
Abstract
Interferon beta-1a (IFNβ-1a) 30 μg weekly by intramuscular (IM) injection is used to treat relapsing forms of multiple sclerosis. We assessed if it can be given safely by inhalation. Twenty-one healthy volunteers inhaled IFNβ-1a 300 μg, formulated for deep delivery to the lungs, in a randomized, parallel-group, repeat-dose trial. Comparators were room air and placebo. The primary outcome measure was carbon monoxide transfer factor corrected for hemoglobin (TLCOc), which measures the CO transfer from inspired gas to pulmonary capillary blood. After 3 and 4 once-weekly doses, IFNβ-1a significantly reduced TLCOc compared with room air: after the third dose, mean standard deviation (SD) change in percent predicted TLCOc was−10.9 (2.8), and after the fourth dose was−12.1 (2.7). After 2, 3, and 4 doses, IFNβ-1a significantly reduced TLCOc compared with placebo: after the second dose, mean (SD) change in percent predicted TLCOc was−8.8 (5.5), after the third dose was−10.9 (2.8), and after the fourth dose was−12.1 (2.7). Circulating IFNβ-1a concentrations were about one-third those of the intramuscular dose regimen. Tolerability of IFNβ-1a and the comparators was equally good. In conclusion, IFNβ-1a reduced TLCOc, whereas placebo and room air did not. A dose of IFNβ-1a 300 μg by inhalation may not be safe for general use.
Introduction
I
The lung has a large surface area (100 m2) for the potential absorption of drugs. For optimum deep lung delivery, aerosol particles must be 1–2 μm in diameter (Patton and Byron 2007). Smaller particles are exhaled, and larger ones are deposited in the upper airways where absorption is poor. In the past, inhaled drugs were developed mainly to target the lung, but several successful attempts have been made to deliver inhaled drugs to the systemic circulation. For example, insulin has been successfully delivered through the lungs to patients with diabetes (Cappelleri and others 2002; Ceglia and others 2006; Santos Cavaiola and Edelman 2014). A rapidly acting inhaled insulin has recently been approved for treatment of patients with diabetes (FDA 2014).
IFN has been given by inhalation to patients with various lung diseases. IFN-α (Kinnula and others 1989; Ruotsalainen and others 1999), IFN-γ (Halme and others 1995), and IFN-β1a (Halme and others 1994) have been given to patients with lung cancer. IFN-α has also been given to patients with tuberculosis (Giosue and others 1998), and IFN-γ has also been given to patients with idiopathic pulmonary fibrosis (Diaz and others 2012). Overall, tolerability was good in those studies. The most common adverse effects were flu-like symptoms, but some patients had dyspnea and a fall in peak expiratory flow rate (PEFR). A novel application of inhaled IFN-β is currently in clinical development for preventing or treating symptoms of respiratory tract viral infection in patients with asthma (Djukanovic and others 2014; Synairgen 2014).
IFN-α (Giosue and others 1996) and IFN-γ (Martin and others 1993) have been given by inhalation to healthy volunteers.
In the nonhuman primate, IFNβ-1a 60 μg was administered by pulmonary inhalation 1, 3, or 7 times/week for 4 weeks. The results suggested that pulmonary administration might be a safe and feasible alternative to IM administration for the systemic delivery of IFNβ-1a (Martin and others 2002).
The rationale for our study was that the available data suggested that inhaled IFN was systemically bioavailable, but there was uncertainty about its safety and tolerability. In particular, prior reports of dyspnea and reduced PEFR mandated further investigation. We were particularly concerned that inhaled IFN might impair pulmonary gas transfer. We did this study in healthy volunteers to assess the local (pulmonary) safety and tolerability of inhaled IFNβ-1a, formulated to allow deep delivery to the lungs. Because the placebo (excipient) had not been tested for effects on transfer factor corrected for hemoglobin (TLCOc), we included an air treatment as an inactive control for the excipient.
The primary outcome measure was carbon monoxide TLCOc, because in a preliminary study we had noted a trend for TLCOc to fall after inhalation of IFNβ-1a by healthy volunteers. TLCO has been used to assess drug-induced changes in lung function both when the lung is the target organ, as with alpha1-antitrypsin (Schwaiblmair and others 1997), and when it is not, as with bleomycin (Villani and others 1995) and amiodarone (Ulrik and others 1992). TLCO has the unique advantage in that it measures specifically the efficacy of pulmonary gas transfer, independent of the influence of physiological compensatory mechanisms, which impair the sensitivity of measures, such as arterial blood gases or pulse oximetry. As secondary measures, we did standard spirometric tests, pulse oximetry to monitor oxygen saturation of hemoglobin, chest x-ray to detect inflammatory edema of the lung, and physical examination of the chest to detect wheeze, crackles, and consolidation.
