
Abstract
This meta-analysis examined the relationship between IL-17A (rs2275913) and IL17F (rs763780 T/C) gene polymorphisms and the risk of inflammatory diseases, including periodontitis, rheumatoid arthritis (RA), and inflammatory bowel disease. PubMed, MEDLINE, EMBASE, Web of Science, and Elsevier Science Direct were searched, and odds ratios (ORs) with 95% confidence interval (CI) were calculated to estimate the strength of the association. A total of 25 studies comprising 7,474 cases and 10,628 controls were included. Significant associations were found between inflammatory diseases and IL-17A rs2275913 A versus G allele (OR = 1.197, P = 0.033) and the GA versus GG genotype in the codominant model (OR = 1.406, P = 0.036). Our findings suggested that individuals who carry the rs2275913 A allele or GA genotype have a 20% or 41%-increased risk of inflammatory diseases compared with subjects with the G allele or GG genotype, respectively. With respect to IL-17F rs763780, the C versus T allele (OR = 1.94; P = 0.040), the TC versus TT (OR = 1.39; P = 0.041), the CC versus TT (OR = 2.71; P = 0.003), as well as the TC + CC versus TT genotype (OR = 1.83; P = 0.032) were risk factors for RA. In summary, our pooled analysis indicated that the IL-17A (rs2275913) and IL17F (rs763780 T/C) increased the RA risk.
Introduction
A
Periodontitis is a chronic inflammatory disease that affects the tooth-supporting tissue and destroys the alveolar bone. It is the most frequent cause of tooth loss in adults. Periodontitis has interactions with a number of common human diseases like rheumatoid arthritis (RA). RA is a chronic autoimmune disorder that is characterized by systemic inflammation and continual synovitis that contributes to joint damage (Paradowska-Gorycka and others 2010). Inflammatory bowel disease (IBD) is identified by chronic relapsing inflammation of the gastrointestinal tract, and it comprises two main phenotypes: Crohn's disease and ulcerative colitis (UC) (Zhang and others 2013).
Among the complex network of inflammatory cells, T-helper (Th)-17 cells and their cytokines are related with different autoimmune and inflammatory diseases, including periodontitis, RA, and IBD (Kerami and others 2014). One of the main features of the Th17 subset is the production of interleukin (IL)-17 (Bogunia-Kubik and others 2015). IL-17 is a newly described cytokine that connects the adaptive and innate immune systems. It is not only involved in neutrophil proliferation, maturation, and chemotaxis but also stimulates T cells and induces the maturation of dendritic cells (Kellner 2013; Senhaji and others 2016).
IL-17 is a proinflammatory cytokine that is produced by activated T cells (Zacarias and others 2015) and includes six similar members, IL-17A, IL-17B, IL-17C, IL-17D, IL-17E, and IL-17F, based on the order in which they were discovered. IL-17A is the most homologous to IL-17F, and the genes encoding them are closely located on chromosome 6p12 [15]. Many studies have demonstrated the presence of IL-17 in periodontal tissues, crevicular gingival fluid, saliva, and plasma of patients with periodontal disease (Zacarias and others 2015), synovial membrane and synovial fluid of RA patients (Kellner 2013; Benedetti and Miossec 2014), and serum of IBD patients (Liu and others 2016).
Polymorphisms in cytokine genes that could potentially affect expression and or biological activity would be of particular interest. Polymorphisms in the IL-17A and IL-17F genes have been reported to be associated with different inflammatory diseases in various populations (Zhang and others 2013; Senhaji and others 2016). The IL-17A G197A (rs2275913) and IL-17F T7488C (His161Arg, rs763780) are two putative single nucleotide polymorphism (SNP) loci in the IL-17 genes, which could influence the transcriptional regulation of IL-17. These two SNPs have been analyzed for their association with the occurrence of inflammatory diseases, including RA, IBD, or periodontitis in different populations (Abhimanyu and others 2013; Tiwari and others 2014; Bulat-Kardum and others 2015). However, the findings were somewhat conflicting, which could be caused by the relatively small sample size of individual studies.
