
Abstract
Hepatitis C virus (HCV) is an Egyptian serious national health problem. The combination of pegylated interferon (PEG-IFN) with ribavirin (RIB) was considered the established therapy for chronic hepatitis C (CHC), and it was associated with several adverse effects, including thyroid dysfunction (TD). The aim of this work was to study TD in CHC patients receiving PEG-IFN+ RIB therapy. This retrospective study included 100 adult patients attending the outpatient clinics at AL-Kahera Al-Fatemya hospital and were eligible candidates for PEG-IFN+ RIB therapy. Thyroid hormonal profile (thyroid-stimulating hormone, free triiodothyronine, and free thyroxine) was done before initiation of treatment (week 0) and at weeks 12, 24, 48, and 72. The incidence of TD was more evident by the end of treatment (week 48); it was found to be 35%, mostly in the form of hypothyroidism, while the least incidence was detected by week 12 (2%), all in the form of hyperthyroidism. Generally, hypothyroidism was higher than hyperthyroidism in multiple folds. Thyroid profile was not significantly related to viral load.
Introduction
H
TD induced by IFN-α takes place in about 10% of patients, likely through immune mediation (Chédin and others 1994), and it is recommended to be notified to the patients earlier (Földes and others, 2004; Nadeem and others, 2010). Thus, thyroid-stimulating hormone (TSH) is recommended to be tested before initiation of SOC, and at least once during treatment (commonly at week 12), and after SOC (Aspinall and Pockros, 2004; Jadali, 2013), to prevent or decrease the occurrence of TD (Jadali 2013).
Aim of the Study
This study aimed at evaluating TD among HCV patients on PEG-IFN+ RIB therapy, including its follow-up regarding incidence, clinical form, influential factors, and its impact on treatment.
Patients and Methods
This was a retrospective study that included CHC patients attending the outpatient hepatology clinics at Al- Kahera Al- Fatemya Hospital, seeking for remedy as it is a member of the National Committee for Control of Viral Hepatitis.
Inclusion criteria are as follows: (a) adult patients (≥18 years), (b) established diagnosis of HCV; virologically by polymerase chain reaction (PCR) and histopathologically by liver biopsy, and (c) eligible candidates for SOC; inclusion criteria are as follows: total leukocyte count >4,000/mm3, neutrophil count >2,000/mm3, platelets >100,000/mm3, HB >12 gm for females & >13 gm for males, prothrombin time <2 s above the upper limit of normal, direct bilirubin ≤0.3 mg/dL & indirect bilirubin ≤0.8 mg/dL, albumin >3.5 g/dL, serum creatinine within normal limit, TSH within normal limit, HBsAg negative, antinuclear antibody (ANA) <1/160, positive anti-HCV and HCV RNA, diabetically controlled (HAIC <8.5%), alpha-fetoprotein <100 ng/mL, female patients practicing adequate contraception, and signed written informed consent before starting treatment.
Exclusion criteria are as follows:
All patients were treated with the combined PEG-INFα-2a (180 mcg/week) and RIB daily (1,000–1,200 mg) for 48 weeks. All patients were subjected to the following: (
TSH (normal population range 0.4–4.2 μIU/L), FT3 (normal population range 1.4–4.2 pmol/L), and FT4 (normal population range 0.8–2 ng/dL) were measured using the Accubind ELISA Kit (Monobind, Inc., Lake Forest, CA). The intra-assay coefficients of variation (CV) for TSH, FT4, and FT3 were 6.6–8.1, 3.25–10.98, and 2.4–11.9, respectively; the interassay CV were 5.9–9.3, 6.01–10.81, and 10.2–13.1, respectively. Hormonal levels were measured 5 times; before initiating SOC = week 0, then during therapy that is weeks 12 and 24, by the end of therapy course (week 48), and finally at week 72 from the start of treatment (6 months after ETR).
(
The study was approved by the institutional research ethics committee.
Results
This study included 100 adult CHC patients who were eligible candidates for PEG-IFN+ RIB therapy. The included patients were middle aged (range 22–59 years, mean age was 43 ± 10 years), and comprised 64 males and 36 females. The laboratory results of the studied patients are shown in Table 1.
• Most of the patients were negative for ANA and schistosomiasis, i.e., 93% and 73%, respectively.