Unlike previous studies, the present one was designed specifically to measure pulmonary adverse effects of inhaled IFN. We used healthy volunteers to avoid confounding of the results by deterioration in the condition of patients with respiratory, neurological, or other diseases.
Materials and Methods
The study was done at Hammersmith Medicines Research, London (clinical trial registry number: NCT 01863069) in accordance with the ICH Guideline for Good Clinical Practice, and was approved by the local research ethics committee. All subjects gave fully informed, written consent.
Subjects
Twenty-one subjects (12 men and 9 women) aged 18–44 (mean 25) years were enrolled. All subjects were deemed healthy on the basis of medical history and examination, chest x-ray, 12-lead electrocardiogram (ECG), body mass index (BMI), laboratory tests, including HIV and hepatitis B and C serology, and tests for drugs of abuse. At screening, subjects had values of at least 80% predicted normal for forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), total lung capacity (TLC), and carbon monoxide TLCOc. Subjects were nonsmokers or had not smoked for at least 6 months. They used no prescription medicines in the 4 weeks before the trial, and no over-the-counter medicines (with the exception of acetaminophen) in the 48 h before the trial. Female subjects were not pregnant or lactating, and used a reliable method of contraception.
Design and methods
The study was placebo-controlled, randomized, parallel-group and repeat-dose in design. Twenty-one subjects were randomized equally to 1 of 3 treatments: IFNβ-1a 300 μg, placebo (sucrose/leucine excipient), and room air as a control. Subjects were scheduled to receive 4 doses of the treatment, at weekly intervals. IFNβ-1a 300 μg was selected because a single 300 μg dose had shown acceptable pulmonary safety in an earlier trial and had yielded plasma concentrations about ¼ of those after a 60 μg IM dose.
Drug formulation and delivery
IFNβ-1a 300 μg was formulated with 2.7 mg leucine/sucrose excipient. Placebo was 3.0 mg powder containing leucine and sucrose. Treatments were supplied by Biogen (02142; Cambridge, MA).
All treatments were delivered by a handheld, dry powder, pulmonary delivery system (Nektar Therapeutics, San Francisco, CA) (Patton 2000) that uses compressed air, released at sonic velocity, to convert the active or placebo powder into an aerosol cloud in a 200-mL delivery chamber. The cloud is then inhaled, without the need to coordinate aerosol generation with inhalation. The delivery chamber was covered so that the aerosol cloud could not be seen, thus maintaining the blind with respect to the room air control. The median aerodynamic diameter of the aerosol particles was about 3 μm, which is an appropriate size for deep lung delivery.
Procedures
Subjects were resident from the day before until 48 h after each dose. They took 1 g of acetaminophen 6-h from just before until 24 h after each dose, to mitigate the distressing flu-like symptoms that interferon treatment often causes.
TLCOc was measured at screening, day 1 (the day before the first dose), at 48 (±4) and 144 (±24) h after each dose, and at about 2 and 4 weeks after the last dose. Additional measurements were done if necessary, to follow any changes to resolution. Spirometry was done before and at 0.5, 2, 6, 12, and 24 h after each dose.
Oxygen saturation was measured before, at 10 and 30 min, and 1, 2, 4, 6, 9, 12, 15, 18, 21, 24, and 48 h after each dose.
Medical examination, standard hematological and biochemical blood tests, and urinalysis, were done frequently during the study.
A chest x-ray was done 144 h after the last dose.
Plasma samples for assay of IFN were obtained just before the first and the final (fourth) doses, at 10, 30, and 60 min afterward, and then at 2, 4, 6, 9, 12, 15, 18, 21, 24, 30, 36, 48, 72, 96, and 144 h after the first and the final doses.
Adverse events were elicited by a nonleading question (How do you feel?) at the time of every observation. Evidence of breathlessness was sought specifically, using a modified MRC 5-point rating scale for dyspnea. The subjects completed the rating before each dose, then at 30 min, 2, 6, 12, 24, 48, and 144 h after dosing. The scale ran from zero (dyspnea only upon strenuous exercise) to 4 (dyspnea causing inability to go outside the home); a 1-point change was taken to be clinically meaningful.
