
Abstract
The phase 2b EMERGE study compared the efficacy/safety of peginterferon lambda-1a (Lambda) and peginterferon alfa-2a (Alfa), both with ribavirin (RBV), for treatment of chronic hepatitis C virus (HCV) infection. A key safety finding was a higher frequency of hyperbilirubinemia with Lambda/RBV versus Alfa/RBV. To characterize mechanisms of hyperbilirubinemia associated with Lambda/RBV, we conducted a retrospective analysis of safety data from the HCV genotype 1 and genotype 4 cohort of the EMERGE study. Subjects were randomized to once-weekly Lambda (120/180/240 μg) or Alfa (180 μg), with daily RBV, for 48 weeks. Early-onset Lambda/RBV-related hyperbilirubinemia events (6–12 weeks) resulted mostly from RBV-induced hemolysis evidenced by sustained reticulocytosis and a predominantly unconjugated pattern of hyperbilirubinemia. The higher hyperbilirubinemia frequency with Lambda/RBV versus Alfa/RBV was attributed to bone marrow suppression known to occur with Alfa but not Lambda. Late-onset (>12 weeks) Lambda/RBV-related hyperbilirubinemia events occurred most frequently with higher Lambda doses and were associated with increased levels of hepatic transaminase and direct bilirubin fractions compared with early events. This dual pattern of hyperbilirubinemia observed while on Lambda/RBV treatment is thought to be caused by exaggerated RBV-induced hemolysis in early-onset events compared with possible direct Lambda-induced hepatocellular toxicity in late-onset events.
Introduction
P
Previously reported studies assessing safety and tolerability have identified the differences in toxicity between Lambda/RBV and Alfa/RBV (Freeman and others 2014; Muir and others 2014). The phase 2b EMERGE study results showed that treatment of chronic HCV infection with Lambda/RBV was more frequently associated with sudden, grade 3 and 4 increases in bilirubin with or without elevated hepatic transaminase levels compared with Alfa/RBV (ClinicalTrials.gov ID: NCT01001754; Muir and others 2014). For most subjects affected, these events did not impact treatment efficacy and manifested with only minimal symptoms (itching most frequently reported); furthermore, no pathological effect was noted in liver biopsies taken from 2 subjects at the time of the events. Across all affected subjects, temporary drug discontinuation followed by resumption of dosing resulted in reversal and no recurrence of the events.
Hyperbilirubinemia events were not as strongly related to dose as increases in hepatic transaminase events; the frequency of these latter events ultimately led to discontinuation of the development of the Lambda 240 μg dose (Muir and others 2014). However, given the high-grade increases in bilirubin and sporadically associated jaundice, especially in subjects with pre-existing liver disease, further investigation was warranted to understand the nature and underlying mechanisms of hyperbilirubinemia, and whether this was an indicator that Lambda could cause liver toxicity/failure. Additionally, Lambda-treated subjects had significantly lower rates of reductions in hemoglobin, white blood cell counts, and platelet counts compared with Alfa-treated subjects, reflecting differential receptor binding of Lambda compared with Alfa to hematopoietic stem cells. We hypothesized that at least 2 different mechanisms were responsible for the hyperbilirubinemia events associated with Lambda/RBV treatment.
The mechanisms of normal bilirubin conjugation and clearance and the disruptions in this pathway that may lead to hyperbilirubinemia (Supplementary Fig. S1; Supplementary Data are available online at
In brief, bilirubin is the product of heme catabolism. Approximately 80% of bilirubin originates from degradation of erythrocyte hemoglobin in the reticuloendothelial system, whereas up to 20% is derived from inefficient erythropoiesis in bone marrow and degradation of other heme proteins. Once heme is metabolized, it is conjugated to uridine diphosphoglucuronic acid (UDPGA) within hepatocytes to form mono- and diglucuronides of bilirubin, thereby reducing the unconjugated form circulating in the blood. The exact mechanism of uptake into hepatic cells is unknown but is thought to be mediated through passive diffusion as well as by active transport, the latter mediated through organic anion-transporting polypeptide 1B1 (OATP1B1) and possibly organic anion-transporting polypeptide 1B3 (OATP1B3). Upon entering the hepatic cell, unconjugated bilirubin is bound to ligandin within the cytoplasm and is transported to the endoplasmic reticulum, where conjugation with glucuronic acid occurs by the enzyme uridine diphosphate glucuronosyltransferase 1A1 (UGT1A1). Once conjugated, bilirubin glucuronides can be excreted into the bile or back into the sinusoidal blood through active transport. Elimination of conjugated bilirubin into the bile is primarily mediated by the transporter multidrug resistance protein 2 (MRP2)/ATP-binding cassette subfamily C member 2 (ABCC2), whereas introduction of bilirubin glucuronides into the sinusoidal blood occurs through multidrug resistance protein 3 (MRP3)/ATP-binding cassette subfamily C member 3 (ABCC3), where they could once again be transported back into hepatocytes through OATP1B1/3.
