
Abstract
Pegylated interferon and ribavirin plus simeprevir therapy (simeprevir-based triple therapy) has been recently introduced, providing excellent results for nontransplant patients with hepatitis C virus (HCV) infection. However, there are limited data available on its effect on liver transplant recipients. In the present study, we evaluated the efficacy and tolerability of simeprevir-based triple therapy in liver transplant recipients. We treated 9 liver transplant recipients for genotype 1b HCV reinfection with simeprevir-based triple therapy. The efficacy and adverse effects were evaluated until 24 weeks after therapy. All recipients continued immunosuppressive therapy at the same dose as that before therapy induction. Seven of the 9 recipients (77.8%) achieved sustained virological response at 24 weeks. Two recipients (22.2%) experienced viral breakthrough (BT) at 12 and 16 weeks; NS3 HCV mutations conferring resistance to simeprevir were detected in both these patients after BT. Anemia was the most common adverse effect, requiring ribavirin dose reduction and blood transfusion. However, all recipients, except those with BT, completed the 24-week therapy. No recipient experienced cellular rejection during therapy. In conclusion, simeprevir-based triple therapy exhibited high efficacy and tolerability in liver transplant recipients with genotype 1b HCV reinfection.
Introduction
E
Until recently, the standard treatment for HCV reinfection in LT recipients included pegylated interferon and ribavirin (PEGIFN/R) therapy, similar to that for non-LT HCV chronic hepatitis patients. However, sustained virological response (SVR) was achieved in only approximately 30% of refractory genotype 1 (G1) LT recipients (Picciotto and others 2007; Berenguer 2008; Roche and others 2008; Veldt and others 2008). Moreover, it has been reported that achieving SVR improves the prognosis of recipients with HCV reinfection (Picciotto and others 2007; Veldt and others 2008; Kawaoka and others 2014).
PEGIFN/R in combination with NS3/4A protease inhibitor has been recently used, providing excellent results for non-LT HCV G1 patients. Telaprevir and boceprevir, the first-generation inhibitors of linear NS3/4A HCV protease, in combination with PEGIFN/R achieved SVR in 50%–60% of non-LT patients with G1 chronic HCV infection (Bacon and others 2011; Jacobson and others 2011; Poordad and others 2011; Zeuzem and others 2011). The efficacy of telaprevir- and boceprevir-based triple therapy has already been reported in LT recipients (Pungpapong and others 2013; Coilly and others 2014; Ikegami and others 2014).
However, it has been difficult to administer telaprevir- and boceprevir-based triple therapy due to severe adverse effects, such as anemia and a requirement of frequent monitoring of drug–drug interactions with calcineurin inhibitors (CNIs) in LT recipients (Pungpapong and others 2013; Coilly and others 2014; Ikegami and others 2014).
Following the introduction of first-generation NS3/4A protease inhibitors, simeprevir—a second-generation inhibitor of macrocyclic HCV NS3/4A protease—has been recently approved for use in combination with PEGIFN/R for patients with G1 chronic HCV infection. Simeprevir-based triple therapy has good effects in non-LT HCV G1 patients (Jacobson and others 2014; Manns and others 2014). Moreover, simeprevir-based triple therapy has revealed lesser adverse effects, including less severe ones and a lower discontinuation rate compared with telaprevir-based triple therapy (Reddy and others 2015). Hence, simeprevir-based triple therapy is expected to improve the therapeutic effects in LT recipients with HCV reinfection.
However, to the best of our knowledge, to date, there has been only one 12-week pilot study regarding the efficacy of simeprevir-based triple therapy for LT recipients. In the present study, we examined the therapeutic and adverse effects of simeprevir-based triple therapy in HCV reinfected LT recipients.
Material and Methods
Study design and recipients
This prospective study was approved by the Ethics Committee of the Nagasaki University Hospital (ID #1322021). The study subjects included 9 recipients who had undergone living donor LT (LDLT) with splenectomy because of end-stage liver disease related to HCV chronic infection in the Nagasaki University Hospital and who were persistently reinfected with HCV after LDLT. All recipients who required antiviral therapy against genotype 1b HCV from December 2013 to February 2014 received pegylated interferon α-2b (Pegintron; MSD) and oral ribavirin (Rebetol; MSD) in combination with oral simeprevir (SOVRIAD; Janssen) (PEGIFN/R plus simeprevir therapy). The requirement for antiviral therapy was evaluated by blood examination and percutaneous liver biopsy.
