
Abstract
The aim of the study was to evaluate the association between the gene polymorphisms in interleukin-10 (IL-10) and interferon gamma (IFN-γ) genes with susceptibility and severity of hepatitis C virus (HCV) infection among Egyptian patients. Interleukin-10 -592 A/C, -1082 G/A and IFN-γ +874 T/A genotypes were determined in 100 chronic HCV patients and 50 healthy controls using restriction fragment length polymorphism (RFLP) and the amplification refractory mutation system-polymerase chain reaction (ARMS-PCR) respectively. IL-10 -592 A/C polymorphism genotyping revealed that the frequency of CC genotype was significantly higher in chronic HCV patients than in controls (58% versus 30%, P < 0.05). Regarding IL-10 -1082 G/A polymorphism genotyping, a higher frequency of GG genotype was found in chronic HCV patients compared to controls (31% versus 10%, P < 0.05). IFN-γ +874 T/A genotyping showed that TT genotype was significantly higher in chronic HCV participants than controls (31% versus 18%, P < 0.05), while a higher frequency of T allele was found in cirrhotic patients compared to noncirrhotic patients (P < 0.05). Our observations suggested that IL-10 -592 A/C, -1082 G/A, and IFN-γ +874 T/A polymorphisms had a strong association with susceptibility to HCV infection. However, no significant association was observed between the cytokines (IL-10 and IFN-γ) genotypes profile and HCV-liver cirrhosis risk in the studied population, except for the high frequency of IFN-γ +874 T allele in cirrhotic patients.
Introduction
H
Interleukin 10 (IL-10) is a T-helper type 2 cytokine which was known to downregulate the Th1 effector mechanisms and regulate the humoral immune responses (Ho and Moore 1994). Several polymorphic sites within the IL-10 gene promoter region have been described, which include 2 dinucleotide repeats and 3 biallelic polymorphisms at positions -1082, -819, and -592 from the transcription start site. These genetic polymorphisms produce 3 distinguished 3 different haplotypes: GCC, ACC, and ATA (Eskdale and others 1999). These haplotypes were shown to control the amount of cytokine production; AA genotype is associated with low IL-10 production, GA genotype is considered an intermediate producer, while GG genotype is considered a high producer (Edwards‐Smith and others 1999). In addition to that, these haplotypes have a prognostic implication where patients with a high production of IL-10 are more liable to develop chronic progressive liver disease, while those with a lower production of IL-10 tend to be asymptomatic carriers (Wang 2003).
Interferon gamma (IFN-γ) is a multifunctional cytokine which is secreted by the effector T and natural killer cells. This cytokine is crucial for host defense against a variety of intracellular pathogens, including HCV (Frese and others 2002). The IFN-γ gene is composed of 4 exons, with 3 introns. It was reported that the single nucleotide polymorphism (SNP) in IFN-γ +874 T/A (rs2430561) in the first intron (TT genotype) produces a high concentration of IFN-γ, which increases the host's defense against viral infection. Conversely, the genotypes AA and AT cause low IFN-γ production, which may increase the risk of viral infection (Pravica and others 2000). According to these foundations, the single nucleotide polymorphism (SNP) in the IFN-γ gene region can influence the IFN-γ production, which may modulate the immune response and consequently the risk of viral infection.
The aim of the study is to evaluate the gene polymorphism of IL-10 at sites (-1082 G/A and -592 C/A), as well as IFN-γ (+874 A/T), as potential of susceptibility to and progression of HCV in Egyptian patients.
Materials and Methods
Study patients
This is a case–control study which was conducted on 100 chronic HCV-infected patients who were recruited from the outpatient clinics of Tropical Medicine Department, Sohag University Hospital (Sohag, Egypt) during the period from January to June 2015. The participants were allocated into 2 groups: chronic HCV patients without cirrhosis (group I; n = 50) and chronic HCV patients with cirrhosis; Child-Turcotte-Pugh A (Pugh and others 1973) (group II; n = 50). Persistence of HCV antibodies and HCV RNA in the serum of the patients for more than 6 months were the criteria used for the diagnosis of chronic HCV. Any participant with serological evidence of hepatitis B virus (HBV) or HIV infection, decompensated hepatic cirrhosis, and hepatocellular carcinoma was excluded from the study. A total of 50 apparently healthy individuals with no history of hepatic disease and without serologic evidence of HCV or HBV infections were recruited as a control group. The study was approved by the official recommendations of the Ethics Committee of Sohag Faculty of Medicine, Sohag University, and written informed consents were obtained from all participants.