Hyperbilirubinemia can result from defects or alterations in any of the above steps or a combination thereof. Additionally, hyperbilirubinemia observed in the context of increased hepatic transaminases is hypothesized to be related to a direct hepatic toxicity mechanism.
In vitro investigation of the effect of Lambda on normal bilirubin clearance mechanisms (Bristol-Myers Squibb 2013) showed that Lambda did not alter the distribution of MRP2 on the canalicular membranes of sandwich-cultured primary human hepatocytes or the activity of OATP1B1, OATP1B3, MRP3, multidrug resistance protein 1/P-glycoprotein (MRP1/P-gp), or bile salt excretory pump, all key transporters in the regulation of bilirubin. The gene expression of both UGT1A1 and MRP2 was upregulated to a minor extent by Lambda, but the positive control Alfa demonstrated a similar in vitro pattern in the regulation of these transporters. These results were not consistent with, and did not explain, the clinical pattern of hyperbilirubinemia observed for Lambda and Alfa (Muir and others 2014). Given the lack of significant effects on drug-metabolizing enzymes and transporters involved in the disposition of bilirubin, a retrospective analysis of EMERGE safety data was conducted to better characterize and identify mechanism(s) of hyperbilirubinemia associated with Lambda/RBV therapy.
Materials and Methods
EMERGE study
The EMERGE study has been described in detail elsewhere (Muir and others 2014). Briefly, this was a randomized, blinded, actively controlled, multicenter phase 2b dose-ranging study that evaluated the efficacy and safety of Lambda/RBV versus Alfa/RBV in 526 noncirrhotic, treatment-naive adults chronically infected with HCV genotype (GT) 1, 2, 3, or 4. Eligible subjects were randomized 1:1:1:1 to receive subcutaneous Lambda (120, 180, or 240 μg) or Alfa (180 μg) once weekly in combination with daily oral RBV (Supplementary Fig. S2). Planned treatment length was 24 and 48 weeks for HCV GT2 and 3 and GT1 and 4 subject cohorts, respectively. All subjects were followed for 24 weeks posttreatment. Adverse events and clinical laboratory test results were recorded throughout the treatment and follow-up periods.
Retrospective analysis
EMERGE study data included in this retrospective analysis were derived from the HCV GT1 and 4 subject cohort (N = 407). Data from the GT2 and 3 subject cohort were not included due to the small subject number, different RBV dose, and shorter duration of treatment compared with the GT1 and 4 subject cohort. Changes in hepatic and hematological parameters during randomized treatment were evaluated and visualized using TIBCO® Spotfire® software version 4.5.0 (Somerville, MA).
Since the EMERGE study lacked pharmacogenetic data to include in the present analysis, pharmacogenetic data were alternatively derived from a phase 3 study assessing hyperbilirubinemia and inosine triphosphate pyrophosphatase (ITPA) GTs (Foster and others 2015) to support initial findings of the EMERGE study retrospective analysis. Specifically, rates of hyperbilirubinemia (grade 1–4) in the phase 3 study were compared with rates of hyperbilirubinemia in the EMERGE study. In addition, the relationship between ITPA activity and the frequency of hyperbilirubinemia events (especially grade 3 and 4 events) was determined.
Results
Summary of previously reported hepatic and hematological parameter changes in the HCV GT1 and 4 subject cohort of the EMERGE study
A cohort of 407 subjects with chronic HCV GT1 or 4 infection was randomized to receive weekly Lambda (120 μg, n = 98; 180 μg, n = 102; 240 μg, n = 104) or Alfa (180 μg, n = 103) in combination with daily RBV (Doyle and others 2006; Everson 2011; Muir and others 2014). Changes in hepatic parameters (total bilirubin, alanine aminotransferase [ALT], and aspartate aminotransferase [AST]) during treatments are summarized in Table 1.
IFN dose reduction was required by protocol amendment in the Lambda 240 μg group as of April 2011.
Maximum severity is the worst severity experienced by a subject across all of his/her events.
AE, adverse event; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GT, genotype; HCV, hepatitis C virus; IFN, interferon; RBV, ribavirin; SAE, serious AE.