Eight recipients suffered from chronic hepatitis and had fibrosis progression due to HCV. One recipient was diagnosed with fibrosing cholestatic hepatitis (FCH) due to HCV, and another recipient was treated with telaprevir-based triple therapy 1 year before PEGIFN/R plus simeprevir therapy.
Antiviral therapy regimen
All recipients received PEGIFN/R plus simeprevir therapy. The initial dose of pegylated interferon α-2b was determined according to the body weight (pegylated interferon α-2b; 1.5 μg/kg, weekly). The initial ribavirin dose (200–800 mg/day) was selected at the attending physicians' discretion, based on weight, hemoglobin levels, and the general condition of recipients. The dose of pegylated interferon α-2b and ribavirin can be reduced according to the degree of cytopenia and tolerability during treatment. The daily dose of simeprevir was 100 mg consistently for all recipients. Furthermore, the duration of pegylated interferon α-2b and ribavirin therapy was 24 weeks and that of simeprevir was 12 weeks.
If during therapy, HCV RNA levels changed from being undetectable to detectable, it was defined as viral breakthrough (BT), and treatment was terminated. During hospitalization, all recipients received PEGIFN/R plus simeprevir therapy to evaluate early adverse effects.
The HCV genotype was determined by polymerase chain reaction (PCR). IL28B single-nucleotide polymorphisms (rs8099917) for LDLT donors and recipients were detected by pyrosequencing analysis. (Kamo and others 2015). Routine blood tests and hematochemical analysis were performed every week during treatment in the hospital and outpatient clinic. Blood transfusion was provided to patients with a poor physical condition with hemoglobin levels dropping below 8.0 g/dL despite ribavirin dose reduction. Tacrolimus (Tac) (Prograf; Astellas) alone was administered to 3 recipients, Tac with mycophenolate mofetil (MMF) (CellCept; Tyugai) to 3; cyclosporine (CyA) (Neoral; Novartis) alone to 1 patient, CyA with MMF to 1, and MMF alone to 1 as immunosuppressive therapy. All recipients continued the previous immunosuppressive therapy at the same dose as before the PEGIFN/R plus simeprevir induction.
Trough levels of Tac and CyA were analyzed at 1, 4, 12, and 24 weeks and 12 weeks posttreatment. If necessary, the dosage was changed according to Tac and CyA trough levels. To confirm that hepatic dysfunction was due to HCV reinfection and to evaluate the liver histology, percutaneous liver biopsy with ultrasonography was performed before treatment. The degree of fibrosis (staging) were classified as follows: F1, periportal expansion; F2, portoportal septa; F3, portocentral linkage or bridging fibrosis. The degree of necroinflammatory activity (grading) was classified as follows: A1, mild; A2, moderate; A3, severe (Desmet and others 1994).
Efficacy assessment
To assess the efficacy of PEGIFN/R plus simeprevir, the plasma HCV viral load was monitored using the COBAS TaqMan Real-Time PCR assay (Roche Diagnostics) at baseline; day 1; weeks 1, 2, 4, 8, 12, 16, 20, and 24; and posttreatment weeks 4, 8, 12, and 24. A rapid virological response (RVR) was defined as undetectable HCV RNA at 4 weeks; a complete early virological response (cEVR) was defined as undetectable HCV RNA at 12 weeks, and an end-of-treatment response (ETR) was defined as undetectable HCV RNA at the end of treatment. Furthermore, SVR24 was defined as undetectable HCV RNA 24 weeks after the end of treatment. Viral BT was defined as detectable HCV after achieving undetectable levels of HCV RNA during treatment.
Virological resistance mutations
The mutations conferring resistance to NS3/4A protease inhibitors in the NS3 region (V36A/M, T54A, V55A, Q80R/K, R155K/T/Q, A156S, D168A/V/T/H, and V170A) (Halfon and Locarnini 2011; Suzuki and others 2012; Lenz and others 2015) were analyzed at baseline for all recipients and 2 months after treatment termination for recipients who had experienced BT, evidenced by PCR and direct sequencing. HCV RNA was extracted from sera using the QIAamp MinElute Virus Spin Kit (Qiagen), and reverse transcription was performed by a random primer of SuperScript III (Invitrogen). The HCV NS3 region was amplified by nested PCR using specific primers (Supplementary Table S1; Supplementary Data are available online at
Results
Characteristics of the study population
Recipient characteristics are presented in Table 1. There were 3 males (33.3%) and 6 females (66.7%), with a mean age of 60.1 years (42–73 years). Six recipients had the major allele of IL28B (rs8099917) (TT), and 3 had the minor allele (TG). Eight donor IL28B alleles were examined, with all having the major allele of IL28B (TT), except 1 (GG). All recipients were reinfected with genotype 1b HCV, and HCV RNA levels were high, >5.0 log IU/mL (5.7–7.8 <log IU/mL). In the histological examination of the graft liver at baseline, F1 was observed in 3 recipients, F2 in 4, F3 in 1, and FCH in 1. A mutation in the core amino acids 70 and 91 was found in 3 (33.3%) and 4 (44.4%) recipients, respectively.
