
Abstract
In viral meningitis, proinflammatory cytokines were detected at higher levels in the cerebrospinal fluid (CSF) and might play an important role in the inflammatory process. Our goal was to compare the cytokine profiles in the CSF of children of enteroviral meningitis (EVM) with versus without CSF pleocytosis. In total, 158 patients were enrolled in this prospective cohort study and were classified as EVM (group-A, n = 101), nonenteroviral aseptic meningitis (group-B, n = 27), and control (group-C, n = 30) groups. Of the 101 children with EVM, 71 had CSF pleocytosis (group-A1) and 30 had CSF nonpleocytosis (group-A2). Fifteen cytokines/chemokines in the CSF were measured simultaneously by immunoassay. Significant differences were found in interleukin (IL)-2, IL-6, and IL-8 levels in the CSF across the 3 groups, with the highest levels in group-A, followed by group-B and group-C. The levels of IL-1β, IL-2, IL-6, IL8, IL-10, interferon-γ, and tumor necrosis factor-α were significantly higher in the CSF of group-A1 than in that of group-A2. Group-A2 was significantly younger than group-A1 (3.4 ± 2.8 years versus 5.5 ± 3.2 years, P = 0.016). Significant differences between CSF pleocytosis and nonpleocytosis in EVM appear to be associated with distinct levels of CSF cytokines.
Introduction
A
The spectrum of illness caused differed among virus types. Enterovirus 71 usually causes hand, foot, and mouth disease and herpangina in children, also, can cause severe infection of the CNS, such as meningitis, poliomyelitis-like syndrome, and brainstem encephalitis (Wang and others 2007). Recent consideration has been directed toward the role of cytokines in the regulation of inflammation and host responses to CNS infection (Mukai and others 2006; Griffiths and others 2012). Normally, cellular expression of cytokines in CNS is highly combined and under regulation. However, in certain pathological conditions, cytokine production may become spatially and temporally dysregulated, leading to inappropriate production.
Data from the literature advocate that the release of specific cytokines, such as interleukin (IL)-1, IL-8, tumor necrosis factor (TNF)-α, and interferon (IFN)-γ, may be responsible for meningeal inflammatory infiltration in bacterial and aseptic meningitis and may be associated with the disease outcome (Azuma and others 1997; Dalal and others 2003; Sulik and others 2014). IL-1 family is a group of 11 cytokines, which plays a central role in the regulation of immune and inflammatory responses to infections. IL-1α and IL-1β are the most studied members, because they possess strongly proinflammatory effect. IL-8 is a 10-kDa proinflammatory chemokine that belongs to the CXC family of chemokines and plays a key role in neutrophil infiltration in infectious CNS inflammation and contributes to extensive spinal cord lesion in multiple sclerosis. TNF-α is an important proinflammatory cytokine and apoptotic molecule involved in the pathogenesis of neuroinfection. Measurement of this cytokine in bacterial and aseptic meningitis has a sensitivity of 74% and a specificity of 81%. IFN-γ is not normally present in the brain parenchyma (Olsson and others 1994). The source of CSF IFN-γ in the CNS inflammatory state has been attributed to infiltrating activated CD4+ T cells and neuronally activated astrocytes and microglia. The proinflammatory cytokine IFN-γ is a good indicator of antigen-specific cellular immunity (Asano and others 2011).
The standard method for identification of enteroviruses is the use of neutralizing antibodies in virus culture. Enteroviral meningitis (EVM) is clinically defined as the presence of pleocytosis and detection of the enteroviral genome in cerebrospinal fluid (CSF) by a reverse-transcriptase real-time polymerase chain reaction (RT-PCR) or viral culture (Rittichier and others 2005; Khetsuriani and others 2006). EVM unaccompanied by CSF pleocytosis has been confirmed through CSF enteroviral RT-PCR testing, including in young infants (Graham and Murdoch 2005; Seiden and others 2010). Although a few studies have reported the lack of CSF pleocytosis in children with EVM, to the best of our knowledge, clinical and laboratory characteristics, including CSF cytokine profiles, of these children have not been documented in the literature thus far.
