
Abstract
Lyme neuroborreliosis (LNB), which is the most common neurological manifestation of Lyme disease (LD), seriously impairs both the central and peripheral nervous systems. Current LNB diagnostic methods and criteria are not very effective. Recently, several studies have indicated that a high concentration of the chemokine CXC ligand 13 (CXCL13) in cerebrospinal fluid (CSF) could be used as a new biomarker for the diagnosis of LNB. Thus, we carried out a meta-analysis to systematically analyze the data from these studies to evaluate the value of CXCL13 as an LNB biomarker. After searching for articles in several databases, including PubMed, Embase, the Cochrane Library, and the China National Knowledge Infrastructure (CNKI), we included 7 articles in the meta-analysis with a total of 1299 patients with LNB or other neuroinflammatory diseases. From these 1299 patients, 343 patients with LNB served as the experimental group and 956 patients with other neuroinflammatory diseases or healthy individuals served as the control group. The analyses were performed using Meta-Disc1.4 statistical software. Based on the pooled specificity, sensitivity, positive likelihood ratio, negative likelihood ratio, diagnostic odds ratio, and summary receiver operating characteristic curve, we found that CXCL13 indeed has a high sensitivity and specificity for diagnosing LNB, which means that it can be used as a new diagnostic biomarker for the diagnosis of LNB.
Introduction
L
LNB seriously impairs both the central nervous system (CNS) and peripheral nervous system, which, during the early stages of LNB, can cause painful lymphocytic meningoradiculitis and cranial neuritis. In the later stages of LNB, symptoms include chronic meningitis, progressive encephalitis, myelitis, encephalomyelitis, and cerebral vasculitis. Other symptoms of LNB include headache, fatigue, memory loss, learning disability, depression, facial nerve palsy, limb pain, sensory loss, muscle weakness, and irreversible CNS damage (Ramesh and others 2008, 2015; Koedel and others 2015). As a result of the relatively high proportion of patients in Europe with serious LNB-related nervous system damage, LNB has become a compulsorily notifiable disease in several European countries (Stanek and others 2011).
Based on the abovementioned nonspecific symptoms, the clinical methods and criteria for LNB diagnosis should be easy to apply and have high specificity and sensitivity. According to the European Federation of Neurological Societies (EFNS) guidelines, the current diagnostic criteria for LNB are as follows: (1) neurological symptoms; (2) cerebrospinal fluid (CSF) pleocytosis; and (3) B. burgdorferi (Bb)-specific antibodies produced intrathecally (Ljøstad and Mygland 2008; Mygland and others 2010; Tumani and Cadavid 2011; Borde and others 2012). However, the current diagnostic methods and criteria have limitations. According to several reports, some patients with LNB do not have a positive Bb antibody index (AI). In the early stage of subacute cases, the clinician therefore usually has to make treatment decisions based on a suspicion of LNB (as identified by clinical symptoms and CSF pleocytosis). Furthermore, after successful therapy, Bb-specific intrathecal antibodies can persist for a long time. In addition, antibiotic therapy must often be initiated before AI results become available (Rupprecht and others 2005; Ljøstad and Mygland 2008; Borde and others 2012). Thus, it is clear that a new biomarker with high specificity and sensitivity would be helpful for early diagnosis of LNB.
The B lymphocyte chemokine CXC ligand 13 (CXCL13) was discovered in 1998 (Legler and others 1998). Initially, it was known as B cell-attracting chemokine-1 (BCA-1), because it is able to attract B cells. Researchers have found that CXCL13 plays an essential role in the establishment and maintenance of lymphoid tissue microarchitecture. Subsequent reports demonstrated that CXCL13 expression is upregulated in Helicobacter pylori gastritis (Galamb and others 2008), pulmonary tuberculosis (Kahnert and others 2007), and Bartonella henselae infection (Vermi and others 2006), suggesting that there is an association between CXCL13 and chronic bacterial infections (Rupprecht and others 2009).
Recently, many research articles have reported that CXCL13 is upregulated in the CSF of patients with LNB. Furthermore, these articles suggested that high CXCL13 concentrations in CSF can be regarded as a new biomarker for the diagnosis of LNB (Narayan and others 2005; Rupprecht and others 2005; Ljøstad and Mygland 2008; Kingwell 2011; Borde and others 2012; Moniuszko and others 2013). However, other articles have suggested that the diagnostic value of CXCL13 needs to be confirmed by further studies (Tumani and Cadavid 2011; Bremell and others 2013). Therefore, systematically analyzing the data from previous studies would be helpful to evaluate the value of CXCL13 as a new biomarker for LNB diagnosis and this was the aim of this meta-analysis.