Tac, tacrolimus (mg/day); CyA, cyclosporine (mg/day); MMF, mycophenolate mofetil (g/day).
HCV RNA levels were not tested after 4 weeks, but after 5 weeks in Case 4.
BT, breakthrough; FCH, fibrosing cholestatic hepatitis; HCV, hepatitis C virus; LDLT, living donor liver transplantation; SVR, sustained virological response.
Regarding the previous PEGIFN/R effect, 4 recipients were naive, 2 had relapses, a null response was observed in 2, and 1 was intolerant. Only Case 8 had been treated with telaprevir-based triple therapy 1 year before treatment with PEGIFN/R plus simeprevir; however, it resulted in a relapse.
The median level of total bilirubin, ALT, Cr, and eGFR was 0.9 mg/dL (0.5–25.6 mg/mL), 58.0 IU/mL (10–153 IU/mL), 0.8 mg/mL (0.36–1.95 mg/mL), and 54.0 mL/min (29.9–138.8 mL/min), respectively. Moreover, the median values of Hb, neutrophils, and platelets were 12.0 g/dL (8.5–15.8 g/dL), 2.03 × 103/mm3 (1.18–8.5 × 103/mm3), and 22.8 ×104/mm3 (12.5–37.0 × 104/mm3), respectively. The mean pegylated IFN and ribavirin doses at baseline were 1.44 μg/kg/week and 9.49 mg/kg/day, respectively. All recipients received 100 mg/day simeprevir for 12 weeks. One recipient (Case 8) developed cholangitis due to bile duct stricture requiring endoscopic retrograde biliary drainage at treatment week 4 and 8.
Efficacy
Seven of the 9 recipients (77.8%) completed 24 weeks of treatment and 24 weeks of follow-up, and 2 recipients (22.2%) terminated treatment because of BT. All recipients exhibited a good response to PEGIFN/R plus simeprevir therapy and HCV RNA levels rapidly declined after treatment induction (Fig. 1). RVR, cEVR, and ETR were obtained in 100% (8/8), 88.9% (8/9), and 77.8% (7/9) of recipients treated with PEGIFN/R plus simeprevir, respectively. Furthermore, 7 of the 9 recipients (77.8%) achieved SVR24 (Fig. 2). Two recipients (22.2%) who experienced viral BT at 12 and 16 weeks after treatment were null responders in the previous interferon treatment. No recipient exhibited relapse after treatment.

Plasma viral load in 9 recipients treated with PEGIFN/R plus simeprevir therapy. All recipients exhibited a good response to PEGIFN/R plus simeprevir therapy. Hepatitis C virus (HCV) RNA levels rapidly declined after the induction of therapy. HCV RNA was undetectable 24 weeks after therapy (sustained virological response [SVR]24) in 7 recipients. Two recipients experienced viral breakthrough (BT) at 12 and 16 weeks, respectively. PEGIFN/R, pegylated interferon and ribavirin.

Viral response rate after PEGIFN/R plus simeprevir therapy. RVR, cEVR, ETR, and SVR24 were obtained in 100%, 88.9%, 77.8%, and 77.8% of recipients, respectively, treated with PEGIFN/R plus simeprevir. cEVR, complete early virological response; ETR, end-of-treatment response; RVR, rapid virological response.
Adverse effect
Intolerance to hematological toxicities (Table 2) has been a major concern in anti-HCV treatment based on IFN therapy (Wang and others 2006; Berenguer 2008; Pungpapong and others 2013; Coilly and others 2014). Hemoglobin levels decreased to <8.0 g/dL in 6 recipients (66.7%). Seven of the 9 recipients (77.8%) experienced a 3.0 g/dL decline in hemoglobin levels from baseline. Ribavirin dose reduction was required in 7 recipients (77.8%) and transfusion in 4 recipients (44.4%).
Moderate neutropenia (<1.0 × 103/mm3) was observed in 7 recipients (77.8%), and severe neutropenia (<0.75 × 103/mm3) in 3 (33.3%). Moderate thrombocytopenia (<7.5 × 104/mm3) was reported in 3 recipients (33.3%), and severe thrombocytopenia (5.0 × 104/mm3) in 1 (11.1%). Furthermore, 8 of the 9 recipients (88.9%) required a decreased dose of pegylated interferon because of neutropenia and thrombocytopenia. The expected hematological toxicities, skin rash and itching were observed in 3 recipients.
