
Abstract
Interleukin-35 (IL-35) is a critical anti-inflammatory cytokine in autoimmune disease. In the current study, we aimed to investigate the serum IL-35 levels and its clinical association in patients with primary Sjögren's syndrome (pSS) and to investigate whether or not IL-35 participates in the pathogenesis of pSS. One hundred seventy-six pSS patients and 60 healthy controls (HCs) were recruited. Disease activity was assessed according to EULAR SS disease activity index. Serum IL-35 levels were quantified by enzyme-linked immunosorbent assay. The correlations between the serum IL-35 levels with the clinical parameters were analyzed by a Spearman's correlation test. The serum IL-35 levels in the patients with pSS were significantly increased compared with the HCs. The serum IL-35 levels were elevated in the patients with pSS. Strikingly, the serum IL-35 levels in pSS patients with short disease duration (<1 year) were significantly lower compared with HCs. However, the serum IL-35 levels in pSS patients with medium (1–2 year) and long disease duration (>2 years) were higher compared with HCs. We also found a positive correlation between expression of IL-35 and erythrocyte sedimentation rate, disease activity, and immunoglobulin G. Furthermore, the pSS patients with RF-positive showed high serum IL-35 levels. These findings suggest that IL-35 could play a key role in pSS pathogenesis. In addition, our results highlight the potential exploitation of IL-35 as a biomarker of disease activity and may represent a novel therapeutic agent for pSS.
Introduction
P
IL-35 (interleukin-35) is a newly discovered cytokine by Collison and others in 2007, which is reported to be a potent immunosuppressive and anti-inflammatory cytokine. IL-35 is a stimulatory cytokine heterodimer composed of 2 subunits of p35 and Epstein Barr virus Induced gene 3 (EBI3), which shares the commonality of the IL-12 family (Collison and others 2007; Niedbala and others 2007). Despite the obvious structural similarities in the cytokine subunits, receptor components, and downstream signaling, unlike the other members, IL-35 is expressed predominantly by regulatory T cells (Tregs) and appears to be a requirement for maximal suppression of mouse and human Tregs (Collison and others 2009; Chaturvedi and others 2013). Previous studies reported that the expression of IL-35 in some nonimmune cell types of cancer cells is also beginning to emerge, such as pancreatic cancer cells (Nicholl and others 2014), nasopharyngeal carcinoma (Zhang and others 2015), melanoma, and breast cancer cells (Wang and others 2013).
IL-35 has been shown to mediate intracellular signaling either through the heterodimer of receptor chains IL-12Rβ2/gp130 or homodimer of each chain mediated by STAT1 and STAT4 (Collison and others 2012). In mice models, the role of IL-35 has also been explored. IL-35 can induce an inhibitory subset of Foxp3−IL-35+Treg cells (iTr35s) that suppress inflammation in experimental autoimmune encephalomyelitis (EAE) models (Choi and others 2017). The EBI3-p35 fusion protein expressed in mammalian cells was biologically active by inducing the expansion of Tregs and suppressing differentiation of Th17 cells in collagen-induced arthritis (CIA) (Niedbala and others 2007). In human disease, the role of IL-35 has been reported in several autoimmune diseases, such as rheumatoid arthritis (Nakano and others 2015), systemic lupus erythematosus (Ouyang and others 2014), systemic sclerosis (Dantas and others 2015; Tomcik and others 2015), and so on.
Therefore, we inferred that IL-35 performed as an endogenous regulator to reduce inflammation in autoimmune diseases. In the present study, we detected the serum IL-35 levels in patients with pSS to explore the serum IL-35 levels and its clinical association and to probe whether or not IL-35 involves in the pathogenesis of pSS.
Materials and Methods
Patients
A total of 176 patients with pSS were enrolled in the Department of Rheumatology and Immunology of the First Affiliated Hospital of China Medical University from January 2016 to April 2017. Sixty healthy subjects without any chronic inflammatory disease were randomly selected as the healthy controls (HCs). The laboratory parameters, including anti-SSA/Ro antibodies, anti-SSB/La antibodies, rheumatoid factor (RF), erythrocyte sedimentation rate (ESR), immunoglobulin (Ig) G, and other clinical parameters, were collected at the same time. All patients with pSS fulfilled the 2002 American-European Consensus Group classification criteria. EULAR Sjogren's Syndrome Disease Activity Index (ESSDAI) was used to evaluate the disease activity status (Seror and others 2010). ILD was assessed on high-resolution computed tomography. All patients with infections, tumors, and other non-pSS autoimmune diseases were excluded. The experimental group and the control group of gender and age showed no significant difference. The study was approved by the Ethics Committee of the First Affiliated Hospital of China Medical University, and written informed consent was obtained by each subject.
Serum IL-35 levels assay
Serum from all patients and HCs by centrifugation of peripheral blood samples was frozen at −80°C. Serum IL-35 levels were determined using commercially available Enzyme Linked Immunosorbent Assay (ELISA) Kit (No. SY-H7912; Shanghai ShuangYing, China) according to the manufacturer's protocol. This immunoassay has been shown to accurately quantitate human IL-35 in serum and free of interference from IL-12p70 and/or IL-27p50. A standard curve was generated for each plate, and the absolute serum IL-35 levels were calculated. Detection range is 2–50 ng/L.
Statistical analysis
Data were analyzed to compute median or the mean ± SE. Continuous variables from the study were processed by the ANOVA and/or the Student's t-test with a parametric distribution or the Mann–Whitney U test with a nonparametric distribution. Spearman's correlation coefficient was used to assess the associations between 2 variables. All analyses were performed using SPSS17.0 (SPSS, Inc., Chicago, IL) and GraphPad 5 software. Differences of P < 0.05 were considered significant.