Materials and Methods
Search strategy
We used a comprehensive search strategy to identify articles on the association between the concentration of CXCL13 and LNB from the following databases: PubMed, Embase, the Cochrane Library, and the China National Knowledge Infrastructure (CNKI). We collected all the relevant articles that were published before 27 May 2016. The key search words were “CXCL13,” “CXCL-13,” “BCA1,” or “BCA-1” together with “Lyme neuroborreliosis”.
Eligibility criteria
All the articles were independently assessed by 2 reviewers (J.R.Y. and X.L.H.). Any disagreements with regard to each assessment were resolved by discussing the issues until a consensus was reached. Articles were included if they matched all of the following criteria: (1) each patient with LNB had an LNB diagnosis that was confirmed by a clinician (based on internationally recognized methods and criteria), (2) the CXCL13 concentration in the CSF was assessed for all of the patients, (3) there were sufficient reported data for analysis, (4) patients with other neuroinflammatory diseases or healthy individuals served as the controls, and (5) the article was written in English. The exclusion criteria were as follows: (1) duplicate publications, (2) non-case–control studies (e.g., reviews), and (3) insufficient data reported for analysis.
Data extraction
All the data from each eligible article were independently extracted by 2 reviewers (J.R.Y. and X.L.H.) after they reached a consensus on all the information that needed to be extracted. The extracted information included the name of the first author, year of publication, study country, number of patients, and age range of patients (Table 1).
QUADAS, Quality Assessment of Diagnostic Accuracy Studies (Whiting and others 2003).
Quality assessment
Two reviewers (J.R.Y. and X.L.H.) independently scored each article using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool, which involves 14 questions (Whiting and others 2003). There are 3 potential answers to each question: “Yes” (which is given a score of 1) and “No” or “Unclear” (which are given scores of 0) (Table 1).
Statistical analysis
For the statistical analysis, we used standard methods that are recommended for diagnostic accuracy meta-analyses (Devillé and others 2002). According to the specificity, sensitivity, and number of patients in each study, we extracted the true positive (TP), false positive (FP), true negative (TN), and false negative (FN) values for each study. The TP, FP, TN, and FN values were used to calculate the overall diagnostic accuracy. We calculated the sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), and diagnostic odds ratio (DOR) and generated a bivariate summary receiver operating characteristic (SROC) curve using a bivariate meta-analysis model. A random effects model was used to calculate the pooled sensitivity, specificity, and other related indexes for the studies. The heterogeneity was assessed using the chi-squared and I 2 tests, and a P value <0.05 and an I 2 value >50% were taken to indicate statistically significant heterogeneity.
Spearman's correlation coefficient was used to evaluate whether the heterogeneity was caused by the threshold effect. As there were less than 10 included articles, a funnel plot could not be used to detect potential publication bias. All the analyses were performed using Meta-Disc1.4 for Windows statistical software (XI Cochrane Colloquium, Barcelona, Spain).
Results
Literature search
We found a total of 75 articles after the initial search, among them 26 duplicate articles and 7 reviews were excluded (Fig. 1). Furthermore, 3 articles were excluded because they were written in German or Japanese. In the next step, 27 articles were excluded because the research topic did not match our inclusion criteria, leaving 12 studies available for further full-text review. After carefully reading these articles, 5 with insufficient reported data were excluded and, finally, 7 articles were included in the meta-analysis (Fig. 1).