Simeprevir is reported to be an organic anion-transporting polypeptide 1B1 substrate resulting in unconjugated hyperbilirubinemia (Tischer and Fontana 2014). A mild elevation of total bilirubin levels (<2.0 mg/dL) was observed in all recipients, except in Case 8 and 9 during treatment (Case 8 experienced elevated total bilirubin because of cholangitis, and Case 9, who had FCH at baseline, exhibited high levels of total bilirubin level from therapy induction). No severe adverse effect leading to therapy termination was observed in this study.
Immunosuppression
Trough levels of Tac and CyA in 9 recipients at baseline, 12 and 24 weeks, and at week 12 posttreatment are provided in Figure 3A, B. Tac with or without MMF was administered to 6 recipients (Cases 1, 2, 3, 6, 7, and 8). There was no change in the Tac dose except in Case 3, whose dose was reduced from 2.0 mg/day to 1.5 mg/day at 19 weeks. The mean Tac trough level of 4 cases (Cases 1, 2, 6, and 7), who had been administered the same dosage during and after therapy, was 4.75, 4.01, 3.48, and 2.45 ng/mL at baseline, 12 and 24 weeks, and at week 12 posttreatment, respectively. Decreases in Tac trough levels were observed during and after therapy in Cases 1, 2, and 7.
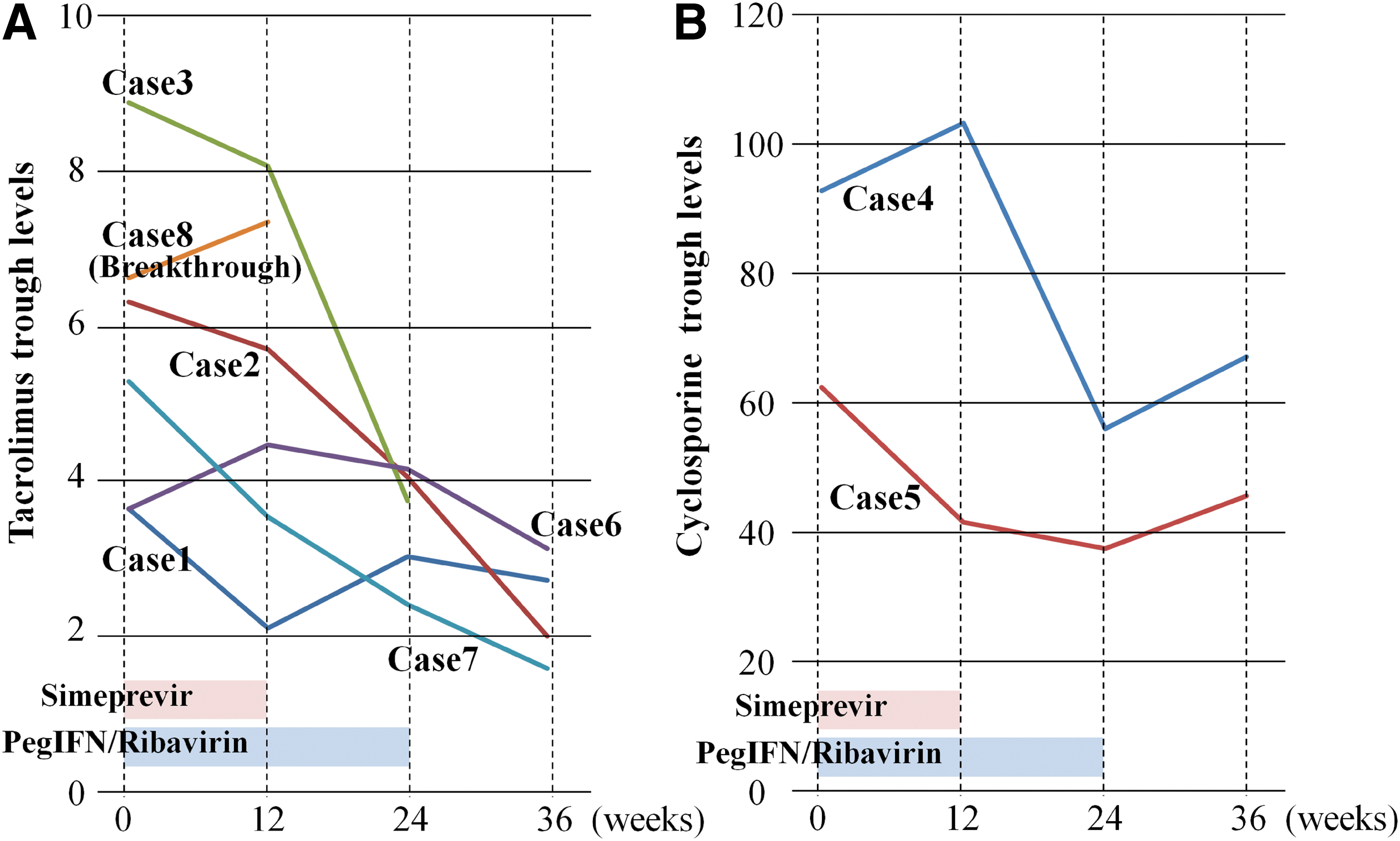
CNI trough levels at baseline, 12 and 24 weeks after therapy induction, and 12 weeks posttreatment in 9 recipients.