This image was published in Muir and others (2014).
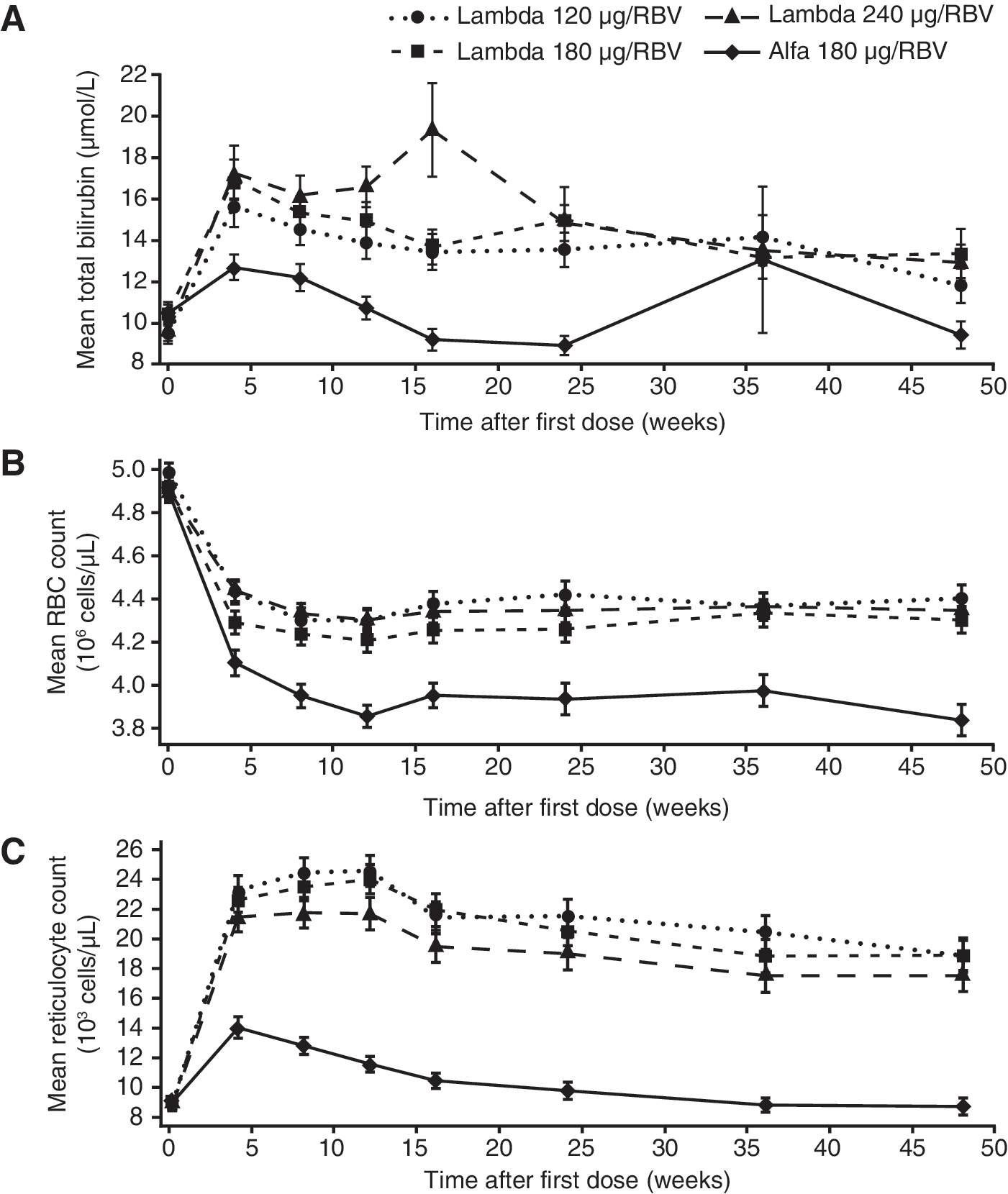
The frequency of grade 3 and 4 ALT and AST elevations with Lambda appeared to be dose related, with transaminase elevations occurring at similar frequencies for the Lambda 120 and 180 μg groups and the Alfa group, and at higher frequencies for the 240 μg group (the Lambda 240 μg dose was discontinued during the study due to high discontinuation rates resulting from elevated hepatic transaminases). Grade 3–4 increases in total bilirubin, however, seemed to occur less frequently among the Alfa and Lambda 120 μg groups compared with the Lambda 180 and 240 μg groups. Incidence of reductions in hematological parameters, including hemoglobin, neutrophils, and platelets, were lower in the Lambda groups compared with the Alfa group. In particular, mean hemoglobin levels were reduced in all treatment groups, but to a greater extent in the Alfa group (Fig. 1). The mechanism behind these hematological differences is thought to be related to the differential bone marrow suppressive effects of Lambda compared with Alfa (Anderson and others 2013). As shown in Fig. 2B, higher red blood cell (RBC) counts are maintained in the Lambda dose groups compared with the Alfa group, despite RBV-induced hemolysis occurring in all groups. The higher RBC counts are accompanied by a greater sustained reticulocyte response in all Lambda dose groups versus the Alfa group (Fig. 2C).
