
Abstract
Ribavirin clearly plays a role in chronic hepatitis C treatment response. The equilibrative nucleoside transporter-1 codified by SLC29A1 gene has been associated with ribavirin uptake into hepatocytes and erythrocytes. rs760370A>G single nucleotide polymorphism (SNP) at the SLC29A1 gene may have a role in ribavirin-based regimen treatment response. Accuracy of the polymerase-chain reaction-restriction fragment length polymorphism (PCR-RFLP) assay compared with the TaqMan assay for the detection of the SNP rs760370 at the main ribavirin transporter gene and its relation to sustained virological response in chronic hepatitis C virus (HCV) patients treated with pegylated interferon–ribavirin therapy. The study included 100 chronic HCV patients who were treated with pegylated interferon–ribavirin therapy. The patients were categorized according to the treatment response into responders (50 patients) and null responders (50 patients). rs760370 SNP was measured using TaqMan 5-nuclease assay and by the newly developed PCR-based RFLP assay. The overall accuracy of the newly developed PCR-RFLP assay compared with the TaqMan assay for rs760370 polymorphism detection was 100%. Allelic frequencies at rs760370 were as follows: A/A genotype (28%), A/G genotype (58%), and G/G genotype (14%). Treatment response was not significantly related with rs760370 polymorphism (P = 0.5). Ribavirin-induced anemia was good predictor of sustained virological response (P = 0.001), but was not related to rs760370 polymorphism (P = 0.92). PCR-RFLP assay is an accurate, cost-effective method in the detection of rs760370 compared with TaqMan assay. rs760370 SNP cannot serve as predictor of response in chronic HCV patients treated with interferon ribavirin therapy.
Introduction
R
The molecular mechanisms by which ribavirin enhances response rates during antiviral HCV therapy are still unknown. Several mechanisms of action have been proposed, including (1) immunomodulatory properties, (2) inhibition of inosine monophosphate dehydrogenase (IMPDH) with depletion of pools of guanosine triphosphate, an essential substrate for viral RNA synthesis, (3) direct inhibition of the HCV-encoded NS5B RNA polymerase, and (4) induction of lethal mutagenesis (Chung and others 2008; Hofmann and others 2008).
Ribavirin is transported within the cells by nucleoside transporters that have been classified into 2 families; (1) The equilibrative nucleoside transporters (ENTs) 1 to 4, codified by the solute carrier SLC29A 1 to 4 genes and (2) The concentrative nucleoside transporters (CNT) 1 to 3, codified by the SLC28A 1 to 3 genes (Kong and others 2004; Owen and others 2005; Bengsch and Thimme 2010). In hepatocytes (Govindarajan and others 2008) and erythrocytes (Jarvis and others 1998), which are the 2 main cellular compartments for ribavirin accumulation, ribavirin is primarily transported by ENT1.
Morello and others (2010) examined whether specific single nucleotide polymorphisms (SNPs) at the SLC29A1 gene could affect the hepatic expression or function of ENT1, influencing ribavirin intracellular exposure and potentially its antiviral activity against HCV in HIV patients coinfected with HCV.
The TaqMan and direct-sequencing assays have been previously utilized for the determination of rs760370 genotypes. However, these methods are much more expensive compared to polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) assay. PCR-RFLP assay would markedly minimize the cost of testing for rs760370 SLC29A1 gene polymorphism by more than 5 times, helping for more expanded future studies, especially in low resources and less developed countries (Hui and others 2008).
Objectives
We investigated the accuracy of the PCR-RFLP assay compared with the TaqMan assay for the detection of the single nucleotide rs760370 polymorphism at the main ribavirin transporter gene. Also, we studied the relation of SNP rs760370 polymorphism and sustained virological response in chronic HCV patients treated with pegylated interferon ribavirin therapy.
Materials and Methods
A cohort study included 100 Egyptian patients with chronic HCV infection treated with pegylated interferon and ribavirin therapy were recruited from National Liver Institute and Cairo Fatymic hospital specialized centers for treatment of chronic HCV.
Patients were divided into 2 groups according to response to treatment; group 1: 50 patients null responder (failure to achieve early virological response as decrease by 2 log10 IU/mL HCV RNA level from baseline at 12 weeks of therapy) and group 2: 50 patients who achieved sustained virological response (negative PCR at the end of treatment and after 24 weeks of treatment).
