and others 2000).
Host factors have been involved in infectious diseases under the paradigm of the gene–environmental interaction. HCV infection is not an exception, and the discovery of a host factor contributing to HCV pathogenesis will help us to understand the host–virus relationships, and to improve our management of the HCV pandemic.
Cytokines play an important role in the pathogenesis, progression, and treatment outcome of HCV infection (Wan and others 2009). There is evidence that T-cell immune-regulatory cytokines may play a key role in influencing the persistence of HCV infection (Koziel 1999; Huang and others 2004; Kempuraj and others 2004; Gramenzi and others 2005; Petrarca and others 2005). Interleukin (IL)-12 is a key cytokine in promoting antiviral T-helper (Th1) responses and is a heterodimer of p35 and p40 subunits. The gene encoding IL-12 p40 (IL-12B) is polymorphic and located on 5q31–33 (Sieburth and others 1992), and a functional single-nucleotide polymorphism (SNP) (A/C) of the 3′-untranslated region (3′UTR) at position 1188 (rs3212227) has been identified (Huang and others 2000). The variant C allele of the 1188A/C polymorphism has been associated with enhanced IL-12 production (Seegers and others 2002). This polymorphism is associated with the susceptibility to multiple sclerosis and insulin-dependent diabetes mellitus (Morahan and others 2001; Van Veen and others 2001). Hegazy and others (2008) proved that a genetic background of enhanced IL-12 production was associated with apparent resistance to HCV infection. This lends support to a central role for cellular immune responses in protecting from infection. Such studies are still lacking in Egypt, where the frequency of this IL-12B A/C polymorphism is still unidentified, and its impact on susceptibility to persistence of HCV infection is not studied. The aim of this study was to determine the frequency of the IL-12B A/C polymorphism in Egyptians and to assess its impact on susceptibility to persistence of HCV infection in Egyptians independently and with sex.
Materials and Methods
Subjects
This study included 238 subjects; out of them, there were 138 patients with HCV infection obtained from the National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt, and the rest 100 subjects were healthy controls collected from the Faculty of Medicine, Cairo University. Institutional ethics board approval was taken before the study, as well as informed consent was taken from all the participants. The selection criteria for patients were to have a confirmed diagnosis of chronic HCV infection, positive for HCV Ab, not infected with other viral infections (HBV, HIV, EBV, and CMV), no bilharziasis, and no other autoimmune diseases or hematological diseases. The selection criteria for healthy controls are to be negative for HCV Ab, no bilharziasis, and no other autoimmune diseases or other diseases.
Blood sample and DNA isolation
A peripheral venous blood sample of 2 mL was drawn from each individual by standard venopuncture. The blood sample was collected in sterile anticoagulant tubes. Genomic DNA was extracted using the salting-out technique (Miller and others 1988).
Virological testing
The presence or absence of HCV Abs was determined by a third-generation ELISA (Dia Sorin, Torino, Italy).
Genotyping of the IL-12B rs3212227 polymorphisms
The IL-12B genotypes were identified using a polymerase chain reaction (PCR)–restriction fragment length polymorphism analysis (RFLP). The primers for rs3212227 were as follows: forward: 5′-TTCTATCTGATTTGCTTTA-3′ and reverse: 5′-TGAAACATTCCATACATCC-3′ (García-González and others 2005). PCR cycles involved the first denaturation step at 94°C for 4 min followed by 35 cycles with the following cycle profile: denaturation at 94°C for 30 s, annealing temperature 43°C for1 min, and elongation at 72°C for 30 s and a final elongation at 72°C for 5 min. The PCR product [233 base pairs (bp)] was digested by the restriction enzyme Taq-1 (Promega, Southampton, United Kingdom) at 65°C for 120 min. Taq-1 recognizes the sequence. The presence of the C allele produces 2 fragments of 68 and 165 bp, which were separated on an agarose gel (2%) and visualized under UV light.