Spirometry
FVC, FEV1, peak expiratory flow (PEF), and mid expiratory flow (MEF 25%–75%) were measured using a SuperSpiro spirometer (Micro Medical).
TLC and TLCOc
TLC was measured by the helium dilution technique, and TLCO was measured by the single breath-hold method, using the MasterScreen Pulmonary Function Testing system (Jaeger). TLCO was measured, and corrected for hemoglobin, according to the American Thoracic Society ATS guidelines (ATS 1995). The mean of 2 readings that met technical and reproducibility criteria, as defined by the ATS, was taken as the result at each time point.
Oxygen saturation
Oxygen saturation was measured by pulse oximetry using the SpaceLabs Patient Care Monitoring System.
Statistical analysis of TLCOc
TLCOc was measured on 2 occasions before the start of the study: at screening and on day 1. The mean of those 2 values was taken as the baseline. TLCOc was measured again at 48 and 144 h after each dose, and the mean of those 2 values was taken as the postdose result. All values were expressed as percent of the subject's predicted value. Any subject who had a reduction of >15 in percent predicted TLCOc postdose compared with baseline (percent predicted postdose−percent predicted baseline) was not dosed further, but continued with the scheduled TLCOc measurements; their data, including TLCOc measurements taken after dosing had been discontinued, were included in the analysis. Data from subjects who withdrew for reasons unrelated to the study were included up to the time that they withdrew.
After each dose, the mean change in percent predicted TLCOc (percent predicted postdose−percent predicted baseline) and mean absolute change in TLCOc were compared between air and IFNβ-1a, and placebo and IFNβ-1a. That was done using the Wilcoxon rank-sum (nonparametric) test with 95% confidence intervals. No sample size calculation was done; the choice of 7 subjects per treatment was determined by feasibility and affordability.
Results
Baseline characteristics
All subjects met strict entry criteria. The 3 treatment groups, each with 7 subjects, had the same male:female ratio, subjects of similar age, and similar TLCOc absolute, and percent predicted TLCOc results at baseline (Table 1). Percentage change in TLCOc from screening to day 1 is shown in Figure 1, and baseline characteristics are summarized in Table 1.

Mean (treatment group) change in percent predicted transfer factor corrected for hemoglobin (TLCOc) from screening to Day 1 for: IFNβ-1a, air, and excipient. Each symbol represents data from a single subject. n = 7 per treatment. Excipient = triangles, air = squares, interferon = diamonds.
n = 7 per treatment group.
IFNβ-1a, interferon beta-1a; TLCOc, transfer factor corrected for hemoglobin.
Local safety and tolerability
Sixteen subjects completed the 4 scheduled treatments. Dosing was stopped in 3 subjects, and 2 subjects were withdrawn for reasons unrelated to the study. Mean change in percent predicted TLCOc from baseline to postdose (the mean of 48 and 144 h values) is shown in Figure 2 and Table 2. The mean percent predicted TLCOc at screening, day 1 and 48 and 144 h after each dose is shown in Figure 3. The mean difference in actual (as opposed to percent predicted) TLCOc between air and IFNβ-1a, and placebo and IFNβ-1a, is shown in Table 3. The mean difference in actual TLCOc between air and IFNβ-1a was statistically significant from the third dose onward; the mean difference in actual TLCOc between excipient and IFNβ-1a was statistically significant from the second dose onward.

Mean change (95% CI) from baseline to postdose (mean of 48 and 144 h) in percent predicted TLCOc. Data points are offset for clarity. n = 7 per treatment group. CI, confidence intervals.