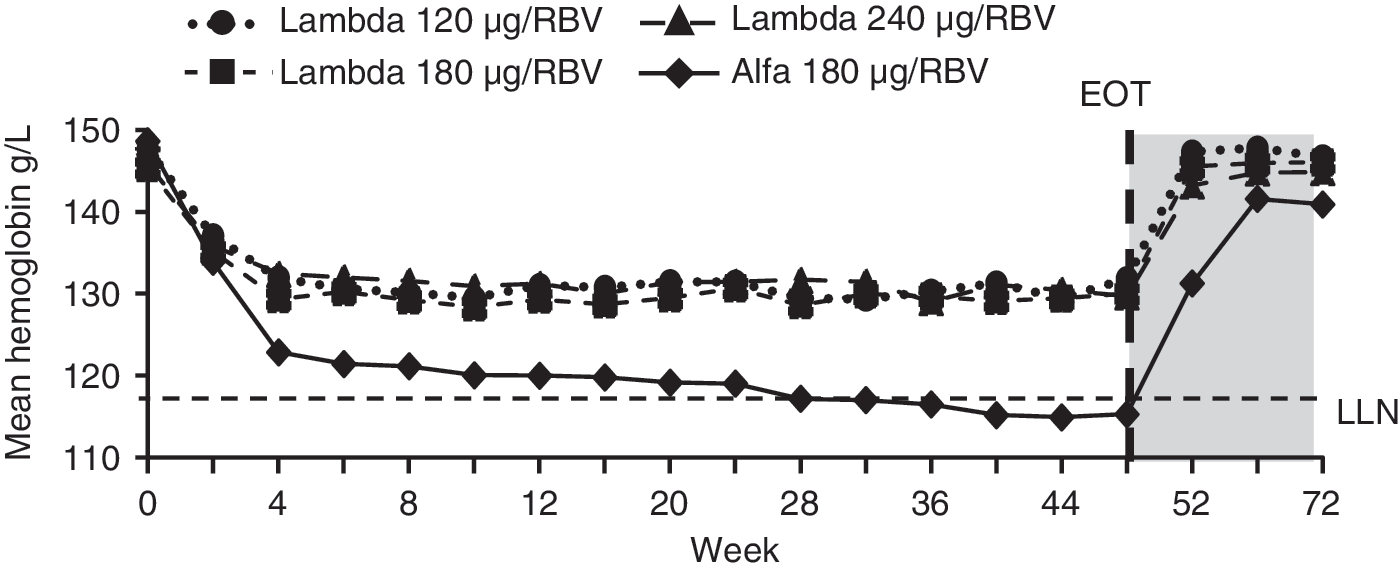
Hemoglobin over time in subjects with chronic HCV GT1 and 4 infection treated with Lambda/RBV or Alfa/RBV in the EMERGE study. EOT, end of treatment; GT, genotype; HCV, hepatitis C virus; LLN, lower limit of normal; RBV, ribavirin. This image was published in Muir and others (2014).
Mean
Retrospective characterization and investigation of potential mechanism(s) of hyperbilirubinemia associated with Lambda/RBV in the HCV GT1 and 4 subject cohort of the EMERGE study
Hyperbilirubinemia events occurred within the first 12 weeks of treatment, with a higher frequency of grade 3 and 4 hyperbilirubinemia events in men (27/260; 10.4%) versus women (4/178; 2.2%) and with no relationship between these events and age (data not shown). The temporal pattern of mean total bilirubin level (Fig. 2A) in the Alfa/RBV group was similar to that observed in the Lambda 120 and 180 μg groups (although with lower quantitative values for Alfa), suggesting a similar underlying mechanism of hyperbilirubinemia with Lambda and Alfa treatments during the first 4–6 weeks of therapy. For the Lambda 240 μg group, however, a second peak occurred after week 12, suggesting additional reasons for increases in bilirubin levels with that dose. Alfa/RBV-induced increases in bilirubin are well described in the literature and are attributed mostly to RBV-induced hemolysis (Ishigami and others 2010).
