
Abstract
Infection with hepatitis C virus (HCV) remains one of the serious human diseases worldwide, especially in Egypt, which can lead to cirrhosis or hepatocellular carcinoma (HCC). However, the exact molecular mechanism of HCC progress in HCV-infected patients remains unclear. Soluble fibrinogen-like protein 2 (sFGL2) is a modulator of the immune response that is secreted by T cells and inhibits maturation of dendritic cells and T cell proliferation. In the current study, serum sFGL2 levels were analyzed by enzyme-linked immunosorbent assay (ELISA) technique in 30 chronic HCV-infected patients (HCV group), 30 chronic HCV-infected patients with HCC (HCC group), and 12 healthy individuals (control group). Moreover, serum levels of soluble FAS ligand (sFASL) and interferon gamma (IFN-γ) were analyzed and correlated with sFGL2 levels. According to our results, serum sFGL2 levels were significantly elevated in all patients with chronic HCV infection. However, HCC patients showed lower sFGL2 levels than HCV-infected patients without HCC incidence. In addition, serum sFASL levels were significantly elevated in both HCV and HCC groups, whereas serum IFN-γ levels were only elevated in the HCC group. Interestingly, sFGL2 correlated positively with serum total bilirubin level and negatively with serum levels of sFASL, IFN-γ, and albumin in HCV and HCC groups. Thus, conclusively, sFGL2 level increases in Egyptian HCV-infected and HCC patients. Taken together, the current work may open future possibility of designing new treatment strategies for HCV infection targeting sFGL2 and its immunosuppressive effect.
Introduction
H
The immune system includes both innate and adaptive immune responses that provide host cells with the required defence mechanism against infection with foreign particles. The innate immune response is the first line of defence that has the ability to detect different viral infections and secretes different cytokines to develop antiviral defence response in the infected cells (Akira and others 2006; Echeverria and others 2015). On the other hand, adaptive immune response requires activation of antigen-presenting cells known as dendritic cells (DC) that play a critical role in the establishment of a successful immune response against viral infection by activating antiviral effector CD4+/CD8+ T lymphocytes (Szabo and others 2010). Indeed, it is recently proved that HCV alters both innate and adaptive immune response by interfering with interferons (IFNs) production, altering differentiation of DC and induction of T cell dysfunction that might explain the persistence of HCV infection (Ding and others 2013; Nitta and others 2013; Douam and others 2016).
Fibrinogen-like protein 2 (FGL2) is a member of fibrinogen-related protein superfamily that presents in two forms: soluble (sFGL2) and membrane (mFGL2) form (Doolittle 1990). mFGL2 has prothrombinase-like activity and, therefore, has the ability to convert prothrombin into thrombin that is responsible for its procoagulant activity (Levy and others 2000). On the other hand, sFGL2 is secreted by T cells and has immunosuppressive activity that prevents maturation of DC and subsequent T cell activation (Chan and others 2003). Based on the immunosuppressor effect of sFGL2, its overexpression during pathogen invasion can trigger serious complications and immune dysfunction (Yang and Hooper 2013).
FAS ligand (FASL) is a member of tumor necrosis factor (TNF) superfamily that is able to induce apoptosis and cell death after binding to its corresponding death receptor FAS (Manago and Yonehara 2005). FAS receptor is expressed in different normal and defected cells, whereas FASL is expressed mainly in immune cells such as natural killer cells and activated T cells (Iwai and others 1994). Therefore, FAS/FASL pathway plays an important role in controlling immune response and induction of apoptosis as a defence mechanism against tumor progression (Nagata 1997). However, many tumor cells develop resistance against FAS-induced apoptosis and immune response as a strategy to escape from host cell defence mechanism (Nagao and others 1999).
In the current study, we investigated serum sFGL2 levels in chronic HCV-infected patients with and without incidence of HCC using enzyme-linked immunosorbent assay (ELISA) technique. In addition, we analyzed serum levels of soluble FAS ligand (sFASL) and IFN-γ. Moreover, the serum sFGL2 levels were correlated with serum sFASL, IFN-γ, total bilirubin, albumin, and aspartate transaminase (AST) levels in HCV and HCC groups to study the role of sFGL2 in the etiology of liver damage and HCC development in HCV-infected patients.