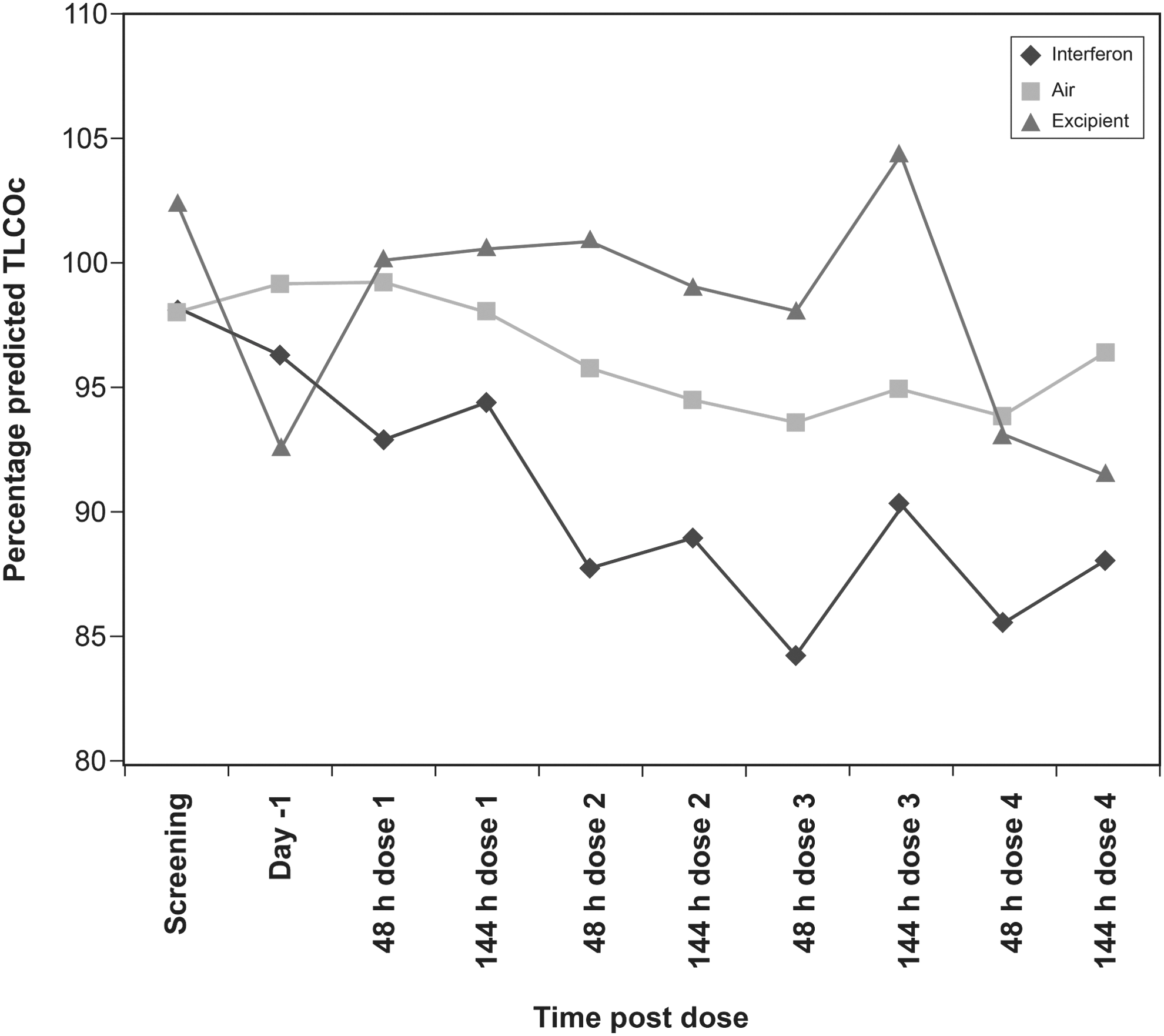
Mean percent predicted TLCOc at screening, day 1 and 48 and 144 h after each dose n = 7 (interferon and excipient dose 4, n = 6). Excipient = triangles, air = squares, interferon = diamonds.
n = 7 per treatment; * n = 6.
SD, standard deviation.
n = 7 per treatment, except as shown in Table 2.
CI, confidence intervals.
Dosing was stopped for safety reasons in 3 subjects, each of whom had received a different treatment, as follows: (1) 1 subject stopped treatment after 2 doses of IFNβ-1a, because of a decrease in percent predicted TLCOc of−8 after dose 1, and−16 after dose 2 (recovering to−14 at the time point scheduled for dose 3, and−10 at the time point scheduled for dose 4). (2) 1 subject stopped treatment after 2 doses of air because of a change in percent predicted TLCOc of−6 after dose 1, and−16 after dose 2 (then−3 at the time scheduled for dose 3, and−2 at the time scheduled for dose 4). (3) 1 subject stopped treatment after 1 dose of placebo (excipient) owing to a persistent cough, without a reduction in TLCOc.
In addition, 1 subject withdrew from the study after 3 doses of placebo (excipient), and another after 3 doses of interferon, for reasons unrelated to the study.