In this study, both treatments resulted in an initial elevation in mean total bilirubin level (Fig. 2A) that correlated with a concurrent drop in the total RBC count (Fig. 2B) and a rise in the mean absolute reticulocyte count (Fig. 2C). The magnitude of the increase in absolute reticulocyte count was greater with Lambda (Fig. 2C), whereas the reduction in RBC count was considerably greater with Alfa (Fig. 2B). This suggests that the basic mechanism of hyperbilirubinemia observed with both Lambda and Alfa is RBV-induced hemolysis, and that the differential impact of the 2 treatments on bone marrow synthesis and RBC turnover accounts for the difference in the magnitude of hyperbilirubinemia (ie, Lambda permits a higher level of persistent reticulocytosis and a sustained increase in RBC turnover [quantity of RBCs at risk of RBV-induced hemolysis], whereas Alfa induces bone marrow suppression and prevents the compensatory increase in RBC turnover). If RBV-induced hemolysis is indeed the common driver for hyperbilirubinemia with both Lambda and Alfa, over time a predominantly unconjugated (indirect) pattern of hyperbilirubinemia would be expected with both treatments, as was observed with all doses of Lambda and Alfa (Fig. 3).
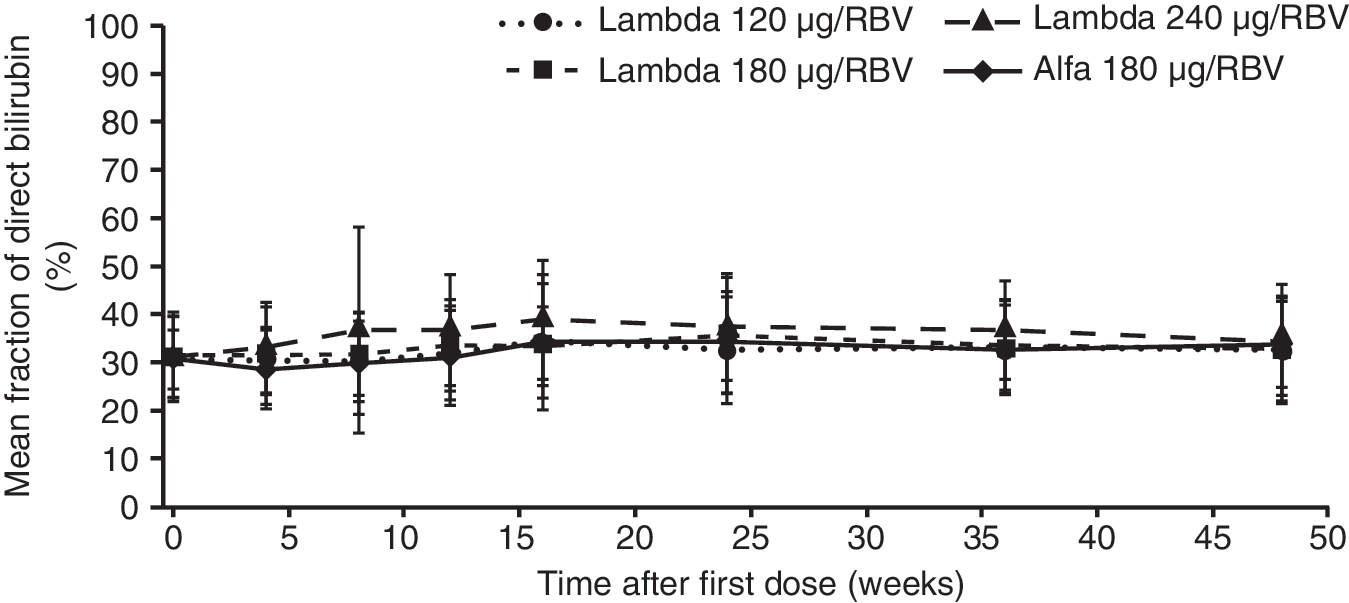
Direct (conjugated) bilirubin as a fraction of total bilirubin over time.