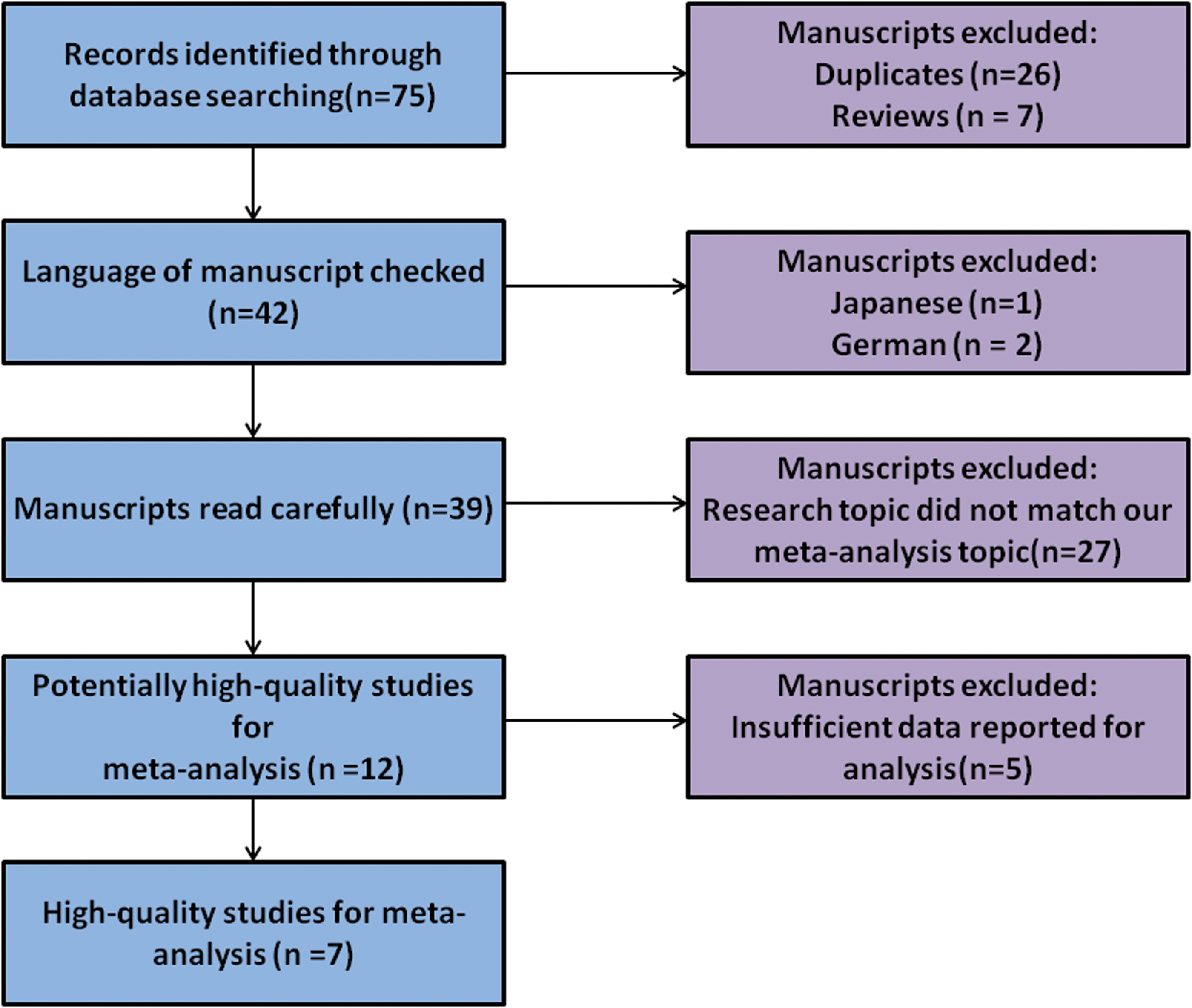
Flow diagram of literature search and article selection process. Color images available online at
Characteristics of included articles
In the 7 included articles, there were a total of 343 patients with LNB and 956 patients with other neuroinflammatory diseases or healthy individuals, which served as the experimental and control groups, respectively. The range of publication years was 2009–2014. According to the gold criterion for LNB diagnosis, each patient with LNB had their diagnosis confirmed by a clinician. All of the CSF samples were collected from patients in Germany, Sweden, Finland, Austria, or the Netherlands, and, for each sample, the CXCL13 concentration was assessed using an enzyme-linked immunosorbent assay (ELISA) (Table 1).
Quality of included studies
Two reviewers (J.R.Y. and X.L.H.) independently scored each article using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool. The QUADAS assessment led to each article being assigned a score of 11 or 12, which indicated that all the articles were of high quality (Table 1).
Data analysis
For each included article, the sensitivity, specificity, PLR, NLR, and DOR were evaluated, and an SROC curve was plotted.
Sensitivity and specificity
As there was significant heterogeneity for both sensitivity and specificity (I 2 = 73.2% and 84.7%, respectively), a random effects model was used. Figures 2 and 3 indicated that the pooled sensitivity and specificity were 0.97 (95% CI: 0.95–0.99) and 0.96 (95% CI: 0.94–0.97), respectively.