Furthermore, CyA with or without MMF was administered to 2 recipients (Cases 4 and 5). In Case 4, 90 mg/day CyA decreased to 70 mg/day at 1 week and was continued at the same dose during therapy. Decreases in CyA trough levels were observed during and after treatment in both Cases 4 and 5. No cellular rejection was observed in any recipients during therapy. However, Case 3 experienced elevated transaminase levels, possibly because of acute cellular rejection after therapy.
Virological resistance mutation at NS3 measurement
No HCV NS3 region mutation conferring resistance to NS3/4A protease inhibitor was detected at pretreatment, except in Case 8. A V36A resistant mutation was reported at baseline in Case 8 (Fig. 4A); this mutation changed from the major population to minor during PEGIFN/R plus simeprevir therapy, and a D168V mutation occurred after BT. In Case 9, R155Q and D168A mutations were detected only after BT.
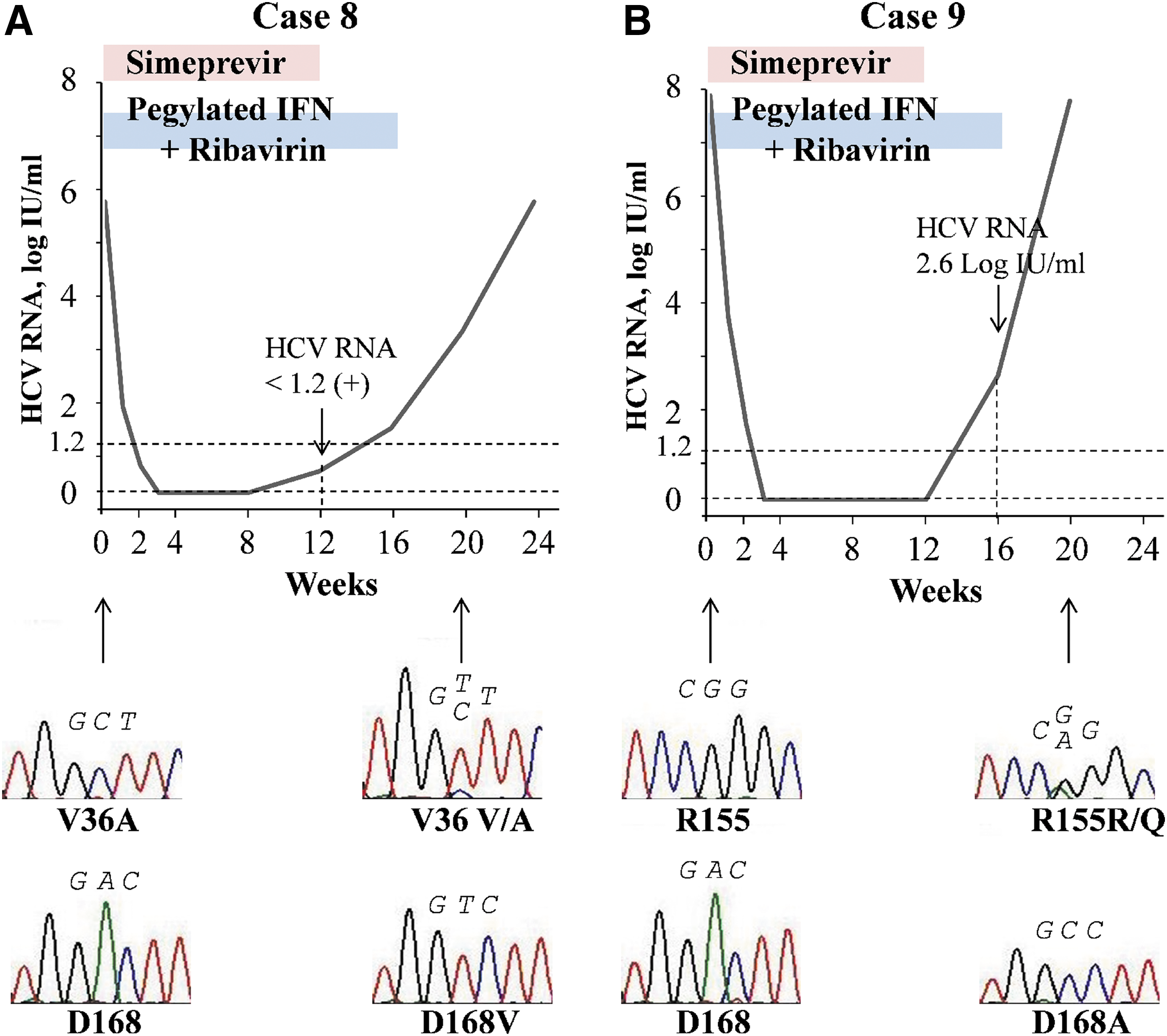
NS3 simeprevir resistance mutations in recipients experiencing viral BT at baseline and after BT.