Diagnosis of HCV infection
All enrolled patients underwent detailed history taking, thorough clinical examination, routine laboratory investigations [complete blood count (CBC), liver biochemical profile, renal function (urea and creatinine), and blood glucose], specific HCV testing [anti-HCV antibodies by enzyme-linked immunosorbent assay (ELISA) and HCV RNA and viral load by real-time polymerase chain reaction (PCR)], abdominal ultrasound, and the histopathological assessment of necroinflammatory grade and fibrosis stage of liver biopsy, applying METAVIR scoring system (Bedossa and Poynard 1996); diagnosis of cirrhosis was based on either liver biopsy or ultrasonographic criteria of liver cirrhosis.
DNA extraction
Peripheral blood was collected in ethylene-diamine-tetraacetic acid tubes. Genomic DNA was extracted from the mononuclear cell layer using a QIAamp DNA Blood Mini Kit (QIAGEN, Germany) and stored at −20°C.
Polymorphism genotyping
IL-10 -592 A/C and IL-10 -1082 G/A SNPs were genotyped by restriction fragment length polymorphism (RFLP). Amplification was carried out in a thermocycler (Biometra) using 25 μL reaction volume containing × 10 PCR buffer (500 KCl, 100 mM Tris–HCl, 1.0% Triton X-100) 2.5 μL, 50 mM MgCl2 0.75 μL, 10 mM dNTPs 0.5 μL, each primer (10 pmol/mL) 1.0 μL (Table 1), 1.0 μL of template DNA, and Taq polymerase (5 U/μL) 0.125 μL. The PCR amplification was done according to the following protocol: denaturation at 95°C for 2 min, followed by 35 cycles of denaturation at 94°C for 30 s, annealing at 60°C for 45 s, and extension at 72°C for 1 min. This was followed by a final extension at 72°C for 10 min. RFLP assay was performed in a 20 μL reaction volume containing PCR product and specific restriction enzyme (Rsa 1 for IL10-592 A/C or Mnl I For IL10-1082 G/A), according to the manufacturer's instructions. Rsa 1 cuts IL10-592 A allele to generate two bands (236/176 bp) while Mnl I cuts IL10-1082 G allele into two fragments (106/33 bp). The digested products were visualized on a 2% agarose gel stained with 0.5 μg/mL ethidium bromide (Figs. 1 and 2).
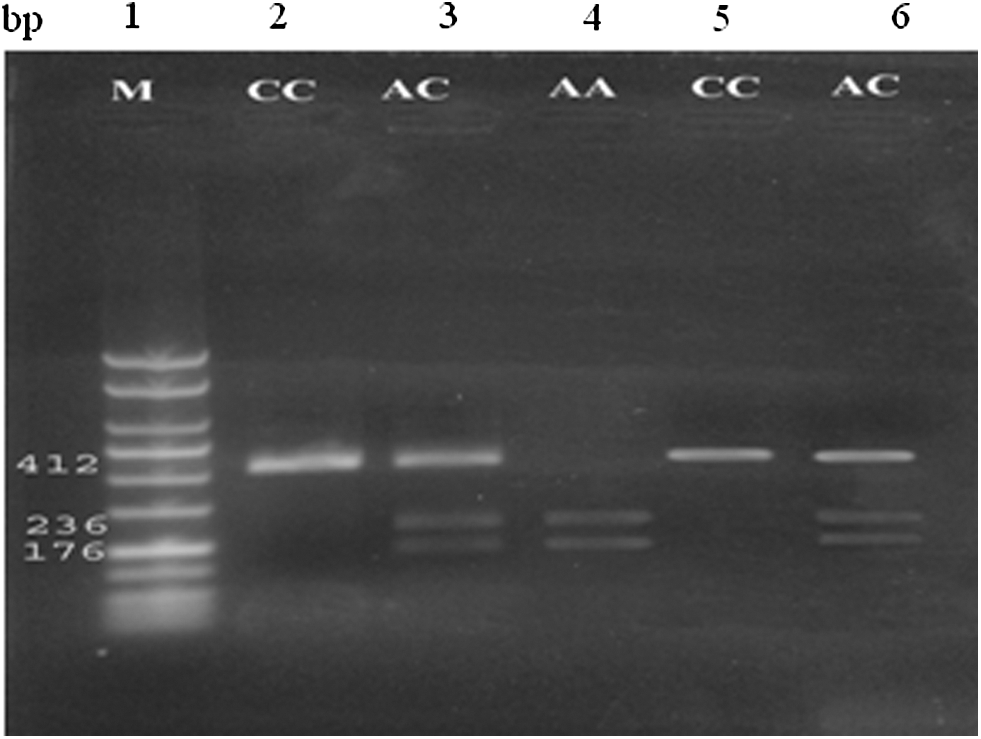
Representative agarose gel electrophoresis illustrating PCR products for the IL-10 -592 C/A polymorphism: lane 1, 100-bp marker. The resulting product was 412 bp, Rsa1 cut the product into 236- and 176-bp fragments in case of A allele, in case of C allele the enzyme will not cut the product. Lanes 2 and 5, homozygous CC subject; lanes 3 and 6, heterozygous subject AC; lane 4, homozygous AA subject. IL-10, interleukin-10; PCR, polymerase chain reaction.