• Hepatic ultrasonographic echopattern is illustrated in pie chart of Fig. 1.
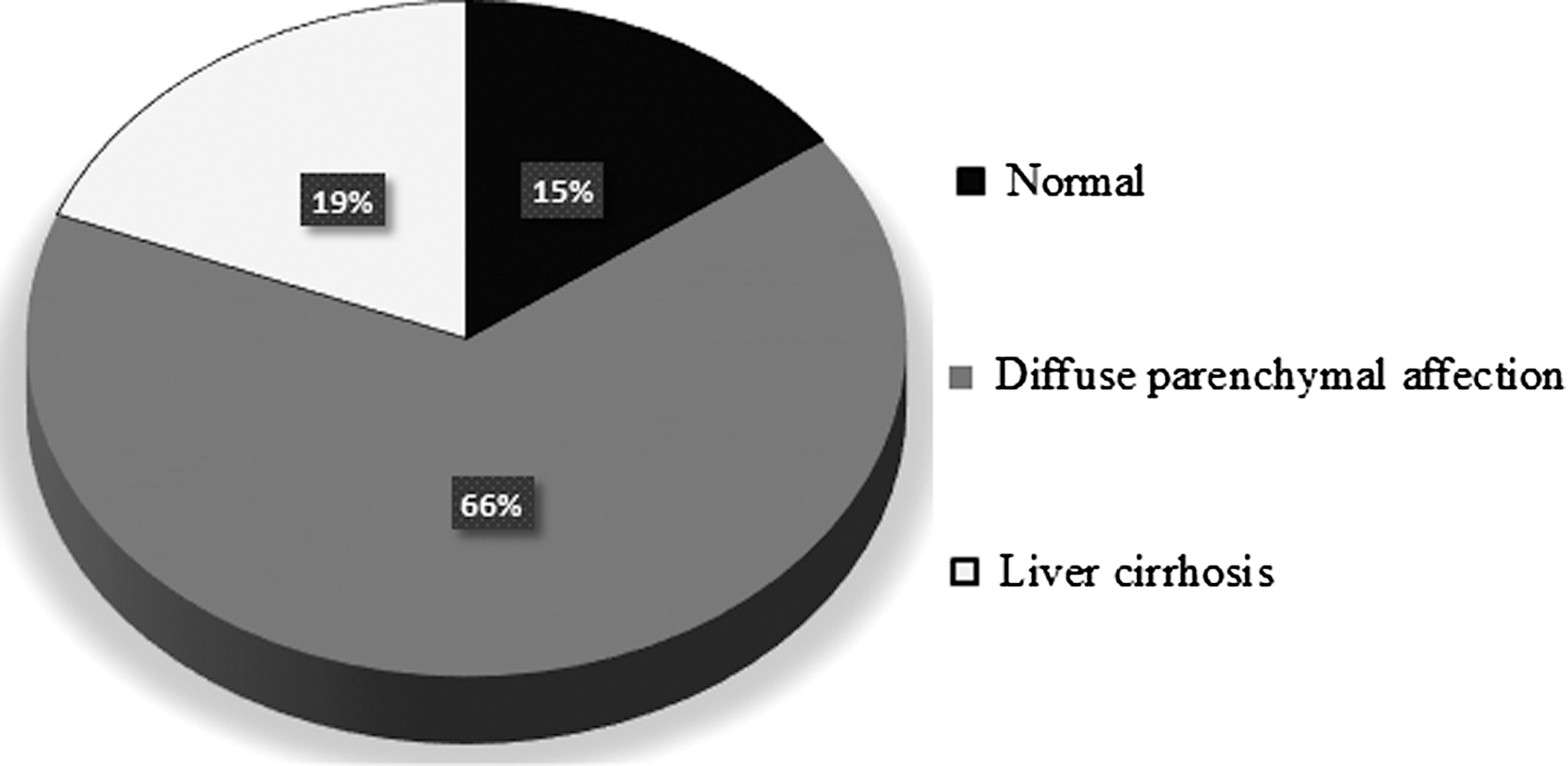
Hepatic parenchyma by US of the studied patients.
AFP, alpha fetoprotein; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CBC, complete blood count; HB, hemoglobin; PC, prothrombin concentration; PCR, polymerase chain reaction; TLC, total leukocyte count.
Thyroid profile along the course of therapy is shown in Table 2.