Discussion
To the best of our knowledge, there have been a small number of studies on the efficacy of simeprevir-based triple therapy in LT recipients (Ikegami and others 2015; Tanaka and others 2015). The current iteration of the AASLD/IDSA/IAS guidelines for the management of HCV in liver transplant recipients does not include the regimen containing PEGIFN. Its use is limited because of the availability of noninterferon-based therapies, including oral direct-acting antiviral agents, which are highly effective and similarly lack drug–drug interactions.
However, the results obtained from this study may be beneficial in certain circumstances, including countries where IFN-free regimens are not available or in cases in which LT recipients have failed IFN-free DAA combination therapy. In particular, this regimen is considered to be potentially beneficial for LT recipients who have failed sofosbuvir (which is NS5B polymerase inhibitor) containing regimen with either daclatasvir or ledipasvir (which are inhibitors of the nonstructural protein NS5A complex), which are the regimens recommended by the AASLD/IDSA/IAS guidelines. The results of this study could be beneficial in these cases in clinical practice.
Most recipients infected with HCV at LT experience reinfection with a rapidly progressing fibrosis (Gane and others 1996; Berenguer and others 2000, 2002; Burton and Everson 2013). Previous studies have reported that the effect of PEGIFN/R therapy in LT recipients was lesser than that in non-LT patients, resulting in a poor survival rate (Picciotto and others 2007; Berenguer 2008; Roche and others 2008; Veldt and others 2008). This is possibly because of discontinuation and dose reduction, owing to frequent adverse effects in LT recipients.
Moreover, immunosuppressant therapy has been assumed to render patients refractory to interferon-based therapy (Hu and others 2003; Boor and others 2006). It has been reported that downregulation of hepatocyte interferon signal is induced by immunosuppressants, particularly corticosteroids (Boor and others 2006). Furthermore, Hirano and others (2008) reported that CNIs inhibited STAT-1 phosphorylation and antiviral activity.
In contrast, it has been clearly demonstrated that SVR following anti-HCV therapy improved the prognosis in LT recipients infected with HCV (Picciotto and others 2007; Veldt and others 2008; Kawaoka and others 2014). More effective anti-HCV therapy is urgently required for improving prognosis in LT patients. Our study provides evidence that simeprevir-based triple therapy is more effective and tolerable to LT recipients with HCV reinfection, despite the small number of study subjects.
In this study, RVR, cEVR, and ETR were obtained in 100%, 88.9%, and 77.8% recipients, respectively, and 77.8% recipients achieved SVR24. Although our study is limited to a small number of recipients, the SVR rate is superior to that reported in a systematic review, which was 28.7% (range, 12.5%–40.0%) of recipients with G1 HCV reinfection achieving SVR by PEGIFN/R therapy (Berenguer 2008). All recipients, except those who had experienced BT, completed the 24-week simeprevir-based triple therapy. The duration of conventional PEGIFN/R therapy was 48 weeks. The shorter duration of simeprevir-based triple therapy is a considerable advantage compared with that of PEGIFN/R therapy.
We have reported our observation on the effect of PEGIFN/R therapy in LT recipients (Ichikawa and others 2009). In this report, Ichikawa and others. have revealed that HCV infection was more refractory in LT recipients than in non-LT patients, and the decline in HCV RNA levels in the early phase after treatment was blocked in LT recipients.