Representative agarose gel electrophoresis illustrating PCR products for the IL-10 -1082 A/G polymorphism: lane 1, 100-bp marker. The resulting product was 139 bp, MnlI enzyme cut the resulting 139-bp fragment in case of G allele generating 106- and 33-bp (not shown) fragments. In case of A allele the resulting fragment will not be cut; lanes 2, 4, and 6, heterozygous subject; lanes 3 and 7, homozygous AA subject; lane 5, homozygous GG subject.
ARMS-PCR, amplification refractory mutation system–polymerase chain reaction; IFN-γ, interferon gamma; IL-10, interleukin 10; RFLP, restriction fragment length polymorphism.
IFN-γ +874 T/A polymorphism was genotyped by the amplification refractory mutation system (ARMS)-PCR assay in 2 separate PCR reaction mixtures. An internal control primer pair, which amplifies human growth hormone (HGH) gene, was used to check for successful PCR amplification (Table 1). The PCR reaction was performed in the following conditions: 95°C for 4 min, followed by 10 cycles of 95°C for 15 s, 62°C for the internal control for 50 s, 72°C for 40 s, and then 25 cycles of 95°C for 20 s, 49°C for 50 s, 72°C for 50 s, and 72°C for 10 min for the final extension. IFN-γ PCR product was 261 bp and HGH was 426 bp. The amplified products were separated by electrophoresis on 2% agarose gel stained with 0.5 μg/mL ethidium bromide (Fig. 3).

Representative agarose gel electrophoresis illustrating PCR products for the IFN-γ +874 T/A polymorphism; each participant has been represented by 2 lanes, one for the A allele and the other lane for T allele; in presence of both a product of 261 bp will be presented in each lane, the internal control (human growth hormone) product was 426 bp. Lanes 1 and 20, 100-bp marker; lanes 2–7, homozygous TT subject; lanes 8–11 and 16–19, heterozygous subject AT; lanes 12–15, homozygous AA subject. IFN-γ, Interferon gamma.
Statistical analysis
Statistical analysis of the data was performed using the computer program SPSS (Statistical Package for the Social Science; SPSS, Chicago, IL) version 15 for Microsoft Windows. The one-way analysis of variance (ANOVA) test was used to compare the laboratory data between the studied groups. The odds ratios and their corresponding 95% confidence intervals were calculated to compare the genotype frequencies; P values <0.05 were considered significant.
Results
The ages and genders of the participants were comparably similar in both the study and control groups. The levels of ALT and AST were significantly higher in the patients, while the albumin level and prothrombin concentration (%) were significantly lower in the patients in comparison to the controls (Table 2).
Data are represented as mean ± SD, n (%) or median (range).
P < 0.0001; b P < 0.05; c P < 0.001.
ALT, alanine transaminase; AST, aspartate transaminase; SD, standard deviation.
The genotype frequencies in all HCV patients versus control group were displayed in Table 3. Regarding IL-10 -592A/C polymorphism, higher frequency of CC genotype was found in HCV patients than in controls (58% versus 30%, odds ratio = 3.2, 95% confidence interval = 1.8–5.8; P < 0.05), while genotype AA was significantly higher in controls than in HCV patients (50% versus 19%, odds ratio = 0.2, 95% confidence interval = 0.12–0.44; P < 0.05). There was a significant association of IL-10 -592 C allele and HCV infection (odds ratio = 3.5, 95% confidence interval = 0.12–0.44, P < 0.05). IL-10 -1082 G/A polymorphism, GG genotype, was significantly higher in patients than in controls (31% versus 10%, odds ratio = 4, 95% confidence interval = 1.86–8.8; P < 0.05), while GA pattern frequency was higher in the controls than in the patients (70% versus 43%, odds ratio = 0.3, 95% confidence interval = 0.18–0.58, P < 0.05). The results of IFN-γ +874 T/A genotyping showed that TT genotype was significantly higher in the patients than controls (31% versus 18%, odds ratio = 2, 95% confidence interval = 1.1–3.97; P < 0.05). There was no significant association of IFN-γ +874 T and A alleles and HCV infection (odds ratio = 1.3, 95% confidence interval = 0.79–2.4; P > 0.05).
P < 0.05.
CI, confidence interval; HCV, hepatitis C virus; NS, not significant; OR, odds ratio.