All results of the dyspnea scale assessments were zero, at all times after all treatments.
There was no change from baseline in the results of spirometry, oxygen saturation monitoring, medical examination, or chest x-ray, after any of the treatments.
Pharmacokinetic data
Pharmacokinetic data were not released by the sponsor, but circulating concentrations of IFNβ-1a were reported to be about one-third those achieved by administration of a 30 μg dose by the IM route (Biogen Idec, personal communication).
Adverse events
Adverse events are listed in Table 4. Events related to the respiratory system were minor, and their frequency, nature, and severity did not differ importantly among treatments. Although a persistent cough led to the withdrawal of 1 subject from treatment (with room air), that cough was not particularly troublesome and would not have caused any concern if the subject had not been in a clinical trial. The incidence of systemic adverse reactions after IFNβ-1a was similar to that after the control treatments.
n = 7 per treatment.
Treatment stopped in 1 subject, after 2 doses.
Treatment stopped after 2 doses.
Discussion
We found that inhaled IFNβ-1a, formulated for deep delivery to the lungs, reduced TLCOc, but there was no adverse change in any of the other safety variables, which included a comprehensive range of tests of pulmonary function. General tolerability of inhaled IFNβ-1a was good: in particular, there was no excess of the systemic symptoms that are typically associated with therapeutic doses of interferon (Table 4). That outcome is consistent with the observed plasma concentrations of IFNβ-1a, which were substantially lower than those associated with therapeutic IM doses. However, it is also possible that any systemic symptoms that might have occurred were mitigated by the prophylactic acetaminophen that the subjects received.
TLCO is a measure of CO transfer from inspired gas to pulmonary capillary blood. Although gas transfer can be influenced by changes in ventilation–perfusion relationships, capillary volume, hemoglobin concentration, and reaction rates between CO and hemoglobin, all those factors would have been stable in our healthy subjects. So, the fall in transfer factor must indicate impaired transfer of gas from the surface of alveolar epithelium to the pulmonary capillary blood. In the absence of any more plausible explanation, it is reasonable to assume that the decrease in TLCOc was due to mild alveolar edema induced by IFN beta-1a, as further discussed below. Our results, therefore, suggest that IFN might not be safe when given by inhalation into the lung. Given that our inhaled dose of 300 μg yielded plasma concentrations of IFN that were about 1/3 of those associated with the conventional 30 μg IM dose, we cannot conclude that the inhaled route is a safe alternative to IM administration. However, if IFN should prove to be effective at plasma concentrations much lower than those seen with the 30 μg IM dose, as proposed by Brod (2010), it might be appropriate to investigate the pulmonary safety of correspondingly lower doses of inhaled IFN.
TLCO shows considerable within-subject variability, both intra- and intersession (ATS 1995; Robson and Innes 2001). Guidelines recommend that 2 technically acceptable tests that meet reproducibility criteria (ie, within ±10% of the average TLCO) be reported as the result in any given session (ATS 1995). (Robson and Innes 2001) found the coefficient of repeatability to be ±1.60 mmol/min/kPa in healthy subjects in whom TLCO was measured twice, 1 week apart. Our results from screening to day 1 (Fig. 1) show variability similar to that. However, more subjects showed a reduction in TLCOc from screening to day 1 (13 subjects) than an increase (8 subjects). That phenomenon might reflect regression to the mean, as subjects had to have a TLCOc of at least 80% predicted to be eligible for the study, and 9 subjects with values less than 80% predicted were excluded after their first TLCOc measurement. Thus, subject selection was biased toward those who had (by chance) a higher than usual value at first screening. Subjects with low TLCOc, who were more likely to show an increase in TLCOc on second measurement, had already been excluded.
TLCO measurement may vary during the day, perhaps because of diurnal changes in hemoglobin (ATS 1995). Although we aimed to measure TLCOc at the same time of day in each subject, that was not always possible. That might have increased the variability of the test, but it is unlikely to have affected the overall results, as the volunteers were studied in 2 large groups, with equal treatment allocation. Any effect of time of day would have been distributed equally among all treatments.
The magnitude of the fall in TLCOc that is clinically relevant has not been defined. In clinical practice, pulmonologists tend to follow trends over time to monitor lung disease progression. We had to set a threshold for change in TLCOc that would oblige us to stop dosing a subject, given that the safety of the healthy volunteers was paramount. Informal conversations with pulmonologists suggested that most would regard a decrease in TLCOc of up to 15% as being of doubtful significance, whereas a decrease >15% might be of clinical significance. We chose a change of >15% as the stopping criterion, because we considered that it would ensure the safety of the subject without being so low that many subjects would be withdrawn because of random falls in TLCOc.