Statistical analysis
The frequencies of the IL-12B genotypes and alleles were compared between patients with chronic HCV infection and controls by Chi-square test. Two-sample t-tests were used to compare the means for continuous variables and for non-normally distributed continuous variables. The Hardy–Weinberg equilibrium was tested by comparing expected and observed genotype frequencies by w2-test. The distribution of genotypes between the patients and healthy controls was compared by a contingency table analysis. For all tests, a 2-tailed P value of <0.05 was considered significant. The analysis was performed by using statistical software SPSS 17.0 Software.
Results
Demographic and genotyping results
Demographic and clinical data of all subjects included in the study are summarized in Table 1. Genotyping results by the PCR–RFLP showed the existence of the 3 genotypes of the IL-12B rs3212227 polymorphism (AA, AC, and CC), and examples of these results are shown in Fig. 1.
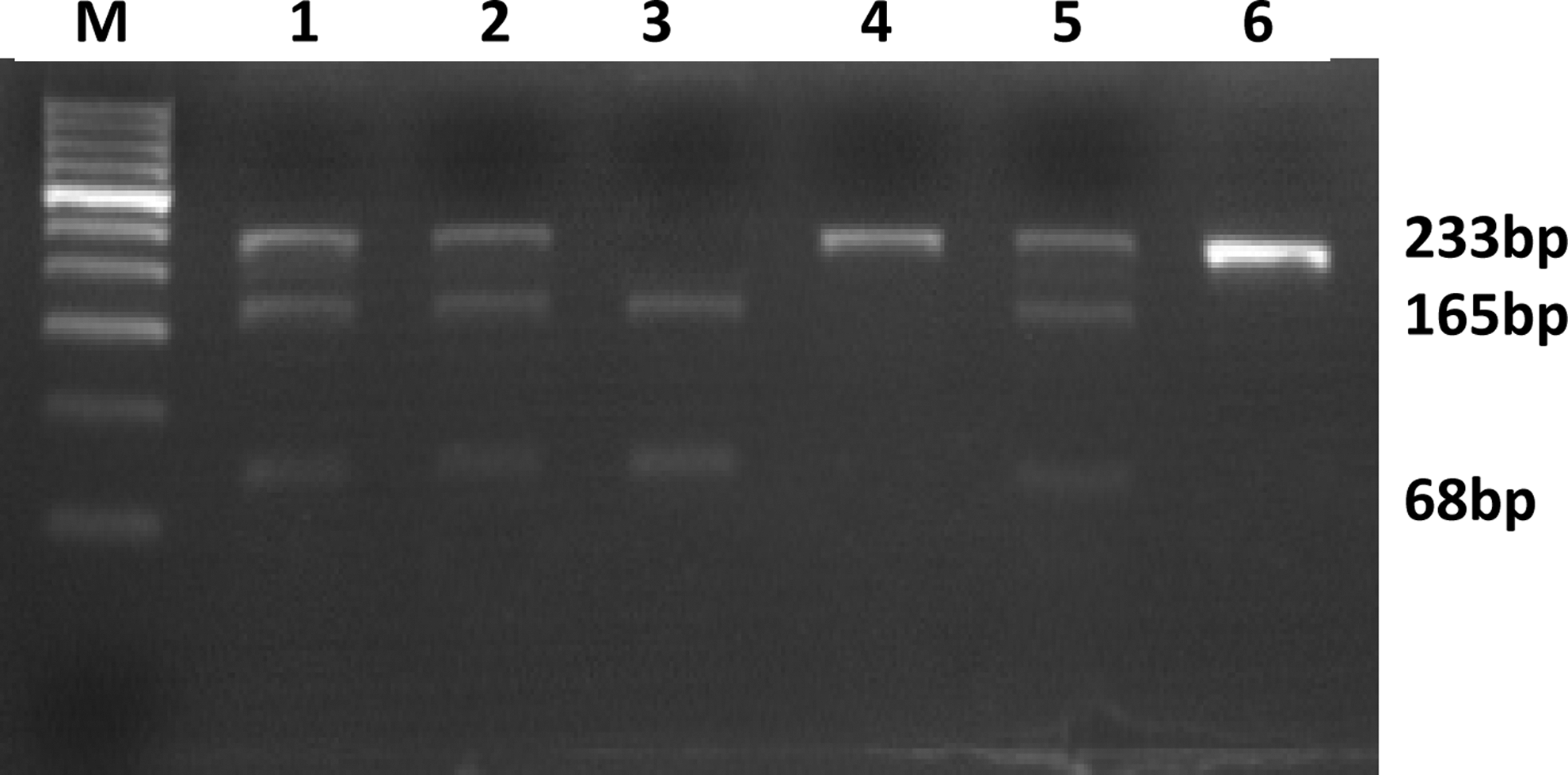
Results of agarose electrophoresis of the restriction fragment length polymorphism analysis reaction. Lanes 1, 2, and 5 represent the interleukin (IL)-12 AC genotype. Lane 3 represents the IL-12 CC genotype. Lanes 4 and 6 represent the IL-12 AA genotype. M is a 50-bp molecular-weight marker.