Bold indicates significant difference.
FT3, free triiodothyronin; FT4, free thyroxine; TSH, thyroid-stimulating hormone.
TD along the PEG-IFN+RIB therapy in the studied patients is shown in Table 3.
Bold indicates significant difference.
In this study, none of the TD patients were clinically manifested along the PEG-IFN+ RIB therapy.
Almost 2/3 of them (22/35 patients; 62.8%, i.e., 1/5 hyperthyroid patients and 21/30 hypothyroid patients) spontaneously became euthyroid at week 72, 4 hyperthyroid patients needed β blocker, while the other hypothyroid patients did not need hormonal replacement therapy.
Comparison between patients with TD (group I) and those with euthyroidism (group II), altogether regarding main demographic features, laboratory results, and viral load at mid (PEG-IFN+ RIB)-treatment (week 24), its end (week 48), and at follow-up (week 72), is shown in Tables 4 and 5, respectively. This was not done at week 12 for the unexpected reliable statistical results as it would be 2 hyperthyroid patients versus 98 euthyroid ones.
HB, hemoglobin; TD, thyroid dysfunction.
Correlation between thyroid hormonal profile and both main baseline investigatory work up, that is laboratory results, histopathology, and viral load prior, along, and at follow-up of PEG-IFN+ RIB therapy (week 72) is shown in Tables 6 and 7, respectively.
Bold indicates significant correlation.
It was found that none of the patients discontinued the PEG-IFN+ RIB therapy.
Discussion
HCV is a significant Egyptian national disease burden that arose long years before (Mohamoud and others, 2013). Antiviral therapy of CHC possibly induces de novo or exacerbates preexisting silent TD (Vezali and others, 2009). There is a wide range of newly developed TD in the treatment of CHC patients with IFN-based therapy (Danilovic and others, 2011; Nair Kesavachandran and others, 2013), regardless of type of IFN (Mekkakia-Benhabib and others, 1996; Kee and others, 2006; Tran and others, 2007), being alone or combined with other drugs (Nair Kesavachandran and others, 2013), dose of IFN (Mekkakia-Benhabib and others, 1996; Dalgard and others, 2002), or type of PEG-IFN (Barut and others, 2012). Also, PEG-IFN+ RIB therapy exacerbates thyroid autoimmunity in susceptible patients who are positive for thyroid autoantibody (Nagayama and others, 1994; Danilovic and others, 2011).
Therefore, patients have to be notified about the possible TD and its screening by hormonal profile (basically TSH) and autoantibodies, which are recommended before, during, and after IFN treatment (Benelhadj and others, 1997; Andrade and others, 2008; Danilovic and others, 2011). In this study, all patients had normal thyroid function and no previous history of thyroid disease. The study aimed at evaluating TD regarding its incidence, form, and influencing factors along the PEG-IFN+ RIB therapy and 6 months after course of SOC (72 weeks from the initiation of treatment).
This study showed that most of the patients were euthyroid along most of the PEG-IFN+ RIB course that is 98%, 93%, and 87% at weeks 12, 24, and 72, respectively. This was close to the fact that sustained euthyroidism was established in most of the patients, that is 92.5% and 80% of the patients, along SOC as reported by Benelhadj and others (1997) and Abdel-Kader and others (2012), respectively. However, it was less evident by the end of treatment (65%).
In this study, TD was not an uncommon side effect of PEG-IFN+ RIB therapy. It was found in 2% and 7% at weeks 12 and 24, respectively. This was close to the 6% reported mean incidence of IFN-α-induced TD by Koh and others (1997), 7.5% by Benelhadj and others (1997), and 8.9% by Kabbaj and others (2006), respectively. Little higher incidence was reported in previous studies, for example 10%, 10.7%, 11.8%, and 12% by Weissel and others (1995), Bini and Mehandru (2004), Dalgard and others (2002), and Mekkakia-Benhabib and others (1996), respectively.
CHC patients on SOC are 11 times more likely to develop TD compared to patients without treatment (Nadeem and Aslam 2012); 16.7%, 16.8%, 18%, 18.69%, 20%, 21.3%, and 21.7% developed TD along the PEG-IFN+ RIB therapy as found by Mammen and others (2012), Barut and others (2012), Nadeem and Aslam (2012), Masood and others (2008), Abdel-Kader and others (2012), Vezali and others (2009), and Földes and others (2004), respectively. Actually, a wide range of TD prevalence during therapy was reported (Nair Kesavachandran and others, 2013), for example it was 1.1%–21.3% in the retrospective Chinese study (Tran and others, 2013).