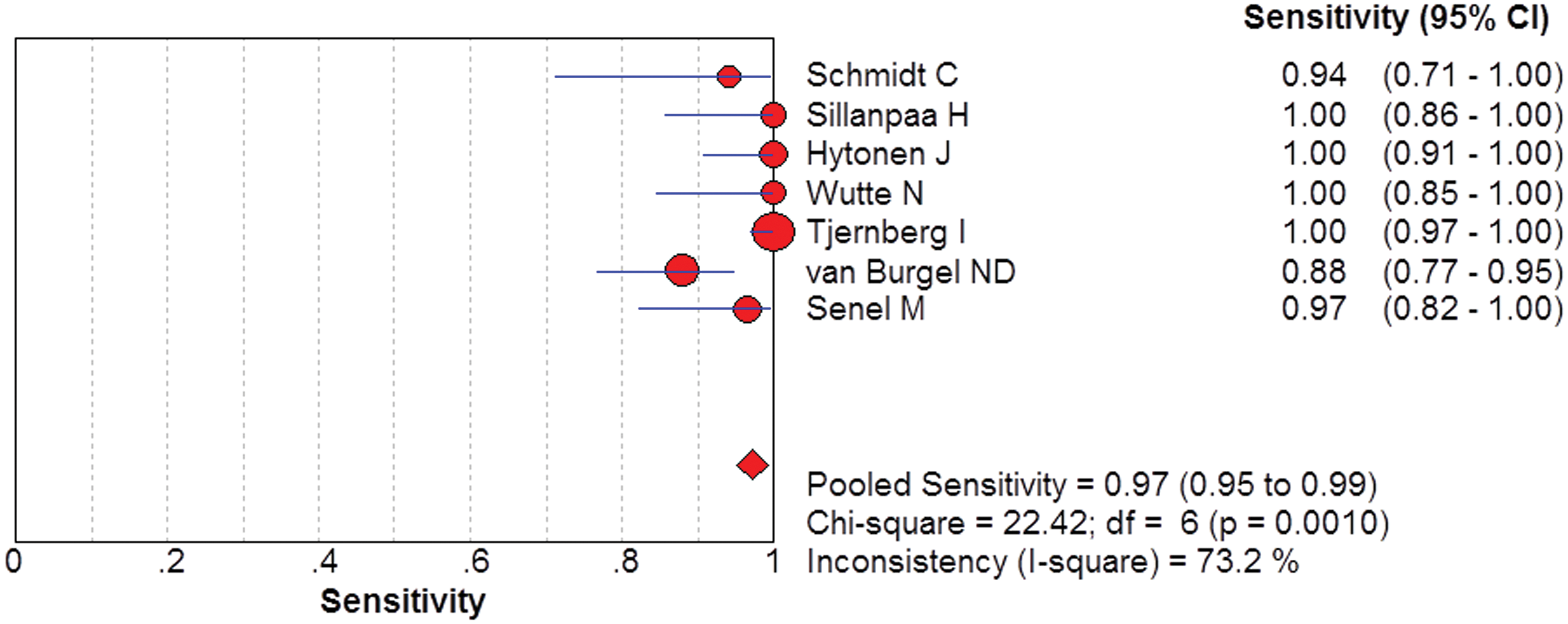
Pooled sensitivity of CXCL13 concentration for LNB diagnosis. LNB, lyme neuroborreliosis. Color images available online at
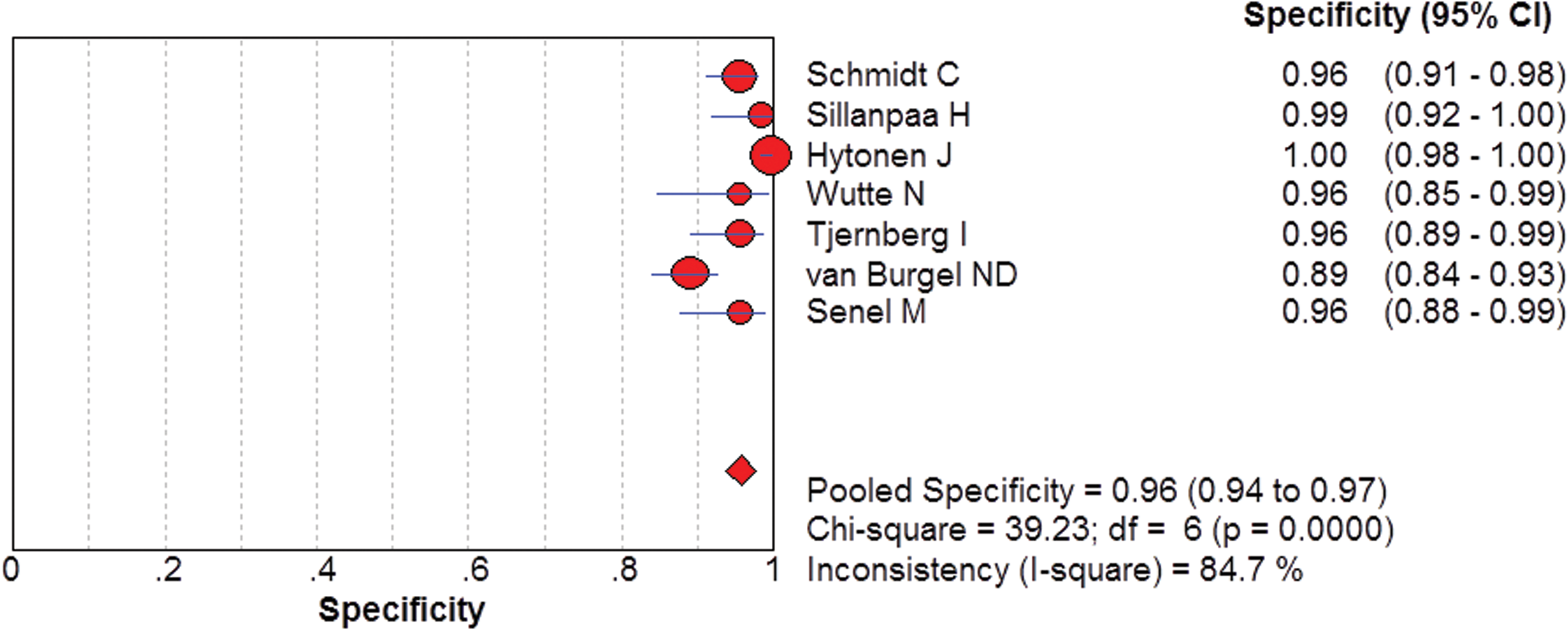
Pooled specificity of CXCL13 concentration for LNB diagnosis. Color images available online at
PLR and NLR
As the studies shared a common effect size and there was significant heterogeneity, a random effects model was used. According