The aim of our study was to investigate the cytokine profiles in the CSF of children with 2 different types of EVM (ie, with and without pleocytosis) to determine their role in causing CNS inflammation. We also compared data obtained from patients with EVM to those with aseptic meningitis caused by other viruses to identify EVM-specific cytokine alterations in CSF.
Materials and Methods
Subjects
A prospective cohort study from a single center was undertaken at the emergency and pediatric neurology clinics affiliated with Pusan National University Children's Hospital in South Korea. The study was performed between March 2015 and February 2016. The study population consisted of children ≤16 years of age suspected of having meningitis or increased intracranial pressure. At the initial visit, all children had clinical signs and symptoms of meningitis and their CSF was examined with routine CSF analysis, bacterial and viral culture, and the RT-PCR tests for enterovirus, herpes simplex virus-1 and 2, Epstein-Barr virus, and Mycobacterium tuberculosis. We considered any patient with only positive RT-PCR results for enterovirus in the CSF to have EVM. The exclusion criteria were as follows: (1) prior diagnosed epilepsy, chromosomal anomaly, or inborn error of metabolism, (2) combined severe poor condition (eg, shock, severe malnutrition, congestive heart failure, or acute or chronic renal failure), or (3) chronic intake of other medication within the previous 3 months (eg, antiepileptic drugs, corticosteroids, immune-modulating therapies). According to their diagnosis, patients were divided into 3 groups: group-A (n = 101), consisting of EVM patients; group-B (n = 27), consisting of patients with nonenteroviral aseptic meningitis, that clearly demonstrated viral meningitis based on the CSF analysis, even though any specific viral etiologies and enterovirus were not confirmed in their specimens; and group-C (n = 30) consisting of the control group. The control group consisted of 30 age- and sex-matched children with suspected increased intracranial pressure due to severe headache, nausea, or vomiting, and/or drowsy mentality. In these children, CSF examination disclosed a normal leukocyte count, normal opening pressure (7–15 mmHg), and negative virological tests of several RT-PCRs and culture, and, on that basis and clinical follow-up, the diagnosis of meningitis or systemic infection was excluded. Group-A patients were divided into 2 subgroups: patients with EVM and CSF pleocytosis (group-A1) and those with EVM with CSF nonpleocytosis (group-A2).
Standard protocol approvals, registrations, and patient consents
This study was approved by the Institutional Review Board of Pusan National University Yangsan Hospital (number: 04-2015-009). Informed consent was received from each participant's parent or guardian included in the study.
Sample and data collection
Lumbar puncture (LP) was performed within 48 h after hospital admission. All patients underwent routine CSF collection for analysis, which included cell count, the proportion of polymorphonuclear and mononuclear cells, and levels of protein and glucose. CSF samples contaminated by red blood cells were excluded. After a routine analysis, the remaining CSF samples were centrifuged and frozen for the purpose of this study. The patients' medical data were recorded together with the CSF findings.
Clinical and laboratory data were obtained from the medical records, which included sex, age, symptoms and signs with duration, interval period from the onset of initial symptoms to LP, findings from the physical examination, results of blood and CSF studies, results of virological testing of the CSF, and neurological outcomes. The laboratory data for the peripheral blood were included only if blood sampling occurred within 2 h before or after LP.
Definitions
EVM was defined as the detection of enterovirus in the CSF through viral culture or RT-PCR. CSF pleocytosis was defined as the presence of an elevated leukocyte count in the CSF. The age-specific definitions of CSF pleocytosis were a CSF white blood cell (WBC) count of >22/mm3 if the patient's age was <4 weeks, >15/mm3 if the patient's age was 4–7 weeks, or >5/mm3 if the patient's age was ≥8 weeks (Bonadio and others 1992).