Meta-analysis is a statistical system for assembling results from different studies to produce a single approximate of the major effect with enhanced precision (Wei and others 2015). Therefore, the present study was aimed at pooling the data available and investigating whether IL-17A (rs2275913) and IL-17F (rs763780) gene polymorphisms are associated with the susceptibility to different inflammatory diseases, including periodontitis, RA, and IBD.
Materials and Methods
Literature search
We executed the literature search by using the electronic databases PubMed, EMBASE, and MEDICINE. All languages were searched, and inclusive search strategies included the Mesh term and Keywords: (“Interleukin-17A” or “Interleukin17A” or “Interleukin-17F” or “Interleukin17F” or “IL-17A” or “IL17A,” or “IL-17F” or “IL17F”), (“polymorphism” or “variant” or “genotype,” “SNP” or “mutations”), (Rheumatoid arthritis or RA, Periodontitis and Inflammatory bowel disease or IBD) through June 5, 2016. Eligible studies were retrieved and evaluated cautiously. Review articles and bibliographies of other pertinent studies found were hand-searched to find further qualified studies. This meta-analysis was conducted in accordance with the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines [31] and by following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [32].
Data collection
The articles were filtered by two independent reviewers (E.E.N., M.M.) to assess the appropriateness of the articles selected by using a standardized protocol and data collection form. Studies were included if they met all of the following criteria: (a) original data; (b) study that assessed the association of IL-17A rs2275913 or IL-17F rs763780 and the susceptibility to inflammatory diseases, including RA, Periodontitis, and IBD; and (c) comparison between patients with RA, Periodontitis, and IBD and controls. Exclusion criteria were (a) nonhuman studies, abstracts only, comments, reviews, editorials or letters, mechanism studies, and studies missing controls; (b) family-based design or sibling pair studies; (c) studies with lack of enough information for data extraction; and (d) unpublished articles.
We collected the following data information from each study: authors, publication date, country, ethnicity, sample size, allele and genotype frequency distribution, and Hardy–Weinberg equilibrium. Differences about inclusion of studies and description of data were resolved by conversation.
Statistical analyses
Quantitative meta-analysis was utilized by RevMan version 5.3 and STATA, version 11.0 (StataCorp., College Station, TX) (Eskandari-Nasab and others 2015). Crude ORs with 95% CIs were used to measure the strength of association between the IL-17A rs2275913 or IL-17F rs763780 and the risk for RA, Periodontitis, or IBD. The significance of the pooled OR was identified by the Z-test, and P < 0.05 was selected as statistically significant.
The pooled ORs for the IL-17A rs2275913 G/A polymorphism and the risk for RA, Periodontitis, or IBD were performed for the codominant model (GA versus GG and AA versus GG), the dominant model (GA + AA versus GG), the recessive model (GA + GG versus AA), and for the allelic contrast (A versus G). The pooled ORs for the IL-17F rs763780 T/C polymorphism and the risk for RA, Periodontitis, or IBD were performed by using the same models. Forest-plots graphs were presented to assess the overall association between the IL-17A rs2275913 or IL-17F rs763780 and the risk for RA, Periodontitis, or IBD. Heterogeneity among studies was calculated by Cochrane's Q-test and I2 assessment, which was defined as the ratio of overall variation that existed among study variants. A P-value less than 0.10 and an I2 value higher than 50% showed significant heterogeneity. A random-effect model was used in the occurrence of significant heterogeneity; if not, a fixed-effect model was executed. Begger's test and Egger's linear regression analysis were applied for publication bias, and a P-value less than 0.10 was indicative of the presence of a publication bias. Sensitivity analysis was performed to examine the precision and consistency of the primary meta-analysis, to verify the effects associated with any individual study.