We compared the early phase decline of HCV load in the present data with that in a previous data. The mean decline of HCV RNA levels by simeprevir-based triple therapy was 2.3 log IU/mL after 1 day, >4.4 log IU/at 1 week (<1.2 log IU/mL of HCV RNA was observed in 1 recipient), and >6.0 log IU/mL at 2 weeks (<1.2 log IU/mL of HCV RNA was noted in 5 recipients and undetectable HCV RNA was recorded in 3 recipients). The mean decline in HCV RNA levels by PEGIFN/R was 0.6 log IU/mL after 1 day, 0.8 log IU/mL at 1 week, and 1.1 log IU/mL at 2 weeks in the previous study. Moreover, RVR was observed in 100% recipients treated with simeprevir-based triple therapy, while no RVR was observed in recipients treated with PRGIFN/R. Hence, the effect of simeprevir-based triple therapy was superior to that of PEGIFN/R therapy from the early phase of treatment.
All recipients were reinfected with genotype 1b HCV in this study. There have already been several studies demonstrating the efficacy of first-generation protease inhibitor-based triple therapy in LT recipients with G1 HCV (O'Leary and others 2013; Pungpapong and others 2013; Coilly and others 2014); however, the study of efficacy in LT patients with genotype 1b, not including genotype 1a, is very limited.
Coilly and others (2014) reported that SVR12 was obtained in 1 of the 5 eligible recipients (20%) in the telaprevir-based triple therapy group and 5 of 7 eligible recipients (71%) in the boceprevir-based triple therapy group, whose study population include 79% of recipients with genotype 1b (15 of 19) in the telaprevir-based triple therapy group and 72% of recipients with genotype 1b (13 of 18) in the boceprevir-based triple therapy group, respectively.
Whereas, with CyA administration and a very close monitoring of drug–drug interactions with CNIs, reduced-dose telaprevir-based triple therapy is reported to improve the SVR rate (Ikegami and others 2014). In addition, they compared the efficacy between telaprevir-based triple therapy and simeprevir-based triple therapy in combination with PEGIFN/R for 26 recipients (Ikegami and others 2015). The subjects included in this study were from an institution in Japan; therefore, most of the HCV genotype seemed to comprise 1b. The SVR12 rate was 83.3% for the telaprevir-based triple therapy group and 64.3% for the simeprevir-based triple therapy group. The SVR rate achieved by simeprevir-based triple therapy was slightly inferior compared with the first-generation protease inhibitor-based triple therapy.
The obvious therapeutic advantage of simeprevir-based triple therapy is that it can be introduced with less consideration regarding drug–drug interaction with CNIs unlike first-generation-based triple therapy. In this study, all recipients continued the previous immunosuppressive therapy at the same dosage as before therapy induction.
It has been reported that the effect of coadministration of telaprevir and boceprevir has a dramatic effect on the blood levels of CNIs (Kiser and others 2012). In a study on healthy individuals, the area under the curve (AUC) of Tac and CyA increased by 70.3 and 4.6-fold when coadministered with telaprevir (Garg and others 2011) and by 17.1 and 2.7-fold when coadministered with boceprevir, respectively (Hulskotte and others 2012). The recipients treated with telaprevir- and boceprevir-based triple therapy required dose reduction for CNIs and very close monitoring of their blood levels.
By contrast, coadministration with simeprevir could be introduced without dosage reduction of CNIs and with a reduced requirement for monitoring. Ouwerkerk–Mahadevan et al. reported that the AUC of Tac decreased by 17% and that of CyA increased by 19% when coadministered with simeprevir (Tischer and Fontana 2014). The effect of coadministration of CNIs with simeprevir is very small compared to with telaprevir and boceprevir.
After therapy induction with a dosage similar to that of the previous dosage of CNIs, 2 of the 7 recipients experienced CNIs dose reduction due to early elevation of trough level in our study (Case 3 and 4). However, trough levels of CNIs by the end of treatment were lower than those at baseline in 6/7 recipients who had completed treatment (Fig. 4), and the lower trough levels of CNIs lasted 12 weeks after treatment unexpectedly. Additionally, liver dysfunction probably caused by acute cellular rejection occurred not during, but only 3 weeks after treatment in Case 3.