Virological tests
GeneXpert assays (Cepheid, Sunnyvale, CA) (Ishiguro and others 1996) were used for the enteroviral RT-PCR assays. The primers and probes were from the portion of the enteroviral genome that codes for the 5′-nontranslated region. The primer sequences used in GeneXpert were 5′-CCC TGA ATG CGG CTA ATC C-3′(F) and 5′-ATT GTC ACC ATA AGC AGC CA-3′(R). The probe sequence was 5′-AAA CAC GGA CAC CCA AAG TAG TCG G-3′. The clinical sensitivity and specificity for enterovirus detection in the GeneXpert assay have been found to be 98%–100% and 90%–98.1%, respectively (Kost and others 2007).
Multiplexed immunoassay
The CSF cytokine concentrations were analyzed simultaneously for 15 different cytokines and chemokines, IL-1β, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12 (p70), IL-13, IL-17, IFN-γ, TNF-α, granulocyte colony-stimulating factor, and granulocyte monocyte colony-stimulating factor. All concentrations were determined using the Bio-Plex Cytokine Assay System (Bio-Rad Laboratories, Inc., Hercules, CA) in accordance with the manufacturer's instructions. A total of 50 μL of each CSF supernatant along with cytokine standards (Bio-Rad Laboratories, Inc.,) were added to a 96-well plate. The plate was analyzed using the Bio-Plex Array Reader (Bio-Rad Laboratories, Inc.,). The cytokine levels were calculated by reference to the standard curves for each cytokine. The lower detection limit for each cytokine was as follows: 1.04 pg/mL for IL-1β, 20.14 pg/mL for IL-2, 6.48 pg/mL for IL-4, 11.72 pg/mL for IL-5, 5.21 pg/mL for IL-6, 0.91 pg/mL for IL-7, 8.68 pg/mL for IL-8, 0.76 pg/mL for IL-10, 150.27 pg/mL for IL-12, 63.03 pg/mL for IL-13, 2.19 pg/mL for IL-17, 2.39 pg/mL for IFN-γ, 0.31 pg/mL for TNF-α, 6.74 pg/mL for granulocyte monocyte colony-stimulating factor, and 0.49 pg/mL for granulocyte colony-stimulating factor. Any undetectable value for each cytokine was defined as zero. We used the Bio-Plex Manager 4.0 software (Bio-Rad Laboratories, Inc.,) for analysis and defined the working range as within 20% for the intra-assay coefficients of variation. We performed the assay of all samples at once to avoid any interassay variability. The percent recovery was defined at 70%–130% of the working range using Bio-Plex Manager 4.0.
Statistical analyses
Statistical analyses were performed using SPSS 19.0 software (SPSS, Inc., Chicago, IL) with raw scores. The results of the immunoassay measurements were presented as median, minimum, and maximum levels, and nonparametric tests were used for statistical analysis. A 2-tailed chi-square test or the Fisher's exact test was used for the analysis of categorical data. The Student's t-test was used for continuous variables with normal distributions between 2 groups, and the Mann–Whitney test was used for continuous variables without a normal distribution between 2 groups. The analysis of variance was used for continuous variables across 3 groups. Multivariable linear regression was used to identify a relationship between the cytokine profiles and CSF pleocytosis. In all analyses, P-values <0.05 were taken to indicate statistical significance.
Results
Demographic data and CSF analysis
A total of 158 children who underwent a CSF examination that included a virological test and cytokine measurement were enrolled. Of the 158 patients, 101 were in group-A (EVM), 27 in group-B (nonenteroviral aseptic meningitis), and 30 in group-C (control group). Of the group-A, there were 71 patients with CSF pleocytosis (group-A1) and 30 with CSF nonpleocytosis (group-A2).
The proportion of boys in the 3 groups was similar: group-A, 66 (65.3%); group-B, 16 (59.3%); and group-C, 15 (50.0%) (P = 0.307) (Table 1). However, the mean age differed substantially between groups A and B. The children of group-A (mean ± standard deviation, 4.9 ± 3.2 years) were significantly younger than those of group-B (8.4 ± 5.0 years, P = 0.012). Of the 101 patients in group-A, group A2 (3.4 ± 2.8 years) was substantially younger than group-A1 (5.5 ± 3.2 years, P = 0.016) (Table 2). CSF nonpleocytosis was observed in 71.4% (5/7) of infants aged 1–56 days, 62.5% (5/8) of infants aged 57 days to 1 year, 22.9% (11/48) of children aged 1–5 years, and 23.7% (9/38) of children aged 6–16 years (P = 0.006). The proportion of patients with CSF nonpleocytosis was significantly negatively correlated with age (Fig. 1).