to Figs. 4 and 5, the pooled PLR was 23.71 (95% CI: 11.33–49.61) and the pooled NLR was 0.03 (95% CI: 0.01–0.11). The pooled PLR revealed that a comparison of patients with LNB to those with other neuroinflammatory diseases indicated that patients with LNB have a 23.71-fold increased likelihood of having a high concentration of CXCL13 in their CSF.
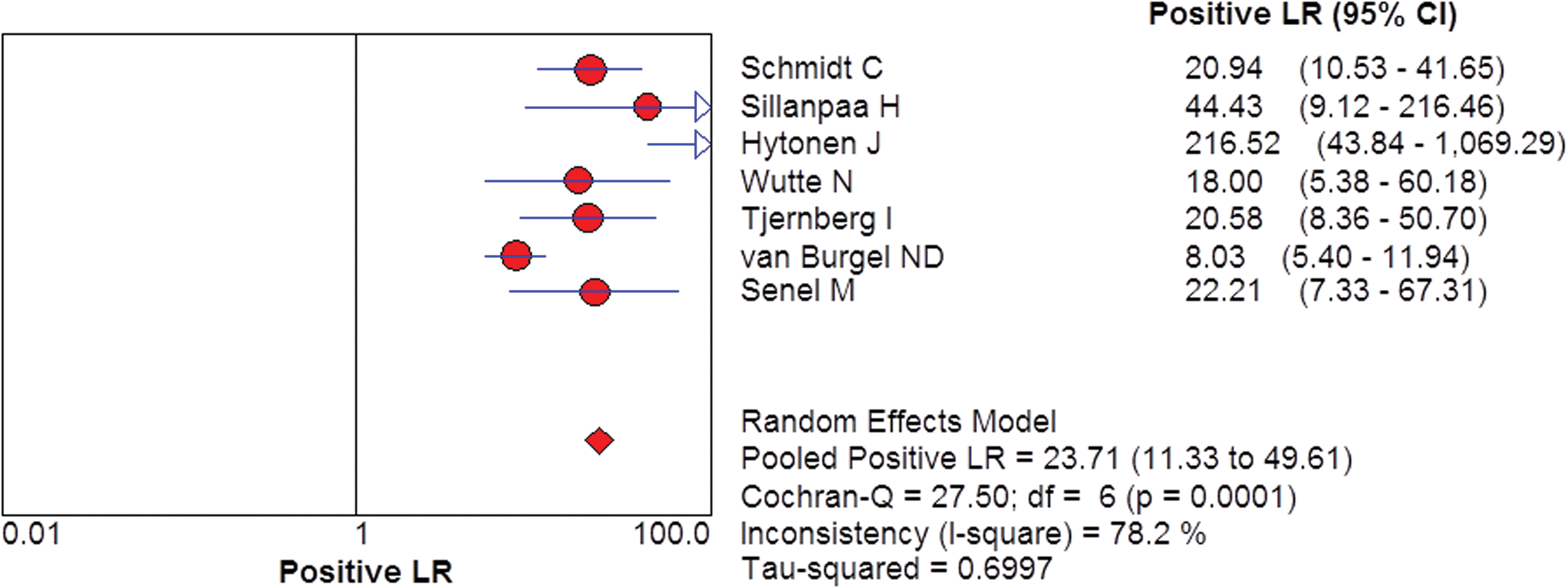