Results
Study characteristics
In the current meta-analysis, a total of 25 studies, including 7,474 cases and 10,628 controls, satisfied the inclusion criteria for both IL-17A and IL-17F SNPs in RA, periodontitis, or IBD. Fifteen studies examined the association between IL-17A rs2275913 G/A variation and the risk for inflammatory diseases, of which six studies were on RA, five studies were on periodontitis, and four studies were performed on patients with IBD. As for IL-17F rs763780 T/C, 10 studies assessed the association between this polymorphism and the risk for inflammatory diseases, of which four studies were on RA, four other studies were on periodontitis, and two studies were on IBD. Baseline characteristics of the included studies on IL-17A and IL-17F SNPs on inflammatory diseases are shown in Table 1 and 2, respectively.
AP, aggressive periodontitis; CD, Crohn's disease; CP, chronic periodontitis; GCA, Giant cell arteritis; HWE, Hardy–Weinberg equilibrium; OA, osteoarthritis; RA, rheumatoid arthritis; SS, Sjögren's syndrome; T1DM, diabetes mellitus type 1; UC, ulcerative colitis.
AP, aggressive periodontitis; GAgP, generalized aggressive periodontitis; UC, ulcerative colitis.
IL-17A rs2275913 G/A polymorphism and inflammatory diseases
Fifteen studies consisting of 4,831 patients and 7,652 controls examined the relationship between IL-17A rs2275913 G/A polymorphism and susceptibility to inflammatory diseases. Table 3 indicates the pooled analysis of associations between IL-17A rs2275913 G/A polymorphism and risk of inflammatory diseases by using codominant, dominant, and recessive models. The results of meta-analysis demonstrated that the A versus G allele was associated with a higher risk of inflammatory diseases with the overall OR of 1.197 (P = 0.033; 95% CI = 1.015–1.412). Using the codominant model, the results indicated that GA versus GG genotype distribution between groups was different and the association was statistically significant (P = 0.036, OR = 1.406, 95% CI = 1.023–1.931).
Boldface indicates the significance level is 0.05.
No., number of studies; OR, odds ratio.