Comparison of the proportion of children with nonpleocytosis per age group in children with EVM. EVM, enteroviral meningitis.
Group-A, children of EVM; group-B, children of nonenteroviral aseptic meningitis; group-C, children without central nervous system infection.
P < 0.05.
CRP, C-reactive protein; CSF, cerebrospinal fluid; EVM, enteroviral meningitis; WBC, white blood cell.
Group-A1, children of EVM with pleocytosis; group-A2, children of EVM with nonpleocytosis.
P < 0.05.
A history of fever was noted in 97 (96.0%) children in group-A and 27 (100.0%) in group-B and was significantly more common in both groups than in group-C (21/30, 70.0%) (P < 0.001) (Table 1). Headache was found more often in group-C (27, 90.0%) and group-A (84, 83.2%) compared to group-B (16, 59.3%) (P = 0.007). The mean duration of hospitalization in group-B (12.6 ± 11.1 days) was significantly longer than for those in group-A (5.1 ± 2.1 days, P = 0.002). Children in group-A1 experienced headache (91.5% versus 63.3%, P = 0.001) and vomiting (76.1% versus 50.0%, P = 0.018) significantly more often than those in group-A2 (Table 2). The mean interval period from the onset of these symptoms to LP (1.8 ± 1.1 days versus 1.8 ± 1.3 days, P = 0.577) and the duration of hospitalization (5.3 ± 2.2 days versus 4.7 ± 1.8 days, P = 0.169) was similar in both group-A1 and A2. No poor outcomes were reported in our patients.
The patients in group-B had the highest levels of CSF leukocyte counts (137.3 ± 203.1/mm3) and CSF protein (49.8 ± 30.7 mg/dL) compared with those in groups A (80.2 ± 27.2/mm3, 35.2 ± 22.4 mg/dL) and C (1.4 ± 3.4/mm3, 25.3 ± 9.7 mg/dL), with a significant trend from B to A to C (nonenteroviral aseptic meningitis > EVM > control) for both CSF WBC counts (P = 0.008) and CSF protein levels (P < 0.001) (Table 1). The mean levels of peripheral leukocyte counts and C-reactive protein (CRP) were similar across the 3 groups (Table 1) and between group-A1 and A2 (Table 2).
Cytokine profile between EVM with pleocytosis and with nonpleocytosis
The levels of IL-1β, IL-2, IL-6, IL-8, IL-10, IFN-γ, and TNF-α were significantly higher in the CSF of group-A1 than in that of group-A2 (Fig. 2). Of these 7 cytokines, IL-2, IL-6, IL8, and TNF-α were the highest in group-A1, followed by group-A2 and group-C (EVM with pleocytosis > EVM with nonpleocytosis > control), and IL-1β, IL-10, and IFN-γ were similar between group-A2 and group-C (EVM with pleocytosis > EVM with nonpleocytosis = control). Of all cytokines examined, CSF levels of IL-2 (r 2 = 0.492), IL-6 (r 2 = 0.79), and TNF-α (r 2 = 0.531) were associated with pleocytosis in EVM through multivariable linear regression (data not shown).