Materials and Methods
Patients and blood samples
Blood samples were collected in hospitals of Mansoura University from 30 chronic HCV-infected patients (HCV group), 30 chronic HCV-infected patients with HCC (HCC group), and 12 healthy individuals (control group). This work was done after the approval of the Research Ethics Committee in the Faculty of Pharmacy, Mansoura University, Egypt. Moreover, the participants' rights, subjects, and interests were protected in this research.
Exclusion criteria were diabetes, acute HCV infection, mixed hepatitis B virus-HCV infection, and patients receiving immunosuppressive and antiviral drugs. Data concerning age and hemoglobin concentration were collected and summarized in Table 1. Abdominal ultrasound examination was performed to detect incidence of HCC development.
Data and biochemical parameters of HCV group (n = 30), HCC group (n = 30), and control group (n = 12). Data are represented as mean ± SD.
AFP, α-fetoprotein; ALT, alanine transaminase; AST, aspartate transaminase; HB, hemoglobin; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; WBCs, white blood cells.
In brief, 5 mL blood samples were collected by vein puncture from each patient and half quantity was left with anticoagulant to obtain whole blood samples and the other half was left to clot at room temperature for 20–30 min to isolate serum samples after centrifuging clotted blood samples at 1,500 rpm for 10 min. Serum samples were stored at −80°C until further analysis.
Measurement of serum levels of sFGL2, FASL, and IFN-γ
sFGL2 levels were analyzed in serum samples using the LEGEND MAX™ Human sFGL2 ELISA Kit (BioLegend Company, USA) according to the protocol of the manufacturer. Serum sFASL and IFN-γ were analyzed using the corresponding ELISA Kit (eBioscience Company, Germany) according to the protocol of the manufacturer.
Liver function analysis