Review of patients' medical records, including their baseline laboratory investigations (complete blood count [CBC], serum transaminases, alpha feto protein [AFP], thyroid stimulating hormone [TSH], and HCV PCR quantitative) and liver biopsy using METAVIR scoring (Bedossa and Poynard 1996). Follow-up of 12 weeks of laboratory tests, including CBC and serum transaminases, were monitored. Serum HCV-RNA levels were measured at baseline, at weeks 12, 24, and 48 of therapy, as well as at week 24 following the completion of treatment to confirm the treatment response.
Peripheral venous blood samples were coded and rs760370 SNP genotypic cross-sectional analysis was done using rs760370 TaqMan assay and the newly designed PCR-RFLP assay specific for the rs760370.
Genotyping for rs760370 was performed using Custom TaqMan SNP Genotyping Assay (Applied Biosystems, Foster City, CA), in which a fluorogenic probe, consisting of an oligonucleotide labeled with both a fluorescent reporter dye (carboxyfluorescein [FAM] or VIC fluorescent dye) and a quencher dye, is included in a typical PCR. Amplification of the probe-specific product causes cleavage of the probe, generating an increase in reporter fluorescence. The primer and probe set were used in the TaqMan SNP Genotyping Assays (ID: C_2334579_10; Applied Biosystems) in accordance with the information on the Applied Biosystems website (
SLC29A1 nucleotide sequence was extracted from NCBI gene database, then targeting primers were designed using Primer 3 (

TGCA targeted restriction enzyme sequence.
PCR amplification was performed in a total volume of 10 μL containing 10 mM Tris-HCl (pH 8.3), 50 mM KCl, Tween-20 0.01%, 0.2 mM deoxyribonucleotides, 24 pmol of each primer (forward primer 5′-TGGGGGACACTCAGTAGAGG-3′ and reverse primer 5′-CCTCCTTGAGGGAACGTGTA-3′), 2.0 mM MgCl2, and 0.5 U Hot-Start Taq DNA polymerase.
At the first PCR cycling step, denaturation at 95°C for 5 min was performed. This was followed by 35 cycles of 95°C for 60 s, 58°C for 60 s, and 72°C for 45 s; finally 72°C for 7 min, using Biometra T3000 thermocycler. Restriction with HpyCH4V (New England BioLabs, Beverly, MA; stored at −20°C) was performed using a reaction containing 1 μL of PCR product, 5 μL (1 × ) of 10 × HpyCH4V buffer, 1 μL (1 U) of HpyCH4V, and 43 μL of nuclease-free water for a minimum of 1 h at 37°C. Restriction products were detected by electrophoresis on a 4% agarose gel after staining with ethidium bromide.
Patients consent
The protocol of the study was approved by the Ethics Committees of the National Committee for Control of Viral Hepatitis (NCCVH) and the National Research Center of Egypt. Patients' informed written consent from each patient and local ethical committee approval were available before starting data collection. With respect to patients' confidentiality, patients were represented in the study by code numbers and not by their names with all personal data concealed. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Statistical analyses
All results were expressed in absolute values and percentages in the case of categorical variables, and quantitative variables were compared using unpaired Student's t-test and ANOVA, in addition to Mann–Whitney test, and Kruskal–Wallis H tests for nonparametric data. All statistical analyses were performed using the SPSS software package (version 13.0; SPSS, Inc.) and significant differences were considered only for P < 0.05.
Results
Detection of rs760370 polymorphism by PCR-RFLP assay compared with the TaqMan assay
A 202-bp product was successfully amplified from the randomly selected samples using the newly designed forward primer 5′-TGGGGGACACTCAGTAGAGG-3′ and the reverse primer 5′-CCTCCTTGAGGGAACGTGTA-3′. The digested fragments using HpyCH4V restriction enzyme were as follows; 1 “202 bp” band for the G allele, and 2 “154 + 48 bp” bands for the A allele, while the AG genotype having 3 bands “202 + 154 + 48 bp amplicon,” as shown in Fig. 2.