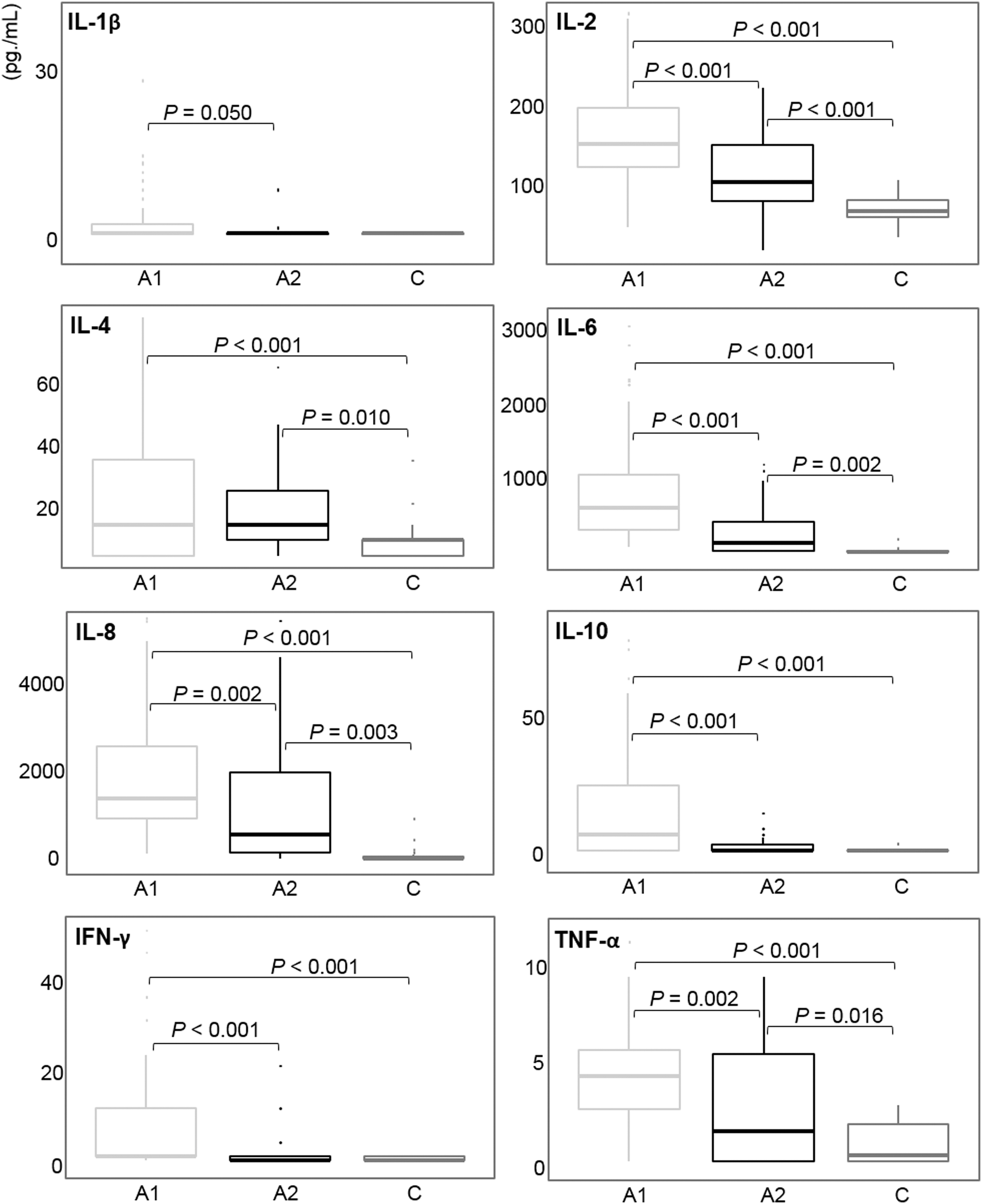
Comparison of the cerebrospinal fluid levels of cytokine profiles among children with EVM with pleocytosis versus nonpleocytosis, and control group (A1, EVM with pleocytosis; A2, EVM with nonpleocytosis, C, control). CSF, cerebrospinal fluid.
Cytokine profile among EVM, nonenteroviral aseptic meningitis, and the control group
Significant differences were found in the IL-2, IL-6, and IL-8 levels in the CSF across the 3 groups (Fig. 3). These cytokines were the highest in group-A, followed by group-B and group-C (EVM > nonenteroviral aseptic meningitis > control). IL-1β, IL-4, IL-10, IFN-γ, and TNF-α were at substantially higher levels in the groups containing children with meningitis than in the control group (EVM = nonenteroviral aseptic meningitis > control).