Isolated serum samples were used to analyze liver enzymes (alanine transaminase [ALT] and AST), albumin, and total bilirubin using the corresponding detection kits according to the instruction of the manufacturer (ELITech Clinical Systems, France). α-fetoprotein levels were measured in serum samples using the ELISA Detection Kit (Calbiotech Company, USA) according to the protocol of the manufacturer.
Statistical analyses
Results were statistically analyzed using the GraphPad Prism 5.0 program (GraphPad Software, Inc.). Data of patients were expressed as mean ± standard deviation (SD). Student's t-test was used to calculate P values (*P ≤ 0.05, **P ≤ 0.01, ***P ≤ 0.0001).
Results
Patients' characteristics
Patients' characteristics and biochemical parameters are indicated in Table 1 and represented as mean ± SD.
Analysis of serum sFGL2 levels in HCV and HCC groups
Serum sFGL2 levels were analyzed in the HCV group (n = 30), HCC group (n = 30), and control group (n = 12). According to our results, sFGL2 levels were significantly elevated in HCV and HCC groups as compared with the control group (Fig. 1). Interestingly, sFGL2 levels were significantly higher in the HCV group than in the HCC group (Fig. 1).
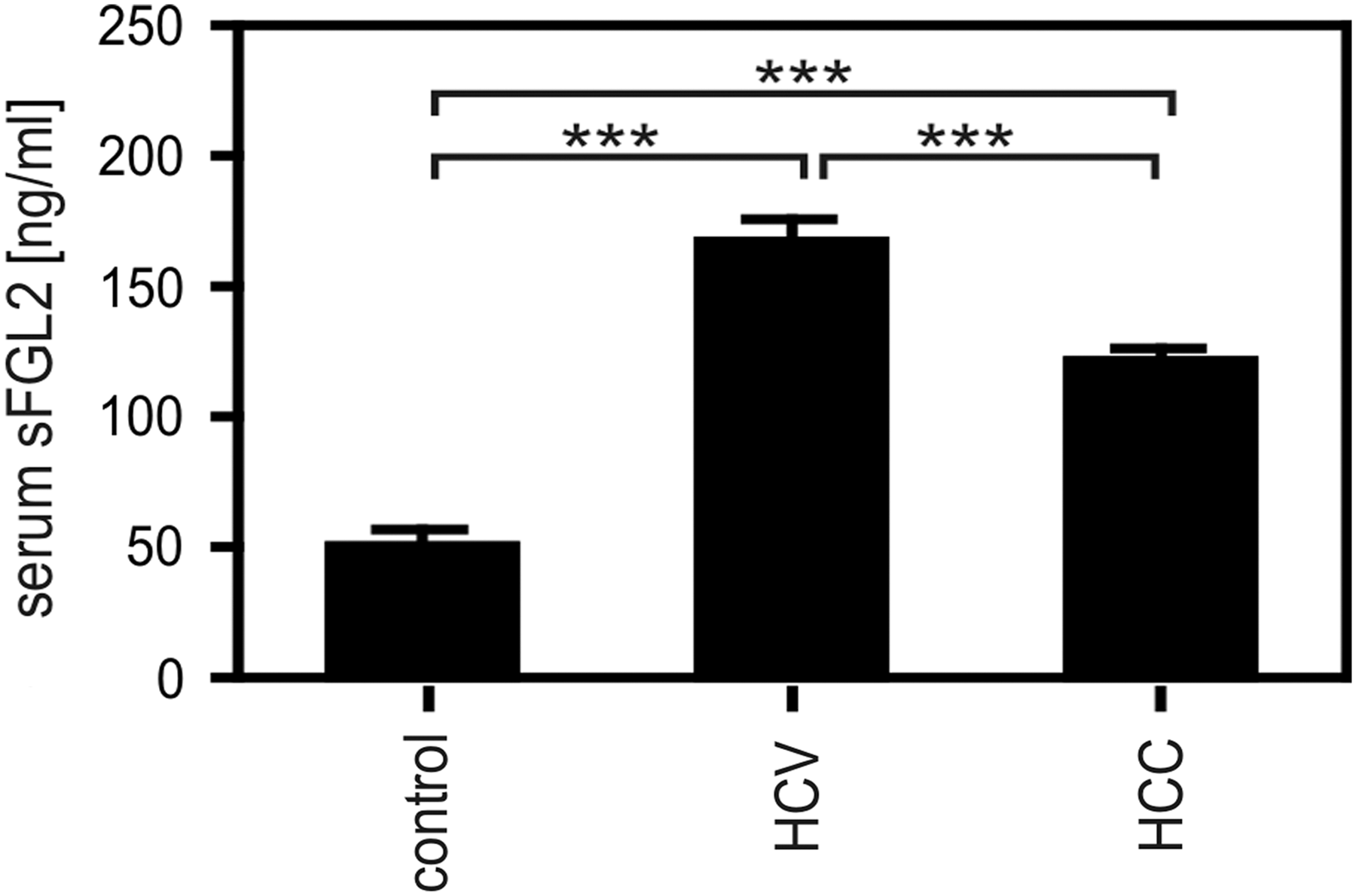
Analysis of serum sFGL2 levels in HCV and HCC groups. Serum sFGL2 level was analyzed in HCV group (n = 30), HCC group (n = 30), and control group (n = 12) using ELISA method. The asterisks indicate significant difference (P ≤ 0.0001). ELISA, enzyme-linked immunosorbent assay; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; sFGL2, soluble fibrinogen-like protein 2.
Analysis of serum sFASL and IFN-γ levels in HCV and HCC groups
Immune response in HCV and HCC groups was characterized by analyzing the serum levels of sFASL and IFN-γ. According to our results, HCC group showed a significant increase in both sFASL and IFN-γ serum levels as compared with the HCV group and the control group (Fig. 2). On the other hand, HCV group showed only a significant elevation in the serum sFASL levels as compared with the control group (Fig. 2).