However, the overall disparity between groups for the AA versus GG and GA + AA versus GG genotype as well as that of the GA + GG versus AA were not associated with the risk of inflammatory diseases (P > 0.05). Figure 1 demonstrates the forest plot of the risk of inflammatory diseases related with IL-17A rs2275913 G/A polymorphism.
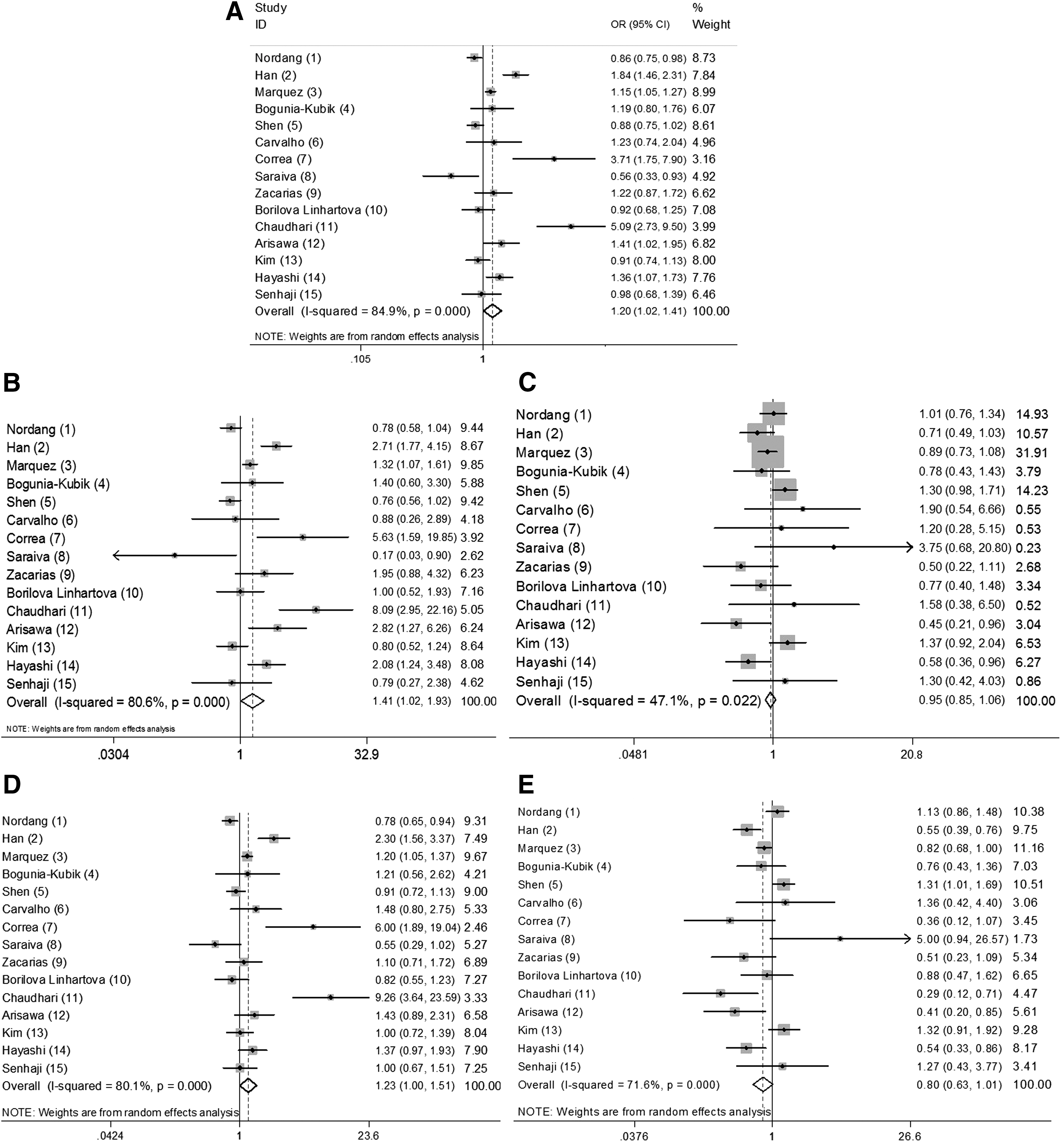
Forest plot of the risk of inflammatory diseases associated with IL-17A rs2275913 G/A polymorphism
IL-17A rs2275913 G/A polymorphism and RA
There were six case–control studies, with 3,267 cases and 5,928 controls, that described the association between IL-17A rs2275913 G/A polymorphism and susceptibility to RA. Table 3 indicates the pooled analysis relationship between IL-17A rs2275913 G/A polymorphism and risk of RA by using codominant, dominant, and recessive models. Our meta-analysis showed that none of the IL-17A rs2275913 comparisons were associated with the risk of RA under codominant, dominant, and recessive models (P > 0.05).
IL-17A rs2275913 G/A and periodontitis
Five studies, including 600 patients with periodontitis and 454 controls, evaluated the association between IL-17A rs2275913 G/A polymorphism and susceptibility to periodontitis. As shown in Table 3, there were no significant associations between IL-17A rs2275913 G/A polymorphism and the risk for periodontitis by using codominant, dominant, and recessive models as well as allele comparison (P > 0.05).
IL-17A rs2275913 G/A polymorphism and IBD
Four studies with 964 patients with IBD and 1,270 controls examined the relationship between IL-17A rs2275913 G/A variation and susceptibility to IBD. Our pooled evidence showed that none of the IL-17A rs2275913 comparisons were associated with the risk of IBD under codominant, dominant, and recessive models (P > 0.05).
IL-17F rs763780 T/C variation and inflammatory diseases
The associations between the 17F rs763780 T/C and inflammatory diseases were investigated in eight case–control studies with 2,643 cases and 2,976 controls. As demonstrated in Table 4, the pooled evidence showed that the prevalence of CC genotype versus TT was different in cases and controls, although the difference was not statistically significant (P = 0.071; OR = 1.466; 95% CI = 0.968–2.244).
Boldface indicates the significance level is 0.05.