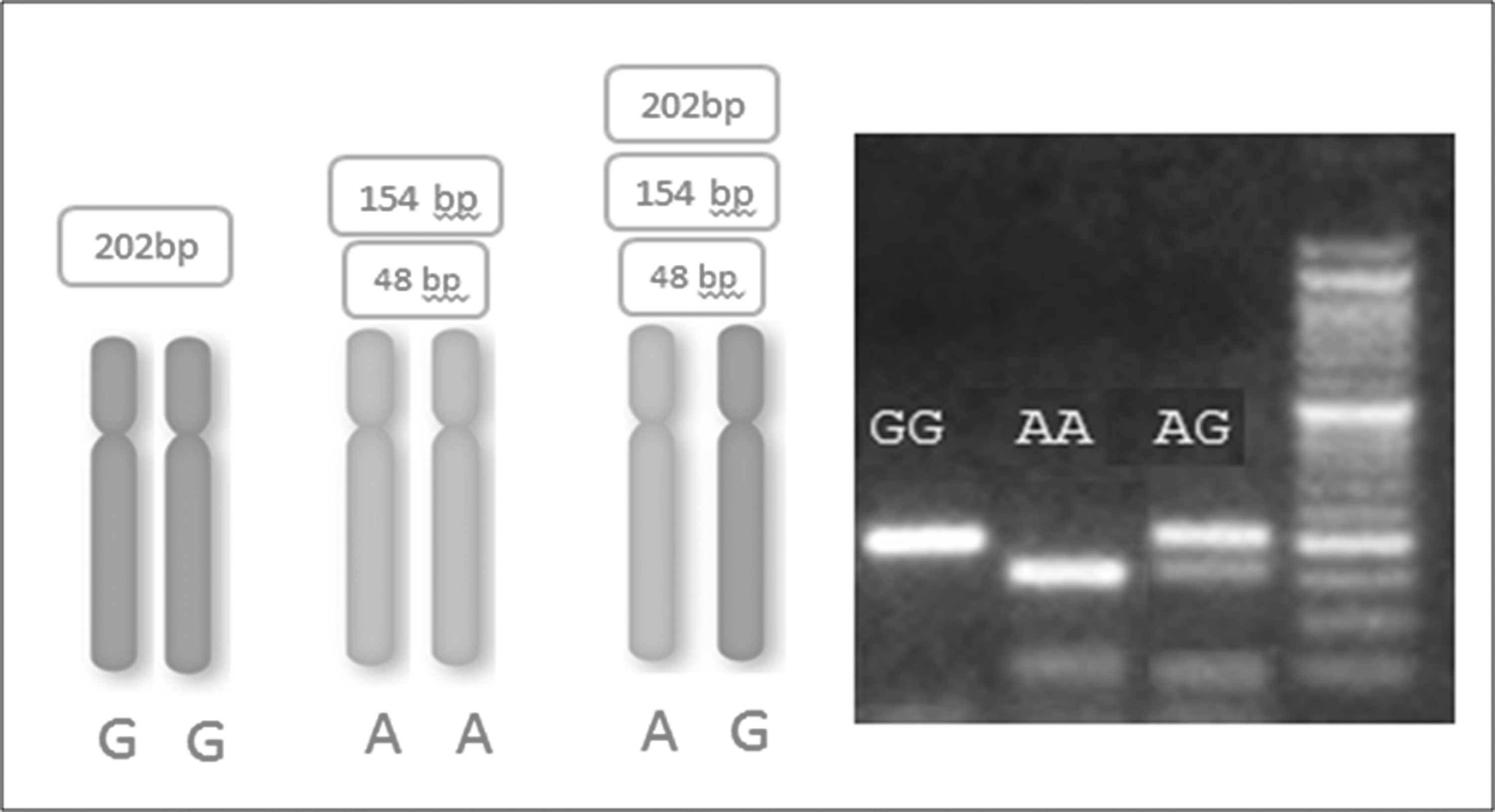
Gel electrophoresis of SLC29A1 202 bp amplicon digested with HpyCH4V restriction enzyme.
When tested the samples that have been analyzed using TaqMan assay, similar results were obtained using the newly designed PCR-RFLP assay targeting SLC29A rs760370 SNP genotyping with 100% accuracy.
Comparison between baseline characteristics and rs760370 polymorphism of the studied patients and groups
The baseline characteristics of the 100 patients studied are summarized in Table 1. No statistical significant difference was observed between the non-responders (NR) group and the SVR group concerning the age (P = 0.466), gender (P = 0.63), and body mass index (P = 0.934).
Bold indicates statistically significant value.
AFP, alpha feto protein; ALT, alanine transaminase; BMI, body mass index; HCV, hepatitis C virus; TSH, thyroid stimulating hormone; WBC, white blood cell.
Concerning the laboratory data, only the baseline platelet count was significantly related to the treatment response, as low baseline platelet count (<130 × 103/mm3) was significantly higher in the NR group (P = 0.026). Otherwise, however, no statistical difference was observed between the 2 groups concerning hemoglobin level (P = 0.641) and white blood cell count (P = 0.166), alanine transaminase (ALT) level (P = 0.133), AFP level (P = 0.34), TSH level (P = 0.24), and basal HCV-RNA load (P = 0.748).