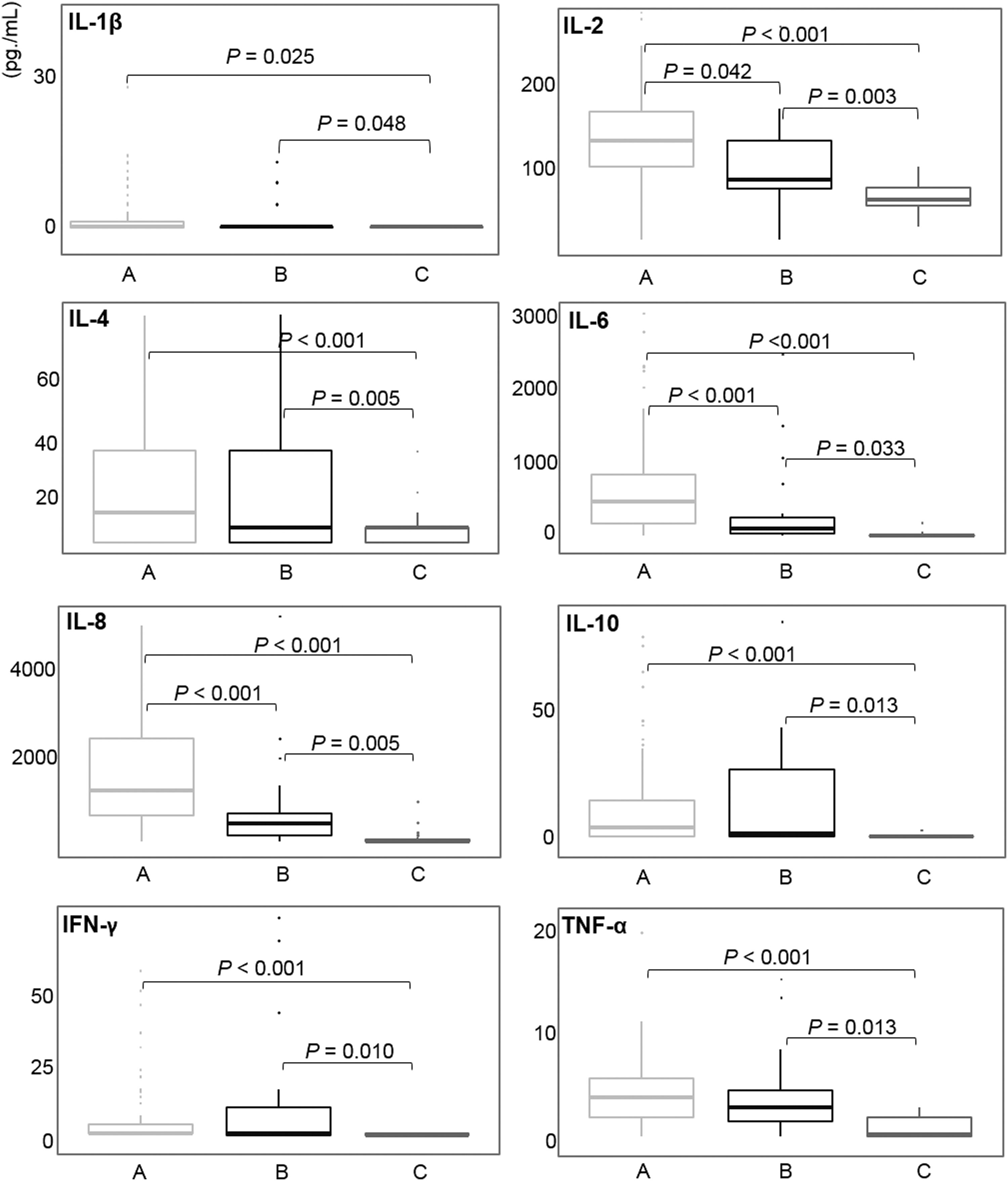
Comparison of the cerebrospinal fluid levels of cytokine profiles among the children with EVM, other aseptic meningitis, and control group (A, EVM; B, nonenteroviral aseptic meningitis; C, control).