On the other hand, the highest incidence was reported by the end of treatment (35% at week 48). This was higher than other results, for example 11.5% and 12.6% by Yan and others (2012) and Kee and others (2006), respectively. The range 6.7%–21.3% by the end of treatment was also found by Tran and others (2013), and on the contrary, TD showed decline along the PEG-IFN+ RIB course in a Taiwani study (Hsieh and others, 2000).
Also, the incidence of TD was 13% at follow-up (week 72). This was within the range 6.7%–21.3% (Tran and others 2013), but higher than a Saudian prospective study of PEG-IFN+ RIB therapy for 48 weeks that is 7.4% (Albaker and others 2013), while the highest incidence was 46%, which was reported by Danilovic and others (2011).
In this study, hypothyroidism was significantly more common than hyperthyroidism. This agreed with many previous studies (Koh and others, 1997; Nadeem and Aslam, 2012), even in cases other than CHC (Lowndes and others, 2010). Its incidence at weeks 24, 48, and 72 were 6/7; 85.7%, 30/35; 85.7%, and 9/13; 69.2% of TD, respectively. Moreover, it was found higher with multiple folds than hyperthyroidism that is 6% versus 1%, 30% versus 5%, and 9% versus 4% at weeks mentioned before. This was similar to many previous studies, for example 50% versus 3%, 18.% versus 3.3%, 16.6% versus 3.4%, 15% versus 3%, 9% versus 4.3%, and 5.6% versus 1.8% by Weissel and others (1995), Vezali and others (2009), Abdel-Kader and others (2012), Masood and others (2008), Mekkakia-Benhabib and others (1996), and Albaker and others (2013), respectively, despite the different HCV genotypes, for example the former Egyptian study was applied on genotype 4, while the last Saudian study was applied on genotype 1. This may be attributed to the additive effect of ribavirin (Carella and others, 2002). High incidence of hypothyroidism was hypothesized by immune-mediated mechanism that is IFN, as an immune-modulatory agent, interacts with the inflammatory cascade (Tilg, 1997) leading to rise of thyroid autoantibodies and damage of thyroid gland (Andrade and others, 2008).
On the other hand, RIB synergistically induces cellular destruction predominantly by stimulating the cytotoxic and cytolytic pathways (Lowin and others, 1994), plus the direct glandular epithelial destruction and thyrocyte death (Akeno and Tomer, 2007).
Conversely, hyperthyroidism was the only detected TD earlier along PEG-IFN+ RIB therapy (2% at week 12). This was similar to Costelloe and others (2009). It was found that hyperthyroidism at week 12 coincides with established autoimmune mechanism (Lowndes and others 2010). Then, in this study, it was reported, but less than hypothyroidism along and at follow-up of PEG-IFN+ RIB therapy, while Benelhadj and others (1997) found that hypothyroidism and hyperthyroidism were comparable as well.
In this study, FT3 showed a highly significant successive decrease along the PEG-IFN+ RIB therapy in the studied patients (P < 0.016, P < 0.001, and P < 0.001 at weeks 12, 24, and 48, respectively), while FT4 lagged behind, that is it started to show a significant decrease only by the end of treatment (P < 0.042). However, only T3 showed a decrease, while FT4 and TSH were rather stable in the study done by Danilovic and others (2011).
TSH results showed a significant increase (P < 0.001) along the course of PEG-IFN+ RIB therapy and at follow-up, more than FT3 and FT4.
In this study, TD did not show a significant relationship with either gender or age, or baseline laboratory results. That was contrary to the fact that females are known to have a higher risk to develop TD (Weissel and others 1995; Mekkakia-Benhabib and others 1996; Hsieh and others 2000; Dalgard and others 2002; Kabbaj and others 2006; Kee and others 2006; Mammen and others 2012; Nadeem and Aslam 2012; Yan and others 2012). Also, the mean age of patients with TD was similar to those with euthyroidism (43 years) who were younger than patients with TD (50 years) as reported by Kabbaj and others (2006). Pretreatment thyroid hormonal (Mammen and others, 2012) and immune profiles (Kabbaj and others, 2006; Yan and others, 2012) influence development of TD during PEG-IFN+ RIB therapy (Weissel and others, 1995; Abdel-Kader and others, 2012), but in this study, the selected patients had normal thyroid profile and their medical history was negative for thyroid disease.