Regarding the liver biopsy, the histopathological activity score was related to the response rate as the percentage of A2 and A3 were statistically higher in the NR group compared with the SVR group with P-value of 0.04, while no statistical significant difference was observed concerning the basal fibrosis score (P = 0.12) between the 2 groups.
The association between baseline ALT level and basal activity score was tested and yielded a statistical significant association between baseline ALT level and basal activity score (P = 0.011), with a median of 43 U/L among the A1 group, 74 U/L among the A2, and 107 U/L among the A3 group.
Among the studied patients, 58 patients were of A/G genotype (58%), 28 patients (28%) had A/A genotype, and 14 patients (14%) had G/G genotype. Overall, allelic frequency among our HCV patients was 57% for A nucleotide and 43% for G nucleotide.
Among the NR patients, 30 patients were of A/G genotype (60%), 15 patients (30%) had A/A genotype, and 5 patients (10%) had G/G genotype. Among the SVR patients, 28 patients were of A/G genotype (56%), 13 patients (26%) had A/A genotype, and 9 patients (18%) had G/G genotype, with no statistical difference between the NR and SVR groups (0.5) even when categorized into G/G and non-G/G groups (P = 0.25).
The baseline characteristics of the studied patients were compared with the different rs760370 genotypes as categorized into AA, GG, and AG. No statistical significant difference was observed between the 3 genotypes and the baseline characteristics as summarized in Table 2.
Comparison between rs760370 polymorphism and the 12-week follow-up of the studied patients and groups
Hemoglobin reduction below 10 g/dL or 2 g drop from the baseline was reported in 13 patients after 12 weeks of treatment. Hemoglobin drop was significantly related to SVR (P = 0.001) as anemia was reported in only 1 case of the NR group compared with 12 patients in the SVR group as presented in Table 3.
Bold indicates statistically significant value.
Although no statistical difference was observed between the 2 groups regarding the platelet count levels (P = 0.673), there was statistical significant drop from the baseline platelets count till 12 weeks of therapy of 11 × 103/mm3 in the NR group compared with 43 × 103/mm3 among the SVR group with P-value 0.006.
Also, a statistical difference was observed as well (P = 0.002) concerning the ALT level at 12th week of therapy with a median of 46 U/L among the NR group and median of 31 U/L among the SVR group.
As anemia is related to the ribavirin and ribavirin dose reduction, we studied the impact of SLC29A1 gene rs760370 polymorphism in patients who developed and did not develop significant hemoglobin drop from the baseline levels. There was no statistical significant difference between the rs760370 polymorphism genotypes (AA, AG, and GG) and the hemoglobin drop (P = 0.92). Also, no significant difference was found between the 3 genotypes rs760370 polymorphism and hemoglobin drop in responder patients (SVR group) with P-value of 0.9 as presented in Table 4.
SVR, sustained virological response.
Discussion
Even with the development of DAAs-based therapy, ribavirin remains an important player in the treatment protocols, especially in cirrhotic and treatment-experienced patients. It appears that ribavirin will continue to be required to suppress the emergence of viral resistance to DAAs in interferon (IFN)-free regimens until more potent agents and oral combinations can be found (González-Moreno and others 2013). In addition, within the era of cost containment, ribavirin (RBV) will probably continue to be part of combination therapy in resource-poor settings despite the lack of understanding of its mechanism of action in chronic HCV infection (Koh and Liang 2014).
Several studies testing for host genetic determinants that may explain an association among ribavirin dosage, serum concentration, ribavirin-induced anemia, and sustained virological response are still conflicted (Owen and others 2005; Doehring and others 2011; Rau and others 2013).
Several studies have shown a definite relationship between RBV plasma/serum concentration and SVR in patients treated with pegylated interferon and ribavirin therapy. Higher level of RBV increases the chance of achieving SVR, at the cost of hematological side effects (Arase and others 2005).
In the current study, we investigated the relation of SNP rs760370 polymorphism at the main ribavirin transporter gene and SVR in chronic HCV patients treated with pegylated interferon–ribavirin therapy; as well as the accuracy of the PCR-RFLP assay compared with the TaqMan assay for the detection of the single nucleotide rs760370 polymorphism at the main ribavirin transporter gene.
Good genotyping data can usually be obtained using TaqMan® assay in a short time using a small amount of genomic DNA, and many samples can be processed simultaneously. The TaqMan and direct-sequencing assays have been previously utilized for the determination of rs760370 genotypes (Hui and others 2008). However, their costs are limiting more extended research in low-resources laboratories and less-developed countries.