Discussion
Pleocytosis in the CSF is a hallmark of meningitis regardless of the etiological agent. Cytokines are potential mediators of cell migration from the blood into the CNS. In this study, we investigated the levels of 15 cytokines in the CSF of children with EVM, nonenteroviral aseptic meningitis, and those in the control group. In our results, IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, IFN-γ, and TNF-α were higher in both viral meningitis groups (group-A and B) than in the control group. Furthermore, IL-2, IL-6, and IL-8 were significantly higher in children with EVM than in those with nonenteroviral aseptic meningitis (EVM > nonenteroviral aseptic meningitis > control). In addition, there was a significant difference between cytokine levels in the CSF of children with EVM with CSF pleocytosis versus those with EVM and nonpleocytosis. IL-1β, IL-2, IL-6, IL-8, IL-10, IFN-γ, and TNF-α were higher in the CSF of EVM cases with pleocytosis than in that of EVM cases with nonpleocytosis. The demographic and laboratory data between EVM children with and without pleocytosis were compared to identify potential variables. The interval periods from onset to LP and peripheral leukocyte and CRP levels were similar between these 2 groups. However, the mean age of the children with EVM and with nonpleocytosis was significantly younger than those with pleocytosis and the proportion of patients with nonpleocytosis had a significant negative correlation with age (Fig. 1). Therefore, we speculate that the elevation of CSF cytokines associated with EVM may be influenced by aging.
Many different cytokines and chemokines control the inflammatory response via activation and migration of WBCs (Sato and others 2003). The results of previous experiments (Utsunomiya and others 1991; Sato and others 2003) indicated that the production of proinflammatory cytokines (IL-1β, IL-6, IL-8, TNF-α, and IFN-γ) stimulated by infection induce the migration of WBCs into the infected area and that inflammation is terminated by anti-inflammatory cytokines (IL-10, IL-4, and transforming growth factor-β1) that are produced after elimination of the microorganisms. In viral meningitis, proinflammatory cytokines, including IL-6, IL-8, and IFN-γ, were detected at relatively higher levels in the CSF of affected patients (Ohga and others 1994; Ishiguro and others 1997). Anti-inflammatory cytokines were also detected in the CSF in the early stages of the illness (Ishiguro and others 1996). It has been suggested that those cytokines might play an important role in the inflammatory process in viral meningitis. Our results support the theory that the production of proinflammatory cytokines is enhanced in children with EVM and pleocytosis than in those with EVM but without pleocytosis.
Dalal and others (2003) demonstrated that IL-6 and IFN-γ were elevated in the CSF of patients with echovirus type 4 meningitis and that the IL-6 level was correlated with the CSF leukocyte count. In pediatric patients, 2 studies revealed a positive correlation between CSF leukocytes and IL-6 and IFN-γ, respectively (Ohga and others 1994; Azuma and others 1997). Asano and others reported that IFN-γ only correlated with CSF pleocytosis in children with mumps meningitis (Asano and others 2011). Our study found that the CSF levels of IL-2, IL-6, and TNF-α were associated with pleocytosis in EVM. In contrast, others demonstrated no correlation between IL-6 or TNF-α levels and CSF leukocyte counts (Glimåker and others 1993; Dulkerian and others 1995).
The reason for the lack of correlation between numerous cytokine levels and leukocytes counts in the CSF, as observed in some studies, may be elucidated as follows. First, the timing of sampling can be important. Ishiguro and others showed differences in the IL-8 levels with time (Ishiguro and others 1997). Second, individual genetic or immune factors may influence the amount of immune response to the etiologic agents (Täuber and others 1999). Third, previous interventions, such as steroids before the presentation of meningitis, may affect the leukocyte counts and cytokine production. The interval period of LP for CSF sampling was similar in our patient population and the patients and had no previous medication or interventions. The levels of IL-2, IL-6, and TNF-α were associated with CSF pleocytosis in our children with EVM, although the correlation between specific cytokines levels and each type of enteroviruses was not investigated in this study.