Meanwhile, thyroid hormonal profile was not correlated with viral load whether before, during, or on follow-up of PEG-IFN+ RIB therapy. It was stated that TD does not correlate with any pretreatment virological parameter; it is probably not related to dose or treatment duration or linked to viral kinetics or virological outcome (Vezali and others 2009), which was contrary to a previous conclusion that the lower HCV RNA levels were significantly associated with TD (Hsieh and others 2000).
In this study, all of the TD patients were clinically free. Many studies reported that most patients with TD were clinically free, for example Dalgard and others (2002) and Yan and others (2012), showed that 85.3% and 70% of TD patients were clinically free respectively, but it was contrary to many others, for example Mekkakia-Benhabib and others (1996), Masood and others (2008), Bini and Mehandru (2004), and Abdel-Kader and others (2012), whose clinically manifested TD patients were more common than subclinical ones (72.2%, 63%, and 58.3%, respectively). None of the patients with hypothyroidism received thyroxin replacement as they had subclinical hypothyroidism. However, in a recent Pakistani study (Mehmood and others, 2015), 70% of the hypothyroid patients and 40% of the hyperthyroid ones needed treatment.
Also, most of TD returned to normal thyroid function in the next follow-up. This was concordant with previous studies, for example Benelhadj and others (1997) and Bini and Mehandru (2004), who found spontaneous recovery soon after treatment or IFN stoppage (Chan and others 2003). Also, it was found that 44.4% of hypothyroid patients and 61.5% of hyperthyroid patients recovered in the study of Mekkakia-Benhabib and others (1996), and only few cases of TD persisted in other studies, that is 2% of TD and 8.7% of hypothyroid patients in Földes and others (2004) and Kee and others 2006), respectively. Debatable results were found regarding the spontaneous resolution of TD after completion of PEG-IFN+ RIB therapy in other studies, for example more than half remitted as reported by Koh and others (1997), while 31.7% remitted in the study of Vezali and others (2009).
Conversely, TD did not negatively influence the completion of PEG-IFN+ RIB therapy, that is none of the patients had to discontinue INF therapy. That was similar to other studies (Bini and Mehandru, 2004; Mehmood and others, 2015), even sustained virological response was higher in patients with TD developed during PEG-IFN+ RIB therapy than those who did not (Dalgard and others 2002; Barut and others 2012), and immune hypothyroidism was associated with higher incidence of HCV remission (Carella and others, 2002). Thus, it was concluded that the PEG-IFN+ RIB therapy can be safely continued for patients with TD who respond well to treatment (Bini and Mehandru 2004), and TD does not contraindicate IFN intake (Chan and others 2003).
Accordingly, TD is a potentially expected side effect in PEG-IFN+ RIB therapy, which requires screening (Benelhadj and others, 1997; Bini and Mehandru 2004) and early detection during treatment (Costelloe and others, 2009) to avoid any hazardous complications (Mandac and others, 2006), provided that standardized testing modalities are crucial to reach the ideal diagnosis (Tran and others, 2013) and identify the true influencing factors (Nair Kesavachandran and others, 2013). The combined IFN-based therapy for HCV (PEG-IFN+ RIB) has declined lately even in the developing countries, including Egypt. Directly acting antiviral drugs were introduced in Egypt by 2014, after starting this study. Even initially, sofosbuvir was given in combination with the combined IFN-based therapy (triple therapy) according to the protocol of the National Committee for Control of Viral Hepatitis. The reported side effects were mainly attributed to IFN. Meanwhile, we have to admit that a limitation of this study is rather the small number of included patients.
Conclusion
TD was an existing side effect related to the PEG-IFN+ RIB therapy, where hypothyroidism was much more common than hyperthyroidism, and mostly remitted spontaneously.
Footnotes
Acknowledgment
We would like to express our gratitude to the medical personnel and information desk of Al-Kahera Al-Fatemeya Hospital for their cooperation and support.
Author Disclosure Statement
No competing financial interests exist.