IL-17F rs763780 T/C variation and RA
There were four case–control studies that described the association between IL-17A rs2275913 G/A and RA, which included 600 cases and 454 controls. Our pooled evidence showed that the C allele versus T (P = 0.040), the TC genotype versus TT (P = 0.041), the CC genotype versus TT (P = 0.003), as well as the TC + CC versus TT (P = 0.032) were associated with an increased risk of RA as demonstrated in Figure 2. The summary ORs for the C allele (OR = 1.936; 95% CI = 1.028–3.645) and TC + CC versus TT genotype (OR = 1.833; 95% CI = 1.052–3.193) were estimated by the random model due to the high heterogeneity, but the OR of 1.398 and 2.712 for the TC and CC genotypes was calculated by using the fixed-effect model.
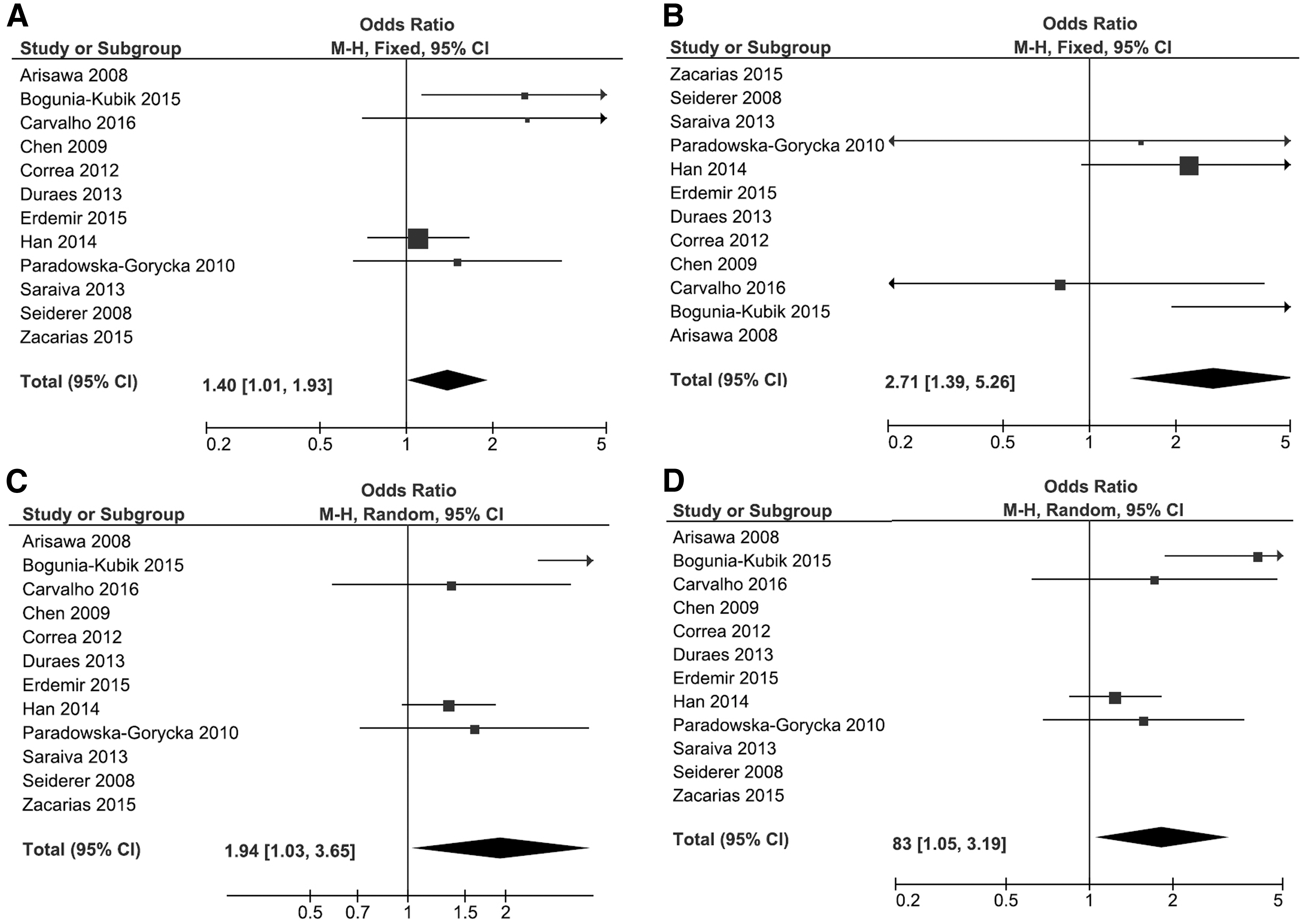
Forest plot of the risk of rheumatoid arthritis associated with IL-17F rs763780 T/C polymorphism
IL-17F rs763780 T/C variation and periodontitis
Four studies comprising 26 cases and 351 controls evaluated the relationship between IL-17F rs763780 T/C and periodontitis. Pooling of the data demonstrated no significant association, using any of the three models suggesting that the rs763780 polymorphism was not associated with periodontitis development (P > 0.05).