Pooled PLR of CXCL13 concentration for LNB diagnosis. PLR, positive likelihood ratio. Color images available online at
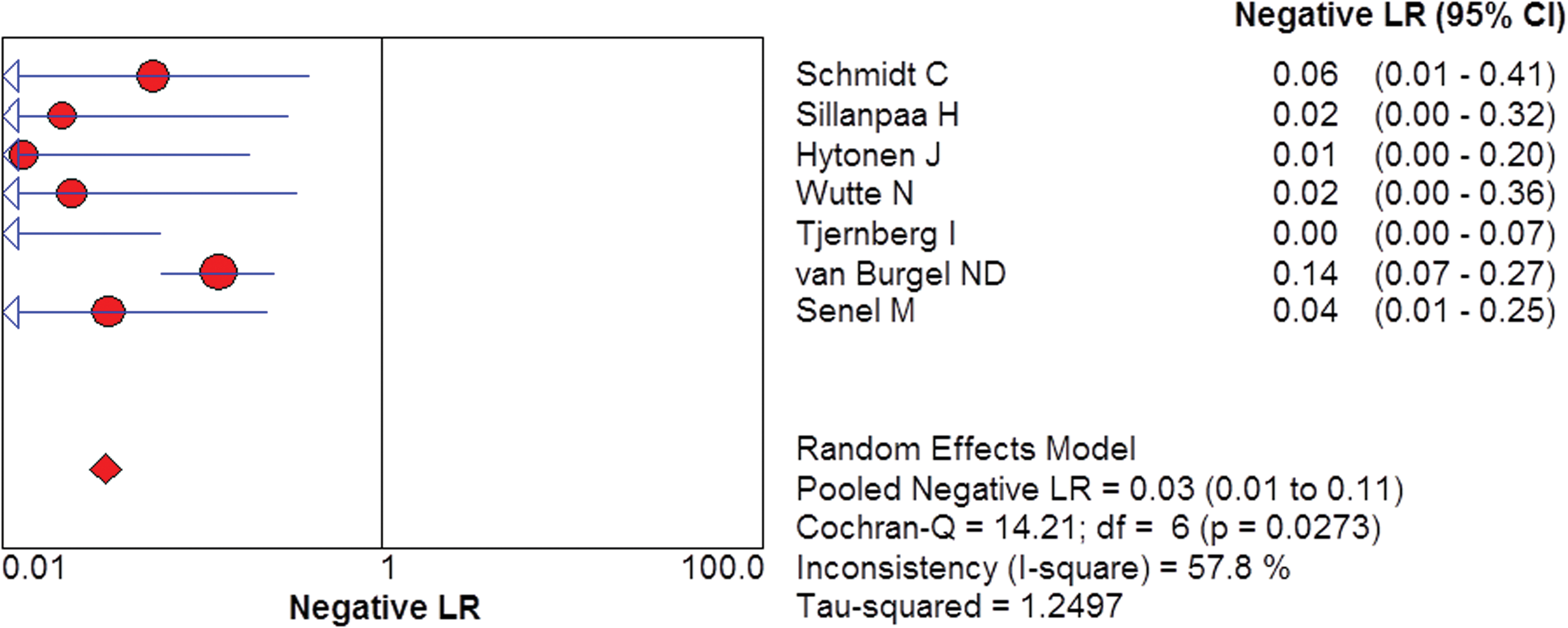
Pooled NLR of CXCL13 concentration for LNB diagnosis. NLR, negative likelihood ratio. Color images available online at
SROC curve and DOR
The SROC curve of all the included articles is displayed in Fig. 6. The pooled area under curve (AUC) was 0.9921 (95% CI: 0.9813–1.0029), and the DOR was 819.76 (95% CI: 149.09–4507.5).