Table 4 showed genotype frequencies of HCV patients in relation to cirrhosis. The frequency of IL-10 -592 A/C and IL-10 -1082 G/A was statistically comparable in patients with and without liver cirrhosis. In contrast, there was a significant association between IFN-γ +874 T allele and the occurrence of cirrhosis in HCV patients (odds ratio = 3.7, 95% confidence interval = 1.5–8.97, P < 0.05).
P < 0.05.
Discussion
Cytokine gene polymorphisms have been shown to influence and affect the overall expression and secretion of cytokines. The documented role of cytokines in modulating the immune response to HCV infection validates the assumption that detection of cytokine gene polymorphism is a pivotal step for predicting the possibility of both viral acquisition, as well as progression (Pasha and others 2013). In addition to these merits, an increased production of IFN-γ was shown to be associated with extended survival after HCV infection (Cyktor and Turner 2011).
In the present study, 2 polymorphisms of IL-10, IL-10 -592 A/C, and IL-10 -1082 G/A, and polymorphism of IFN-γ +874 T/A were studied in a cohort of HCV patients. The results of the study revealed an association of cytokine gene polymorphism and susceptibility to hepatitis C infection. IL-10 -592 CC genotype was significantly higher in HCV patients, while IL-10 -592 genotype AA was significantly higher in noninfected controls. However, there was no significant difference in genotype distribution between HCV patients with and without cirrhosis. These data comparably agree with the results reported in previous studies (Shaker and Sadik 2012; El Bassat and others 2013; Khan and others 2015).
IL-10 -1082 G/A polymorphism genotyping revealed that IL-10 -1082 G/A genotype was higher in controls than in HCV patients, while genotype GG was higher in HCV patients. In accordance with these results, IL-10 -1082 G/A genotype was found to be higher in healthy subjects than in HCV patients (Gao and others 2009; Afzal and others 2011; Li and others 2013). It was reported that the IL-10 -1082 G/G genotype was associated with higher IL-10 production, GA with intermediate production and AA with low production. Individuals carrying the high producer GG genotype may downregulate Th1 response, resulting in failure of HCV eradication and perpetuation of viral infection (Paladino and others 2006). These premises could explain the high rate of IL-10 -1082 G/A genotype in healthy individuals. The aforementioned mechanism was further reinforced by Koziel (2005) who concluded that predominance of Th1 cytokine profile may aid the body to recover from HCV infection. Conversely, patients who develop chronic HCV infection show a predominant Th2 response that downregulates the Th1 response and, thereby, favors persistence of HCV infection (Rehermann and Nascimbeni 2005).
IFN-γ is a cytokine which was shown to enhance the activity of TH1 cells and decrease the production of TH2 cells. Moreover, it suppresses the activity of HCV through affecting the viral RNA and protein synthesis, enhances immune lysis of HCV infected cells, inhibits hepatic fibrosis, and decreases HCV-induced carcinogenesis (Gattoni and others 2005; Ansari and others 2011).
IFN-γ +874 T/A polymorphism was first described by Pravica and others (2000) and was found to be associated with high IFN-γ production. In the present study, IFN-γ +874 T/A genotyping showed that T allele was associated with higher probability of development of liver cirrhosis in HCV patients, Bouzgarrou and others (2011) found similar results in Tunisian HCV patients, and Dai et al.(2006) also reported an increase in IFN-γ +874 T allele in Taiwanese HCV-infected patients complicated with cirrhosis. In contrast, Barrett and others (2003) and Abbas and others (2005) did not find any association between IFN-γ +874 T/A polymorphism and the severity of HCV infection. The difference in the sample size of the studied participants, genetic heterogeneity of the populations, and different gene–gene or gene–environment interactions could explain these contradictory findings between the different studies.
Despite the small number of the recruited participants, which is the main limitation of the current study owing to the financial limitations of the study hospital, the current study validated the contemporary role of cytokine gene polymorphism in patients with HCV infection. Moreover, it may help—in the future—in distinguishing the more risky patients for development of chronic HCV infection who may benefit from more intensive monitoring or a particular sort of therapy.
Conclusion
Our findings proved that IL-10 -592 A/C, -1082 G/A, and IFN-γ +874 T/A polymorphisms have strong association with susceptibility to HCV infection. However, we could not find out any significant association of the cytokines' (IL-10 and IFN-γ) genotype profile with HCV-liver cirrhosis risk in the studied population, except for the high frequency of IFN-γ +874 T allele in cirrhotic patients. Further studies with a larger sample size are required to confirm these results in different communities with different races.
Ethical approval
The study protocol was approved by the local Ethics Committee of Scientific Research in Sohag University, Faculty of Medicine, and consents were obtained from all participants before the study.
Footnotes
Acknowledgments
The authors are grateful to all who participated in the study. All laboratory investigations were done in the Central Research Lab, Sohag Faculty of Medicine without any external funding corporation.
Author Disclosure Statement
No competing financial interests exist.