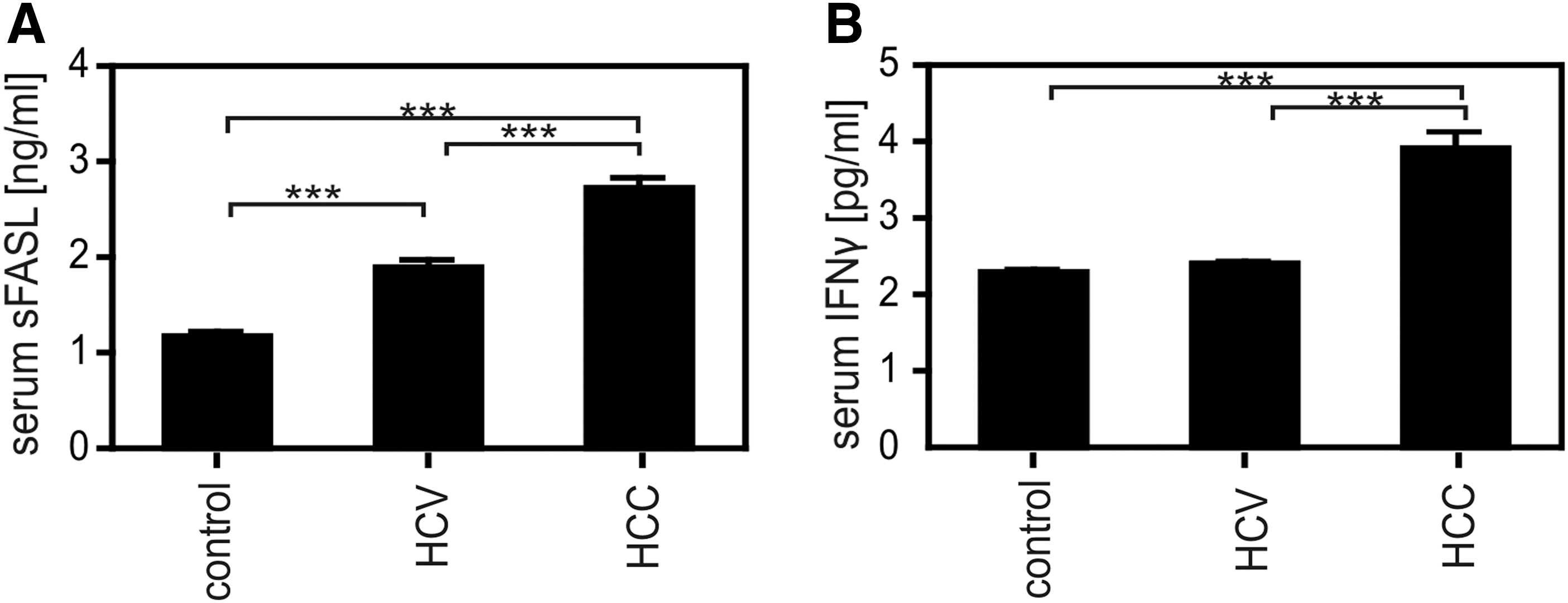
Analysis of serum sFASL and IFN-γ levels in HCV and HCC groups. Serum sFASL
Correlations of serum sFGL2 levels with sFASL and IFN-γ levels in HCV and HCC groups
As far as sFGL2 levels were significantly elevated in HCV and HCC groups, it was interesting to analyze the correlations between sFGL2 levels and sFASL and IFN-γ levels in HCV and HCC groups. Statistical analysis revealed a strong negative correlation between sFGL2 levels and sFASL levels (r 2 = −0.6602) (Fig. 3A) and a weak negative correlation between sFGL2 and IFN-γ levels (r 2 = −0.1049) (Fig. 3B).

Correlations of serum sFGL2 levels with sFASL and IFN-γ levels in HCV and HCC groups. sFGL2 levels were correlated with both serum sFASL and IFN-γ levels in HCV and HCC groups. There is a strong significant negative correlation between sFGL2 levels and sFASL levels
Correlations of serum sFGL2 levels with serum albumin and bilirubin levels in HCV and HCC groups
To investigate whether the increased sFGL2 levels correlated with liver function in HCV and HCC patients, we analyzed the correlation between serum sFGL2 levels and total bilirubin, serum albumin, and AST levels. As indicated by our results, there was a significant positive correlation between sFGL2 and total bilirubin levels (r 2 = 0.3212) (Fig. 4A) and a significant negative correlation between sFGL2 and albumin levels (r 2 = −0.3646) (Fig. 4B). However, there was no significant correlation between serum sFGL2 and AST levels (Fig. 4C).

Correlations of serum sFGL2 levels with serum albumin, bilirubin, and AST levels in HCV and HCC groups. Serum sFGL2 levels were correlated with serum albumin, total bilirubin, and AST levels. There is a significant positive correlation between sFGL2 and total bilirubin levels
Discussion
HCV represents one of the serious human diseases that can lead to the development of HCC (Cameron 2015). As far as the role of HCV in HCC development has been proved, several research efforts have been directed to study the molecular mechanisms of HCC development in HCV-infected patients (De Minicis and others 2013; Rongrui and others 2014; Mileo and others 2015; Tan and Li 2015). One of the possible explanations is the ability of HCV to alter both innate and adaptive immune response that impairs host defence mechanism (Ding and others 2013; Nitta and others 2013; Douam and others 2016).