We took the mean of measurements on 2 separate days as the baseline, and the mean of 2 postdose values (48 and 144 h), to determine the stopping criterion in individual subjects. It is possible that taking the mean of the 2 postdose values underestimated the true maximum effect on TLCOc, as Figure 3 shows that the mean 48 h measurements tended to show a greater decrease from baseline than did the 144 h mean, after both the third and fourth doses of interferon. Thus, some recovery of the effect might have occurred by the 144 h time point. However, given the small sample size, that apparent effect could have occurred by chance alone.
Although we withdrew 1 subject on each treatment, that does not undermine our conclusions about the effect of IFNβ-1a on TLCOc. We withdrew 1 subject because of persistent cough, without a reduction in TLCOc. We withdrew 2 subjects because of a fall in TLCOc: 1 subject after 2 doses of interferon, the other after 2 doses of room air. In the IFNβ-1a-treated subject, TLCOc showed slow but steady improvement during the 2 weeks after the last dose, which is suggestive of a treatment effect that reversed progressively with time. In the air-treated subject, TLCOc measured soon after the last dose showed recovery to near baseline, suggesting that the low measurement after the second dose of air was random rather than treatment-related. The outcome supports our choice of a >15% change in TLCOc as a stopping criterion, given that we withdrew 1 subject whom it might not have been safe to continue dosing, but withdrew only 1 subject because of a random change.
The mechanism of the fall in TLCOc is uncertain. IFNβ-1a in human albumin and phosphate buffered saline administered intrabronchially to monkeys caused mild alveolitis, mainly near the instillation site (Martin and others 2002). Similar changes were also reported in control animals, and were considered by the authors to be due to instillation of a foreign protein or to minor injury caused by the instillation process. One animal in the highest dose group had eosinophilic alveolitis, perhaps due to a type 1 hypersensitivity response to interferon or human albumin. In toxicology studies of the formulation we studied here, monkeys showed mild, multifocal, mixed inflammatory cell infiltrates in the alveolar septae, and perivascular mononuclear cell infiltrates. Those effects were seen in control animals, but to a lesser extent (Biogen Idec, personal communication). So, preclinical studies suggest that our findings in healthy volunteers might have been due to an inflammatory process at the alveolar surface, which would impair gas transfer and so reduce TLCOc.
In a multicenter, placebo-controlled trial in patients with worsening of asthma symptoms caused by viral infections, a dose regimen of 6 million units of IFN-β inhaled daily for 14 days enhanced morning PEF recovery and was well tolerated (Djukanovic and others 2014; Synairgen 2014) A dose of 6 million units is equivalent to 30 μg of IFN-β, and, therefore, was only 10% of our 300 μg dose. In a substantial online data supplement to the main publication, the authors state that diffusing capacity of the lung for carbon monoxide (DLCO) was measured on day 1 and 17 and no results were given, but presumably DLCO was included in the authors' general statement that there were no adverse changes in any of the respiratory function tests. In the supplement, the authors also summarize the outcome of 2 preliminary, dose-escalating trials. The first trial was in 36 patients with atopic sensitization to common air allergens (as shown by skin-prick tests). Patients received IFN- β in single doses of 0.48 million, 2.4 million, and 4.8 million IU, and there were no changes in lung function tests, including DLCO; however, no actual data were given. In the second trial, patients (number not specified) with controlled asthma received 14 days' treatment with IFN- β, once daily, in escalating doses of 0.4 million, 1.5 million, and 6 million IU; safety and general tolerability were satisfactory and supported further studies, but DLCO was not measured.
Conclusions
IFNβ-1a, formulated for deep lung delivery and given by inhalation, reduced TLCOc, whereas placebo (sucrose/leucine excipient) did not. Therefore, caution is needed when interferon β-1a is given by inhalation. TLCO is sensitive and reproducible enough to detect adverse effects of drugs at the alveolar–capillary interface, in healthy volunteers.
Footnotes
Acknowledgment
The authors thank Biogen Idec for sponsoring this study. They played no part in the preparation of this article.
Author Disclosure Statement
Biogen Idec paid Hammersmith Medicines Research Ltd (HMR) to do this study. All the authors were employees of HMR.