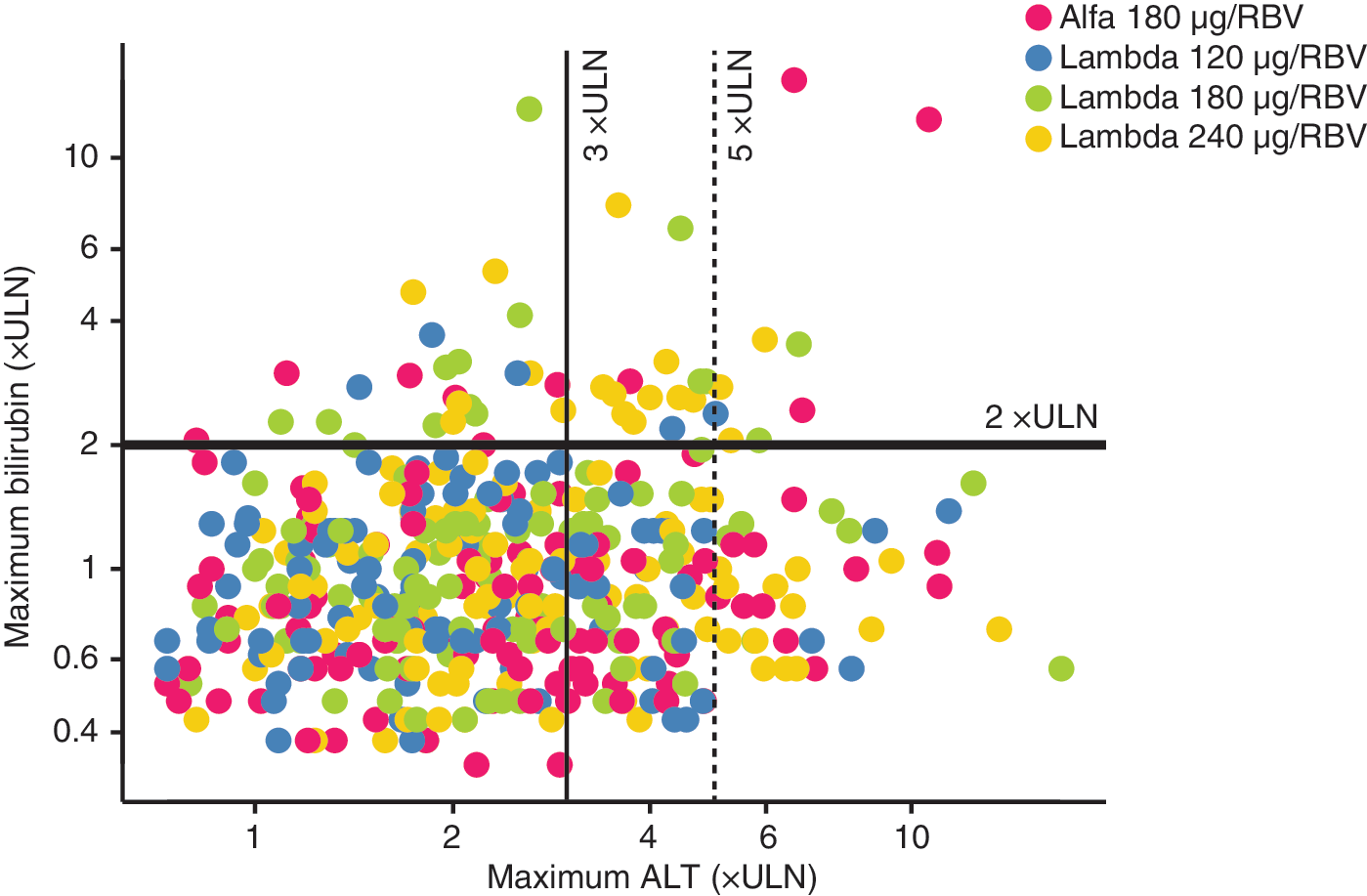
However, Fig. 3 shows a trend for a slight separation of the Lambda 240 μg group from the other groups, suggesting an additional mechanism underlying this Lambda dose. To provide additional information on the possible relationship between treatment and mechanisms of hemolysis, maximum bilirubin was plotted against the fraction of direct bilirubin for each treatment arm (Fig. 4). Assuming that levels of direct bilirubin <50% are primarily indicative of increased hemolysis (likely due to RBV), whereas higher fractions of direct bilirubin (>50%) are primarily associated with hepatotoxicity (likely due to high IFN levels), the results suggest that the majority of hyperbilirubinemia events (>60%) were predominantly associated with the indirect bilirubin fraction, suggesting an etiology of hemolysis. These results have been observed in other studies with Alfa/RBV (Ishigami and others 2010) and were confirmed in this study's ITPA analysis.