The variability in the CSF levels of various cytokines may depend on the specific viral pathogen of meningitis, which may describe the discrepancy in various reports. Glimåker and others reported that the levels of IL-8, IL-10, IL-12, IL-13, and IFN-γ were more increased in mumps meningitis than in other types of viral meningitis and controls (Glimåker and others 1993). These studies emphasized that mumps meningitis causes a distinct immunological response when compared with other viral meningitides. Ichiyama and others demonstrated that the CSF cytokine profile in mumps meningitis was different from that in echovirus type 30 meningitis. They suggested that the higher level of CSF IL-6 in echovirus meningitis than that in mumps meningitis may indicate that IL-6 is mostly produced by monocytes/macrophages (Ichiyama and others 2005). Wang and others revealed a significant association between CSF levels of IL-1β, IL-6, and IFN-γ and the severity of enterovirus 71 brainstem encephalitis, and IFN-γ seems to play a more prominent role in the overwhelming disease process caused by enterovirus 71 (Wang and others 2007). Another recent study reported that higher granulocyte monocyte colony-stimulating factor levels were detected in the serum of Japanese encephalitis patients than in Dengue virus patients or in healthy controls, and levels of granulocyte monocyte colony-stimulating factor, IL-6, and monocyte chemoattractant protein-1 were higher in the CSF than serum in both Dengue and Japanese encephalitis virus infection (Li and others 2017). In our center, the viral studies of these flavivirus such as West Nile virus, Dengue virus, Japanese encephalitis virus, yellow fever virus, and Zika virus were not performed in routine CSF examination, because of very rare incidence in our country and nonendemic area. We just determined to carry out these viral studies for the patients who had the congruent symptoms or signs following a travel history to an endemic area. We also have, not routinely, examined the mumps viral study to only the children who had the usual symptoms or signs of mumps viral meningitis, such as fever, headache, and painful swelling of 1 or both parotid salivary glands. No patients with above history or clinical feature were enrolled in present study.
This study has several limitations. First, the levels of CSF cytokine profiles according to the type-based enterovirus were not evaluated and analyzed, which precluded the correlations between specific enteroviruses and cytokine expression profiles. Second, the selection bias of the cytokine/chemokine profiles can be in methods. More different chemokines known to be major attractants of immune cells into the sites of infection (such as CCL2, CCL3, CCL5, and CXCL10, etc.) were not investigated. Third, the levels of blood cytokines at the same time of CSF collection were not examined. Finally, the possibility of false-positive enteroviral RT-PCR in EVM patients with CSF nonpleocytosis should be considered. However, both of the clinical sensitivity and specificity for enteroviral detection in the GeneXpert assay have been documented to be high (Kost and others 2007), and all CSF samples from all patients were examined using the same test tool (GeneXpert assay). In addition, the retest of CSF by LP was difficult to accomplish because of the patients' favorable condition and fast recovery.
In conclusion, lack of CSF pleocytosis, which was commonly observed in children with EVM, was associated with significantly lower levels of some CSF cytokines than in children with EVM with pleocytosis. Also, children with EVM with nonpleocytosis were substantially younger than those with pleocytosis. Therefore, CSF enteroviral RT-PCR testing may be necessary to detect enterovirus in the CNS, especially in young infants, despite CSF nonpleocytosis. Further detailed study should be needed whether there is a correlation between cytokine expression profiles and specific enteroviruses.
Footnotes
Acknowledgments
This study was supported by Research Institute for Convergence of Biomedical Science and Technology Grant (30-2015-019), Pusan National University Yangsan Hospital. This study was provided with biospecimens and clinical data from the Institutional Biobank Project (OF-2016-01) according to the individual research protocol.
Author Disclosure Statement
No competing financial interests exist.