HCV, hepatitis C virus.
IL-12B SNP (rs3212227) genotype frequencies in healthy subjects versus patients with HCV infection
Results of IL-12B SNP (rs3212227) genotyping of DNA samples from all the subjects are shown in Table 2. The frequency of the IL-12B SNP (rs3212227) in healthy controls were AA: 46%, AC: 39%, and CC:15%.The genotype and allele frequencies in the patient group and healthy controls were in the Hardy–Weinberg equilibrium. As shown in Table 2, there was no statistical difference in the frequency of the IL-12B genotype AA, AC, and CC in healthy subjects versus patients with HCV infection. However, the AA genotype was nonsignificantly more frequent in patients with HCV infection, and the CC genotype frequency was nonsignificantly higher in healthy subjects. There was no statistical difference between the distribution frequency of the A and C alleles between patients with HCV infection and healthy controls, although the A allele was more frequent in patients with HCV infection, and the C allele was more frequent in healthy controls.
N, total number; SNP, single-nucleotide polymorphism; IL, interleukin.
Sex and IL-12B SNP (rs3212227) genotype frequencies in healthy subjects versus patients with HCV infection
Results of comparison the IL-12B SNP rs3212227 genotype and allele distribution frequencies between patients with HCV infection and healthy control according to sex are shown in Table 3. There was a statistically significant difference between the distribution of the IL-12B SNP rs3212227 genotypes in men and women within the healthy controls versus patients with HCV infection (P=0.005). Moreover, a statistical difference was also seen in the distribution of the A and C alleles (P=0.001 and P=0.0001, respectively) in men and women in controls and patients with HCV infection, where the A and C alleles were more frequent in men patients with HCV infection than the control men. On the other hand, the A allele was less frequent in women patients with HCV infection than the women control subjects, and although the C allele is more frequent in control women (62.3%) than men (29.3%), it is highly frequent in HCV men than women (70.7% versus 29.3%) (P=0.001), proving that the C allele is a high risk factor for susceptibility to HCV infection in men, whereas it is a protective factor in women.
Genotype frequency in controls versus HCV according to sex P=0.005.
Discussion
Effective cellular immune responses are critical in the resolution of viral infections, including hepatitis C, and the possible role of immunogenetic factors, such as the cytokine gene polymorphisms, in determining disease outcome via their influence on immune reactivity is important (HILL 1998). IL-12 is a key cytokine for promoting and maintaining antiviral immune responses (Le Cam and Legraverend 1995; Piazzolla and others 2001; Morahan and others 2002). Many chronic infections, including HCV, are associated with impaired IL-12 production (Schlaak and others 1998; Piazzolla and others 2001). An individual's genetically influenced ability to produce IL-12 in response to antigen exposure is likely to be important in influencing the outcome of infection. It was previously reported that an SNP at rs3212227 of the IL-12B gene influences IL-12 secretion (Morahan and others 2001; Seegers and others 2002; Bergholdt and others 2004). A previous study showed that all SNPs genotyped in IL-12B showed a significant variation in the allele frequency by race (Van Dyke and others 2009). The present study is the first one to describe the frequency of the IL-12B SNP rs3212227 polymorphism in Egyptian healthy controls and to compare it with that of chronically infected HCV patients, and moreover, to assess the role of sex in genetic susceptibility to infection with chronic HCV.