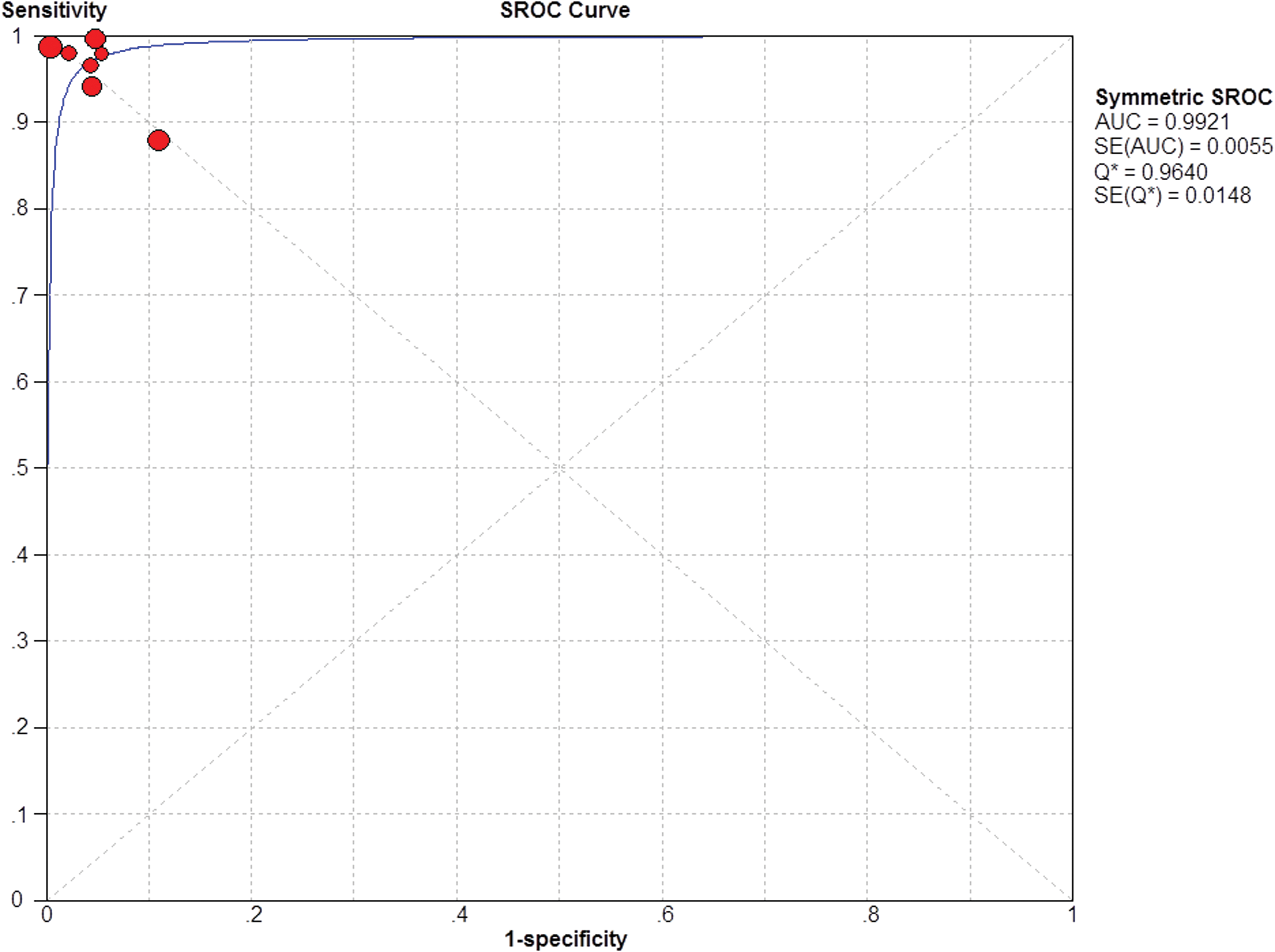
SROC curve of CXCL13 concentration for LNB diagnosis. SROC, summary receiver operating characteristic. Color images available online at
Publication bias
As there were less than 10 included articles, a test of publication bias was unsuitable and unnecessary, so no publication bias test was carried out.
Threshold effect
The threshold effect is a primary source of heterogeneity, and Spearman's correlation coefficient can be used to evaluate whether there is a threshold effect in a meta-analysis. In this meta-analysis, Spearman's correlation coefficient for the correlation between the sensitivity and 1–specificity was–0.464 and P = 0.294, which indicate that the significant heterogeneity in this meta-analysis was not caused by a threshold effect.
Discussion
The ideal diagnostic method for LNB is to directly assess whether the pathogen is present in the CSF. Unfortunately, <10% of bacterial cultures based on the CSF of patients with LNB are positive for B. burgdorferi (Karlsson and others 1990; Ogrinc and others 2013). The US Centers for Disease Control and Prevention and many public health agencies in Europe recommend using a 2-tier approach to serological testing for LNB diagnosis. However, as several studies have reported, many first-tier assays have relatively poor specificity, with FP rates >5% (Tugwell and others 1997; Wilske and others 2007; Koedel and others 2015). Other methods that have been used include body-fluid antigen tests, polymerase chain reaction analysis of urine samples, lymphocyte transformation tests (Dattwyler and others 1988; Valentinethon and others 2006; von Baehr and others 2012; Dessau and others 2014), enzyme-linked immunospot assays (ELISPOTs) (Nordberg and others 2012), natural killer cell counts (Stricker and Winger 2001), and xenodiagnosis (Bockenstedt and Radolf 2014). However, none of these methods are adequate for LNB diagnosis (Koedel and others 2015).