IL-17F rs763780 T/C variation and IBD
Four case–control studies consisting of 1,617 cases and 2,171 controls evaluated the association between rs763780 T/C and susceptibility to IBD. We observed no association between this variation and the risk for IBD by using any of the three models (P > 0.05).
Heterogeneity and sensitivity analyses
We found significant heterogeneities in the information of IL-17A rs2275913 and IL-17F rs763780 variations (Table 3). Because of major heterogeneity across studies, individual studies included in the meta-analysis were omitted consecutively to find the source by sensitivity analysis. The findings indicated that no individual study influenced the overall OR values for rs2275913 and rs763780 variations.
Evaluation of publication bias
As shown in Tables 3 and 4, both Begg's and Egger's test were done to assess the publication bias. Egger's linear regression test showed a moderate publication bias for the IL-17F rs763780 C/T in the codominant model (TC versus TT) in both inflammatory disease (P = 0.045) and periodontitis groups (P = 0.010); however, no evidence of publication bias was found for any other genetic models in all groups as shown in detail in Tables 3 and 4.
Discussion
In the current meta-analysis, we retrieved 25 studies (7,474 cases and 10,628 controls) to evaluate the association of IL-17 A and F gene polymorphisms with autoimmune and inflammatory diseases. Our results provide evidence of strong associations between IL17A rs2275913 G/A and IL17F rs763780 T/C gene polymorphisms and susceptibility to inflammatory diseases. As far as we know, this is the first meta-analysis carried out so far that is aimed at investigating the relationship between IL17A and F gene polymorphisms and inflammatory diseases.
The IL17A rs2275913 G/A was associated with an increased risk of inflammatory diseases at both allelic (A versus G) and genotypic (GA versus GG) levels. Our findings suggested that individuals who carry the rs2275913 A allele or GA genotype have 20% or 41%-increased risk of inflammatory diseases compared with subjects with the G allele or GG genotype, respectively. However, this SNP was not associated with the risk of RA, periodontitis, or IBD. In contrast to our findings, Correa and others (2012) indicated that the rs2275913 AA and GA genotypes increased the risk of CP with OR of 3. Likewise, Zacarias and others (2015) have shown that rs2275913 AA genotype, and the A allele were associated with a susceptibility to CP in a Brazilian population, but they found no associations for IL17F rs763780 T/C and CP in their population, which supports our pooled evidence.