sFGL2 is a novel immune regulatory molecule that is secreted by hepatic stellate cells and plays an important role in immune regulation by inhibiting DC maturation and the subsequent T cell activation (Chan and others 2003; Sun and others 2014). To our knowledge, there is no study that reveals the role of sFGL2 in Egyptian HCV-infected patients, despite the predominance of HCV infection in Egypt. Therefore, we were motivated in this study to investigate sFGL2 expression in HCV-infected and HCC patients. We analyzed serum sFGL2 levels in both HCV and HCC groups and compared them with a control group using ELISA technique (Fig. 1). According to our results, sFGL2 levels increased significantly in HCV and HCC groups as compared with the control group. Consistent with our results, recent studies revealed the elevated sFGL2 levels in HCV and HCC groups (Chaerkady and others 2008; Sun and others 2014). Thus, accumulating evidence has demonstrated that HCV modulation of innate and adaptive immune response may be attributed to sFGL2 secretion. Although we detected a significant increase of sFGL2 levels in HCV and HCC groups, sFGL2 levels were lower in HCV-infected patients with HCC than HCV-infected patients without incidence of HCC that may reflect one of the molecular changes in the host immune defence mechanism after HCC development.
FASL is a death ligand of TNF superfamily that is able to induce apoptosis and suppresses tumor progression by binding to its corresponding death receptor FAS (Ehrenschwender and Wajant 2009; Villa-Morales and Fernandez-Piqueras 2012). Regarding FAS/FASL distribution, liver represents the body organ with abundant FAS distribution, whereas FASL is highly expressed on activated T lymphocytes (Watanabe-Fukunaga and others 1992; Suda and others 1993, 1995). HCV infection induces host immune defence mechanism that leads to the migration of HCV-specific T cells into hepatocytes (Galle and others 1995; Hayashi and Mita 1997). Interestingly, FASL expression is increased upon T cell activation that induces apoptosis and subsequent damage to hepatocytes expressing FAS (Galle and others 1995; Hayashi and Mita 1997). Moreover, several research studies have detected the role of abnormal activation of FAS/FASL pathway in the pathogenesis of chronic liver diseases (Galle and others 1995; Nagata 1996; Hammam and others 2012). According to our results, sFASL was significantly increased in both HCV and HCC groups (Fig. 2A). Moreover, sFASL was significantly increased in HCC group as compared with HCV group that may indicate the activation of FAS/FASL pathway as immune defence mechanism against HCC development.
To analyze the host immune defence mechanism, we analyzed serum IFN-γ levels. According to our results, we detected no significant increase in serum IFN-γ levels in HCV group (Fig. 2B). On the other hand, serum IFN-γ levels were significantly increased in HCC group (Fig. 2B). It was previously detected that HCV envelope 2 glycoprotein binds to the surface of NK cells impairing IFN-γ release that leads to the impairment of the antiviral response induced by host immune system during HCV infection (Crotta and others 2002; Tseng and Klimpel 2002). However, the significant elevation of IFN-γ in HCC patients indicates molecular changes in the immune response that leads to overproduction of IFN-γ. To investigate the impact of sFGL2 expression on host immune response, we performed correlation studies between serum sFGL2 levels and serum levels of both sFASL and INF-γ in HCV and HCC groups (Fig. 3). According to our results, there is a negative correlation between serum sFGL2 levels and both sFASL (r 2 = −0.6602, P < 0.0001) and IFN-γ levels (r 2 = −0.1049, P = 0.0116). This negative correlation indicates that sFGL2 plays an important role in suppressing the immune response and the expression of different immune regulating molecules, such as sFASL and IFN-γ, in chronic HCV-infected patients.
In addition, sFGL2 level significantly correlated with liver functions as indicated by the positive correlation between sFGL2 levels and serum total bilirubin (r 2 = 0.3212, P < 0.0001) and the negative correlation between sFGL2 and serum albumin (r 2 = −0.3646, P < 0.0001) (Fig. 4). Thus, conclusively, this study is the first report that indicates the increase of sFGL2 level in the Egyptian HCV-infected and HCC patients, which may represent a novel target to design effective immunotherapeutic strategy for HCV infection. However, further research studies are required to explain the molecular mechanisms of sFGL2 expression in chronic HCV-infected patients and the decrease in its levels after HCC development.
Footnotes
Acknowledgments
This work was supported in part by financial support to Dr. Mohamed El-Mesery (Application number 41590) and Dr. Mohammed El-Mowafy (Application number 39462) through the Returning Experts Program that is implemented by the Center for International Migration and Development (CIM) on behalf of the German Federal Ministry for Economic Cooperation and Development (BMZ).
Author Disclosure Statement
No competing financial interests exist.