Many case–control studies have reported that the concentration of the chemokine CXCL13 is significantly associated with LNB. Based on recent reports that we have identified, CXCL13 is the only chemokine that could be used to diagnose LNB (Ljøstad and Mygland 2008; Koedel and others 2015). The CXCL13 concentration is only increased in the CSF of patients with early-stage LNB and it decreases faster than other indexes after patients are treated with antibiotics (Lalor and Segal 2010). Several reports have implied that CXCL13 has higher sensitivity, specificity, efficiency, and reliability than other known diagnostic parameters, which suggest that CXCL13 is a unique biomarker for early diagnosis of LNB. There are no previous studies that comprehensively analyze the diagnostic value of CXCL13. Therefore, we conducted this meta-analysis to systematically evaluate the clinical value of CXCL13 for LNB diagnosis.
In this meta-analysis, the pooled specificity and sensitivity were 0.97 (95% CI: 0.95–0.99) and 0.96 (95% CI: 0.94–0.97), respectively. Clearly, assessment of CXCL13 concentration is suitable and efficient for LNB screening. The DOR, defined as the ratio of the odds of a TP to the odds of a FP, can be used as a single indicator of diagnostic test accuracy (Glas and others 2003). A higher DOR value (>1) indicates a better diagnostic test. The DOR in this study was 819.76 (95% CI: 149.09–4507.5), which indicates that CXCL13 is a good biomarker for LNB diagnosis. An SROC curve is often used to summarize the overall diagnostic test performance, and the AUC is usually used to assess the accuracy of the diagnostic test. An AUC >0.97 indicates excellent accuracy and 0.93–0.96 indicates very good accuracy (Jones and Athanasiou 2005). The AUC in this study was 0.9921 (95% CI: 0.9813–1.0029), which means that CXCL13 is an excellent biomarker to screen for LNB and it has advantages over the other known diagnostic methods.
In a meta-analysis, heterogeneity is an important factor. The primary source of heterogeneity is the threshold effect, as different studies use different cutoff values to define positive and negative test results. To discover whether the observed heterogeneity is caused by the threshold effect, we used Spearman's correlation coefficient for the correlation between sensitivity and 1–specificity, which was–0.464 (P = 0.294). This indicates that there was no threshold effect. Thus, the heterogeneity is not from the threshold effect. Other potential factors that can cause heterogeneity include the number of patients, study country, patient ages, and publication year.
Although there were too few articles to assess potential publication bias, we believe that publication bias may exist due to the following reasons. First, all of the samples from patients with LNB in each included article were collected in Europe. Although LD is the most common serious infectious disease in temperate regions of the northern hemisphere, there were no LNB cases from any countries of other continents where LNB has been reported, which imply that publication bias may exist. Second, all of the LNB patients in one of the 7 included articles were children, while all of the LNB patients in the other articles were adults. This may undermine the value of CXCL13 for screening for LNB. Third, too few articles were included in our meta-analysis, which may also lead to potential publication bias.
The immunopathology of LNB is not entirely understood (Pietikäinen and others 2016). It is known that CXCL13 is a chemokine that can attract B cells. Regarding the role of B cells in LNB, many researchers have reported that the concentration of B cells in the CSF is greater for patients with LNB than those with other CNS diseases (Cepok and others 2003; Rupprecht and others 2008; Xing and others 2015). Currently, B cell pleocytosis in the CSF is one of the criteria for diagnosing LNB (Pietikäinen and others 2016). However, a more effective method for LNB diagnosis is necessary. According to the literature, CXCL13 is the only chemokine that is significantly increased in the CSF of patients with early-stage LNB compared to patients with other neuroinflammatory diseases and healthy controls. In addition, the CXCL13 concentration falls rapidly after antibiotic treatment (Ljøstad and Mygland 2013).
By utilizing a meta-analysis, we were able to systematically evaluate the value of CXCL13 for LNB diagnosis. The 4 significant indexes that should be the focus of a meta-analysis of a diagnostic indicator are the pooled specificity, pooled sensitivity, DOR, and AUC of the SROC curve, which were 0.97, 0.96, 819.76, and 0.9921, respectively. These indexes indicated that CXCL13 has high sensitivity and specificity for the early diagnosis of LNB. Given all of the advantages of CXCL13 for the early diagnosis of LNB, we suggest that CXCL13 could be used as a biomarker for LNB diagnosis. However, further studies on the diagnostic value of CXCL13 are needed.
Footnotes
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (No. 31560051 and 81560596) and the Natural Foundation of Yunnan Province (No. 2014FB001, 2014FA011, and 2013FZ057).
Author Disclosure Statement
No competing financial interests exist.