We successfully genotyped the rs760370 SNP PCR-based RFLP assay, using the newly designed forward primer 5′-TGGGGGACACTCAGTAGAGG-3′ and the reverse primer 5′-CCTCCTTGAGGGAACGTGTA-3′ with the aid of HpyCH4V restriction endonuclease. PCR-RFLP for the detection of rs760370 A>G SNP was very accurate, cost effective, and convenient. We believe that this technique would markedly minimize the cost of testing for rs760370 SLC29A1 gene polymorphism, helping for the future studies in low-resources laboratories.
In our study, there was no significant association between rs760370 genotypes and the treatment response (SVR) to pegylated interferon and ribavirin therapy. Also, there were no relation between the baseline characteristics of the studied patients and patient groups and the rs760370 genotypes expression. Thus, the rs760370 could not be used as a predictor of treatment response. This is in line with Milazzo and others in 2015 study that demonstrated no association between rs760370A/G polymorphism and the RVR to pegylated interferon–ribavirin–telaprevir therapy (Milazzo and others 2015).
In contrary to our results, Morello and others in 2010 study demonstrated that only rs760370A>G exhibited significant association with the achievement of rapid virological response to pegylated IFNα and ribavirin therapy (50% vs. 17%, in GG carriers and AA/AG carriers, respectively) (Morello and others 2010). Also, Galtieri and others in 2013 denoted that RVR and SVR were more frequent among GG carriers than in AA/AG (66% vs. 27% and 66% vs. 32%, respectively; P = 0.02 and P = 0.04) in 32 HCV recurrence postliver transplantation patients (Galtieri and others 2013).
The contradictory in the results may be attributed to the sample size, different genotypes, as well as the characteristics of the studied patients. These finding have important implications, as they open additional questions on the role of host genetic factors in the modulation of serum ribavirin levels and response to HCV therapy.
While analyzing the demographic and baseline laboratory data of the studied groups, the low platelets count (<130 × 103/mm3) and the high histopathological activity (A2 and A3) were significantly associated with the failure of response. The significant lower SVR in patients with baseline platelet counts below 130 × 103/mm3 likely reflects the fact that patients with low platelet counts are more prone to being cirrhotic and therefore may have a lower response rate to therapy (Kanda and others 2013).
Significant association between baseline ALT level and basal activity score was demonstrated in our study (P = 0.011), also, the on-treatment ALT level (after 12 weeks of treatment) was significantly lower in the SVR group than the NR group reaching earlier normalization of the ALT level.
Our results agree with previous studies, which reported that the rapid normalization of serum ALT level after initiation of treatment may play an additional role in predicting SVR (Kronenberger and others 2007; Dogan and others 2013). In general, a decreased pattern of ALT level is the accepted basic indicator of interferon therapeutic effect, and several studies have shown that delayed normalization of ALT levels may indicate poor response to interferon therapy (Rauch and others 2010).
The mechanism of decline of ALT level is not clear; however, it can be explained by a reduction in infected cells, a noncytolytic cure, or cell removal irrelevant of ALT dynamics. However, a decreased ALT level at the early phase of treatment is not related to apoptotic activity. Theoretically, the rapid declines in ALT may reflect a rapid decrease of ongoing inflammation in the same manner as removal of the virus ((Kronenberger and others 2007; Dogan and others 2013).
Different studies were published assessing new SNPs that may affect ribavirin response and side effects, especially ribavirin-induced anemia, and may explain the significant association between anemia and SVR (Doehring and others 2011; Hitomi and others 2011; Domingo and others 2012; Galtieri and others 2013; Rau and others 2013).
We also did not find significant association between rs760370 SNP at the SLC29A1 gene and ribavirin-induced anemia. However, we demonstrated a significant association between SVR and ribavirin-induced anemia within the first 12 weeks of therapy (P = 0.001), which supports the theory concerning hemoglobin decline as a pharmacodynamic marker of RBV exposure and response to therapy. These data suggest that the extent of Hb decline could be a pharmacodynamic marker of RBV exposure, which may predict its antiviral effect more precisely than the RBV dose (Rau and others 2013).
We summarize that PCR-based RFLP assay is an accurate, cost-effective technique for detecting SNPs polymorphism. The rs760370 SNP is not a helpful predictor of response in chronic HCV patients treated with ribavirin-based therapy. Further large-scale studies of the host genetic determinants such as SLC28A2 SNPs, SLC28A3 SNPs, and inosine triphosphatase (ITPA) SNPs combined with rs760370 clarifying the confirmed association of ENTs with virological response are needed for better understanding of ribavirin kinetics and mechanism of action and guiding for eligibility to antiviral therapy, especially with the newly available DAAs with ribavirin.
Footnotes
Author Disclosure Statement
No competing financial interests exist.