Maximum bilirubin versus fraction of direct bilirubin. IFN, interferon; RBV, ribavirin; ULN, upper limit of normal.
In contrast, the events resulting in a direct bilirubin fraction >50% were associated mostly with the highest dose of Lambda and, as described in the following section, were also more likely to be associated with high-grade increases in values of ALT, suggestive of direct hepatocellular toxicity.
Dual mechanism hypothesis to explain events of hyperbilirubinemia
As explained in previous sections, differences in the temporal patterns of mean total bilirubin levels after week 12 and the greater tendency for increases in hepatic transaminases with the Lambda 240 μg dose led to our hypothesis that a second mechanism (ie, direct hepatocellular toxicity) in addition to RBV-induced hemolysis, could be responsible for the observed hyperbilirubinemia events. One possibility is hyperbilirubinemia due to IFN-induced hepatocellular apoptosis, which has been described with the use of high doses of Alfa-IFNs (eg, treatment of melanoma) (Kirkwood and others 2002).
An evaluation of drug-induced serious hepatotoxicity (eDISH) plot of maximum total bilirubin against maximum ALT reveals a pattern of high ALT values and high bilirubin values as would be expected in the event of direct hepatocellular toxicity (Fig. 5) (U.S. Department of Health and Human Services Food and Drug Administration 2009). Data points indicating increases in total bilirubin (>2 × ULN) are seen in both the upper right and left quadrants, with or without high-grade increases in ALT. When examining the treatment assignment of subjects in these 2 quadrants, those on the Lambda 240 μg dose (indicated by yellow dots in Fig. 5) tended to be clustered in the upper right quadrant compared with all other dose groups, suggesting a possibility of direct hepatocellular toxicity with the Lambda 240 μg dose. However, given that subjects were allowed to enter the study with values of ALT ≥5 × ULN, we further refined Fig. 5 by plotting maximum bilirubin values and the concurrent ALT value (Supplementary Fig. S3). This figure also suggests that the Lambda 240 μg dose is associated with a higher proportion of concurrent incidence of high ALT and total bilirubin.
eDISH plot of maximum bilirubin versus maximum ALT. ALT, alanine aminotransferase; eDISH, evaluation of drug-induced serious hepatotoxicity; RBV, ribavirin; ULN, upper limit of normal.
To further confirm this effect, we examined the fraction of conjugated bilirubin as a surrogate for defining whether or not an episode was due to hemolysis, direct hepatocellular toxicity, or possibly both. Figure 4 shows that increased bilirubin values with a high conjugation fraction (>50%) were disproportionally represented in the Lambda 240 μg dose group compared with the other dose groups (Lambda 240 μg, 15.1%; Lambda 180 μg, 6.5%; Lambda 120 μg, 0.9%; Alfa, 3.7%). This pattern would be expected in direct hepatocellular injury, whereas the majority of subjects in the Alfa, Lambda 120 and 180 μg groups had abnormal bilirubin levels with a low conjugation fraction (<30%), suggesting a hemolytic mechanism.
Additional data supporting initial retrospective analysis findings
Pharmacogenetic data from the AI452-017 phase 3 study (Foster and others 2015) provide additional evidence to support the complex mechanism(s) of hyperbilirubinemia associated with IFN therapy in subjects with HCV infection.
Functional variants in ITPA are associated with differing rates of RBV-induced anemia in HCV-infected subjects. ITPA deficiency leads to an accumulation of ITP that competes with RBV-TP (an active form of RBV), avoiding accumulation in RBCs (Fellay and others 2010). The AI452-017 study evaluated 2 ITPA single nucleotide polymorphisms (SNPs), rs1127354 and rs7270101, and predicted ITPA activity. Figure 6 shows the frequency of grade 1–4 hyperbilirubinemia by ITPA SNP GT and predicted ITPA activity. Rates of hyperbilirubinemia in AI452-017 were similar to the EMERGE study. These results show that GTs with higher ITPA activity (ie, more sensitive to RBV-induced anemia) had a higher frequency of hyperbilirubinemia events (especially grade 3 and 4 events) compared with those GTs with lower ITPA activity.