Our results showed no statistically significant difference in the distribution of the IL-12B SNP rs3212227 genotypes in controls and patients with HCV infection, suggesting no association of this polymorphism with the susceptibility to chronic infection with HCV. These results are concordant with those of Sunnetha and others (2006) and Muller and others (2004), but differ from them that our results showed a higher frequency of IL-12B genotype AA in patients with HCV infection than in healthy controls, whereas in Sunnetha and others, and Muller and others, it was higher in healthy controls than in patients with HCV infection. Similarly, in our results, the CC genotype was more frequent in the healthy controls than in patients with HCV infection, whereas in Sunnetha and others, and Muller and others, it was higher in patients with chronic HCV infection than in healthy controls. This difference might be due to a different IL-12B genotype frequency in different races and/or in the interference of other immunogenetic factors.
Among the authors who studied the IL-12B SNP rs3212227 genotype distribution in HCV patients with spontaneous recovery versus those with persistent infection, Yin and others reported that homozygosity for the A allele has been associated with HCV persistence in Chinese patients (OR 0.34, P=0.014) (Yin and others 2004). This was also found in a second study from the United Kingdom, where 66% of the persistently infected people were A/A homozygous compared to 50% of those with spontaneous recovery (Houldsworth and others 2005). These results were partially consistent with our results, as we reported a higher frequency of A/A homozygous individuals in patients with chronic HCV infection than healthy controls, but it was nonsignificant. Further studies on our patients are needed to explore the difference in the IL-12B genotype distribution in self-limited versus patients with chronic HCV infection to assess the association of the IL-12B AA genotype with persistent infection with HCV.
Susceptibility to viral infections differs by sex; women have been found to have an increased immune response, which renders them less reliable to acquire viral infections (Klein 2000). Recently, Hannah and others (2008) showed that sex hormones play a critical role in sex variation in the immune response to viral infections. To study the role of sex on the genetic susceptibility to chronic HCV infection, the SNP genotype distribution was stratified according to sex and compared in controls and patients with chronic HCV infection. A statistically significant difference in the genotype and allele distribution was recorded, implying the role of sex in genetic susceptibility to infection with chronic HCV. As far to our knowledge, this is the first data proving the correlation between sex and genetic susceptibility to chronic HCV infection in our Egyptian population. According to our results, men homozygous for the A and C alleles are more susceptible for infection with chronic HCV than women; moreover, men homozygous for the C allele are at a higher risk than men homozygous for the A allele (P=0.004 versus P=0.045). Similarly, women homozygous for the C allele are less susceptible to infection with chronic HCV than men. This agrees with Hegazy and others in the fact that the homozygous CC genotype confers resistance to infection with HCV, but differs from Hegazy and others that it applies on women only. Although these results need to be confirmed on a larger number of samples and in other polymorphisms, they highlight the concept that the sex-related immunogenetic variation may have a stronger impact on the natural course of HCV infection and must be further studied.
In conclusion, our results suggest that the IL-12B SNP rs3212227 alleles impact the setting of HCV infection by conferring a sex-dependent susceptibility to infection. As the IL-12B gene is not located on the X-chromosome, this is considered an interesting result. Due to accumulating data on the genetic polymorphism in HCV infection, the patient's sex needs to be taken into account when future individual risk profiles for HCV infection are generated.
Author Disclosure Statement
No competing financial interests exist.