With respect to IL-17F, the rs763780 C/T polymorphism was associated with increased predisposition to RA at both allelic and genotypic levels but it was not associated with periodontitis or IBD. The C allele, TC, and CC genotypes in the codominant model as well as the TC + CC genotype in the dominant model were risk factors for RA with the ORs of 1.9, 1.4, 2.7, and 1.8, respectively. According to our pooled evidence, the carriers of rs763780 C allele, TC, CC, or TC + CC genotypes had 94%, 40%, 170%, and 83% higher risks of developing RA than subjects with the T allele or TT genotype, respectively. Our results for rs763780 support the findings of Bogunia-Kubik and others (2015), who have shown that rs763780 C allele as well as CC genotype were more common among RA patients than healthy individuals, and both were risk factors for RA in a Polish population. Paradowska-Gorycka and others (2010) indicated that the IL-17F rs763780 C variant was associated with parameters of RA severity, such as number of tender joints, but they did not find any relationship between rs763780 and RA risk. In contrast to our findings, the studies of Seiderer and others (2008), Arisawa and others (2008), and Chen and others (2009) have confirmed a correlation between IBD and IL-17F rs763780 T/C gene variation. Arisawa and others (2008) reported that variant alleles of rs763780 or rs2275913 variations may influence the susceptibility to and pathophysiological features of UC. They found that rs763780 wild-type TT genotype was significantly higher in UC patients compared with control subjects, and that both polymorphisms were significantly associated with the pancolitis phenotype. Chen and others (2009) observed that the homozygous polymorphic (CC) genotype was lower in UC patients than in healthy subjects and that carriers of rare allele C had a higher incidence of getting mild severity than a carrier of common allele T (Paradowska-Gorycka and others 2010).
The rs2275913 polymorphism in the promoter region of cytokines may be related to higher expression of the IL-17A. Espinoza and others (2011) have shown that the IL17A 197A allele correlates to more efficient IL-17 production and higher affinity for the nuclear factor of activated T cells (NFAT). This polymorphism is positioned in close vicinity to two binding motifs for the NFAT, which is a vital controller of the IL-17 promoter. Therefore, it is plausible that the rs2275913 variation affects the transcriptional regulation of IL-17A. IL-17F, another essential member of the IL-17 family, contributes to neutrophil recruitment and activation through stimulation of the production of cytokines and chemokines. IL-17F rs763780 (His121Arg) polymorphism has been shown to suppress the expression and the activity of IL-17F and, therefore, plays a role in diversities in the host's predisposition to inflammatory diseases (Zacarias and others 2015).
Growing proof showed that IL-17A and IL-17F have key functions in the development of many autoimmune and inflammatory diseases, such as RA (Biswas and others 2012), systemic lupus erythematosus (Garrett-Sinha and others 2008), asthma (Song and others 2008), and IBD (Fitzpatrick 2013; Bogunia-Kubik and others 2015). IL-17 overexpression has been associated with inflammation and autoimmune disorders. IL-17 stimulates the production and expression of TNF-alpha and IL-1 beta by human macrophages. Thus, IL-17 contributes to inflammatory bone pathology as in RA and IBD and is involved in several inflammatory and autoimmune disorders (Zacarias and others 2015).
There are several limitations of the current meta-analysis. First, significant relationships were identified between the two genetic variations and the risk of inflammatory diseases in different genetic models, but various possible causes of heterogeneity, including origin of controls, lifestyle, and environmental exposures, were not examined. Inflammatory diseases themselves are heterogeneous, and may result in the heterogeneity. Second, the study information included in this meta-analysis was on the basis of unadjusted analyses, and, thus, we were unable to determine the risk of inflammatory diseases by considering environmental elements, age, family background, lifestyle, or additional risk factors that could have possible effects on pooled results. Third, for the subgroup analysis of ethnicity, the number of each subgroup was very small, and it lacked enough statistical power to explore the real association. Forth, our meta-analysis only included the published literatures, taking into account some pertinent important but unpublished studies. Therefore, despite this limitation, our meta-analysis is valuable to be interpreted with caution.
In conclusion, our study provides an inclusive meta-analysis of the function of IL-17A rs2275913 and IL-17F rs763780 genetic variations in inflammatory diseases risk. The results indicated that these two genetic variations of IL-17A and IL-17F were risk factors for inflammatory diseases, particularly RA. More larger and multicenter researches are needed to verify the prediagnostic influences of IL-17 gene polymorphisms on the risk of inflammatory diseases.
Footnotes
Acknowledgments
E.E.N. and M.M. were responsible for data extraction, A.T. analyzed the data, and E.E.N. wrote the article.
Author Disclosure Statement
No competing financial interests exist.