Changes in trough levels similar to those observed in our study have been reported in a study by Ueda and Uemoto (2016) recently, which showed an increase in CNIs trough level during the first 2 weeks after therapy induction, followed by a decrease after 2 weeks of therapy. They proposed that the initial trough level elevation was caused by the interaction of simeprevir with CNIs and that the trough level decrease after 2 weeks of therapy induction was caused by an increased metabolism of CNIs by the improvement in liver function with HCV clearance.
Kugelmas and others (2003) also reported the decrease of CNIs trough in recipients who had experienced response to antivirus therapy. It has been assumed that HCV clearance improves hepatic microsomal function, which in turn results in decreased CNI blood levels. Although drug–drug interaction between simeprevir and CNIs was little in healthy individuals, monitoring blood CNI levels is necessary during treatment because of the possibility of dramatic CNIs trough level change. Additionally, recipients who obtain viral clearance must continue to be evaluated for acute cellular rejection by CNI monitoring until even if after treatment.
Two recipients experienced BT, and they had been previous PEGIFN/R null responders. Simeprevir-based triple therapy in non-LT patients who had been null responders in previous PEGIFN/R treatment revealed lesser efficacy compared with naive and relapse patients (Zeuzem and others 2014). Although our study included a limited number of subjects, it is quite likely that previous effect of interferon therapy is involved in the efficacy of simeprevir-based triple therapy. Simeprevir-based triple therapy is considered to be similar to simeprevir monotherapy in recipients who had been null responders to PEGIFN/R therapy. HCV RNA quasispecies in null responders are not under unselective immune pressure induced by IFN, which in turn result in NS3 mutations conferring resistance to simeprevir. Simeprevir monotherapy against G1 HCV patients has been reported to induce NS3 resistance mutation as early as 3 days following initiation (Reesink and others 2010).
Furthermore, in this study, D168 resistant mutations that had been undetectable at baseline were found after treatment in both recipients who had experienced BT, and a R155K resistant mutation was found in Case 9. In Case 8, a V36A mutation, which had been reported to confer resistance to first-generation NS3/4A protease inhibitors, was detected at baseline. Given the low prevalence of the V36A mutation in the Japanese HCV G1 population (Suzuki and others 2012), the V36A mutation in Case 8 appears to be induced by telaprevir-based triple therapy 1 year before simeprevir-based therapy. This mutation decreased and changed to nonpredominating after BT.
Importantly, no recipient experienced severe adverse effects that terminated the simeprevir-based triple therapy. A systematic review has shown that the discontinuation rates of PEGIFN/R therapy reached approximately 25% in LT recipients (Wang and others 2006; Berenguer 2008), which is identical to that reported in a previous PEGIFN/R study (Ichikawa and others 2009). Frequent adverse effects predominantly include hematological toxicities.
A total of 66.7% of recipients experienced anemia (Hb <8.0 g/dL) in our study, whereas 32% recipients reported to experience anemia (Hb <8.0 g/dL) in a study by Coilly and others (2014) using first-generation-based triple therapy. However, these figures are difficult to compare because we did not use erythropoietin for anemia. Ikegami and others (2014) reported that anemia (Hb <8.5 g/dL) occurred in 63.6% recipients treated with telaprevir-based triple therapy, which is almost the same frequency as that in the present study.
Moreover, in a recent report on the comparison between telaprevir- and simeprevir-based triple therapy in non-LT patients, the incidence of grade 3 and grade 4 anemia and the requirement for ribavirin reduction, using erythropoietin and blood transfusion, has been reported to be lower in simeprevir-based triple therapy than in telaprevir-based triple therapy (Reddy and others 2015). There were no severe adverse effects due to simeprevir, including hyperbilirubinemia and skin rash. Simeprevir-based triple therapy is believed to be safe or at least as safe as telaprevir-based triple therapy.
In conclusion, high efficacy and tolerability of simeprevir-based triple therapy in LDLT recipients with HCV reinfection was demonstrated in this study of patients who followed up 24 weeks after therapy. Simeprevir-based triple therapy is considered to be available for LDLT recipients. Although the effect by coadministration with simeprevir on CNI concentration is less than that by first-generation protease inhibitors, CNI trough levels should still be monitored during and after treatment. The present study involved a limited number of recipients. Therefore, further studies with a larger number of recipients are urgently required to assess the benefits of simeprevir-based triple therapy in LT recipients with HCV reinfection. However, with new anti-HCV agents being developed, bright prospects are expected for LT recipient refractory to anti-HCV therapy.
Footnotes
Acknowledgments
The authors would like to thank their colleagues in the Department of Gastroenterology and Hepatology, Graduate School of Biomedical Sciences, Nagasaki University, for their kind cooperation and support and Enago (
Author Disclosure Statement
No competing financial interests exist.