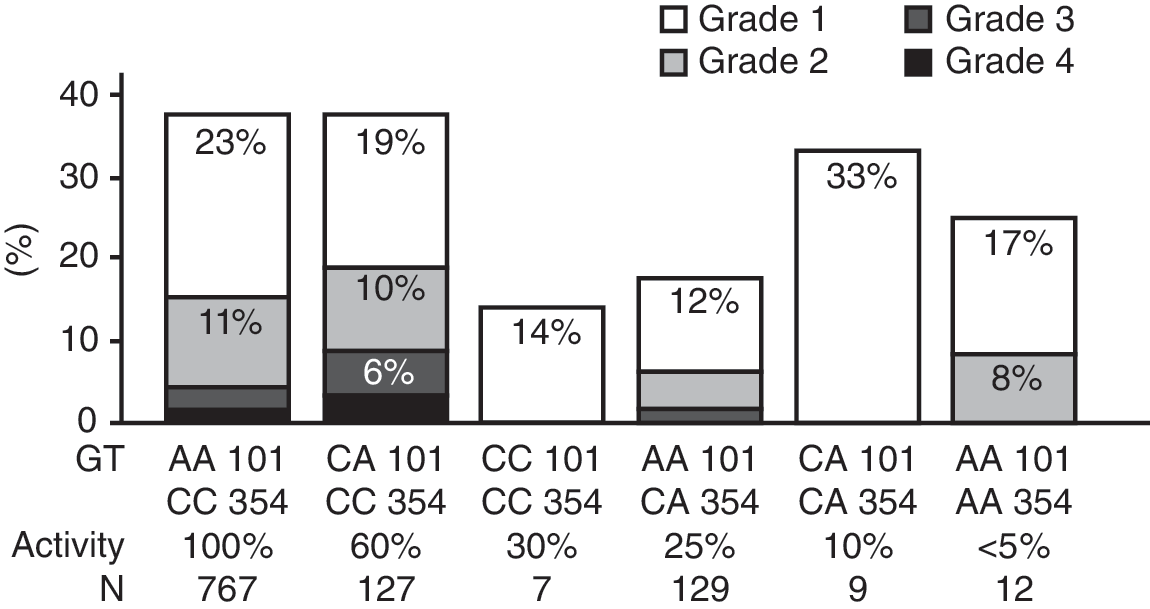
Frequency of grade 1–4 hyperbilirubinemia by ITPA GT in the AI452-017 phase 3 study. ITPA, inosine triphosphate pyrophosphatase; GT, genotype.
Discussion
Results of this retrospective investigation suggest that at least 2 different mechanisms are responsible for the higher frequency of hyperbilirubinemia associated with Lambda/RBV versus Alfa/RBV therapy in the HCV GT1 and 4 subject cohort of the phase 2b EMERGE study. Early hyperbilirubinemia events, occurring during the first 6–12 weeks of treatment, were associated with increased production of bilirubin that likely resulted predominantly from RBV-induced hemolysis, as has been previously described with Alfa/RBV therapy. The higher frequency of hyperbilirubinemia associated with Lambda/RBV versus Alfa/RBV, in the context of this initial elevation, is thought to be related to the differential bone marrow suppressive effect of Lambda and Alfa. This effect results in a greater number of RBCs at risk of hemolysis throughout the duration of treatment with Lambda/RBV. Furthermore, while these early events were sometimes accompanied by a high concurrent ALT due to underlying disease, the predominantly unconjugated fraction of total bilirubin supported a hemolytic mechanism. Additional supportive data from the examination of ITPA polymorphisms provide further credence to this hypothesis. Later-onset hyperbilirubinemia events, usually occurring after week 12 and disproportionately represented in the Lambda 240 μg group, were associated with greater elevations in hepatic transaminases and a predominantly conjugated fraction of total bilirubin, suggesting a mechanism of IFN-induced direct hepatocellular toxicity, which has been described with other IFNs.
The decision to discontinue the Lambda HCV development program resulted primarily from promising advances in the field of HCV treatment, most notably all-oral therapeutic options. Nevertheless, these results highlight an overlooked fact that drug toxicity can be complex, involving more than 1 mechanistic pathway, especially in the setting of polytherapy. Traditional safety data outputs of adverse events and laboratory data may not allow for a full understanding of the underlying mechanisms when they are complex and/or overlapping. Exploration of data, particularly temporal relationships between different parameters and doses, can be useful for delineating complex mechanisms.
Footnotes
Acknowledgments
Medical writing support was provided by Tracy Wetter (Infusion Communications, Haddam, CT), and editorial assistance was provided by Dena McWain (Infusion Communications, Haddam, CT).
This analysis and writing/editorial support was fully funded by Bristol-Myers Squibb.
Author Disclosure Statement
R.Z., P.N., D.X., N.K., E.M.C., and S.S. are employees of Bristol-Myers Squibb. M.W.R. and M.W.H. are employees of and own stock in Bristol-Myers Squibb.