Results
Clinical characteristics of pSS patients
Demographic and clinical characteristics of pSS patients are shown in Table 1. Among these 176 patients, 150 (85.2%) were anti-SSA/Ro positive, 81 (46.1%) were anti-SSB/La positive, 86 (48.9%) were RF positive, 54 (49.1%) had ILD, 23 (13.1%) had Raynaud's phenomenon, 46 (21.6%) had AITD, 20 (11.4%) had AIH, 22 (12.5%) had salivary gland swelling, and 6 (3.4%) had RTA (Table 1).
AITD, autoimmune thyroid disease; AIH, autoimmune hepatitis; CTX, cyclophosphamide; ESR, erythrocyte sedimentation rate; ESSDAI, EULAR Sjögren's syndrome disease activity index; HCQ, hydroxychloroquine; HCs, healthy controls; Ig, immunoglobulin; ILD, interstitial lung disease; LEF, leflunomide; MMF, mycophenolate mofetil; NA, not applicable; pSS, primary Sjögren's syndrome; RF, rheumatoid factor; RTA, renal tubular acidosis; TG, tripterygium glycosides.
Increased serum IL-35 levels in patients with pSS
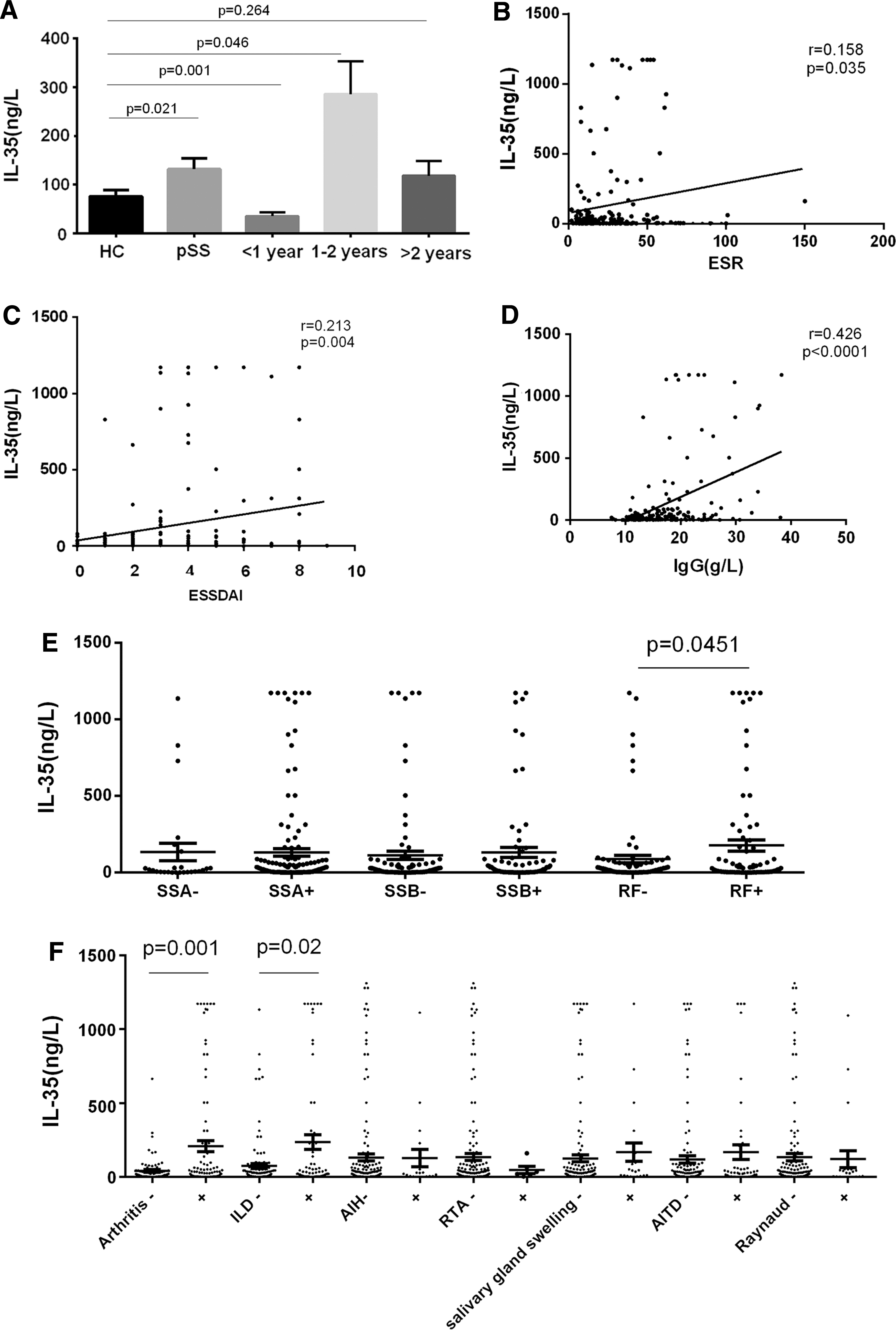
Serum IL-35 levels in pSS patients were higher than those in HCs (mean ± SE, ng/L: 131.9 ± 22.0 versus 76.4 ± 12.6, P = 0.021) (Fig. 1A). Furthermore, patients with short disease duration (<1 year) had lower serum IL-35 levels compared with HCs (mean ± SE, ng/L: 35.5 ± 8.2 versus 76.4 ± 12.6) (P = 0.001). The serum IL-35 levels were significantly higher in medium disease duration (1–2 year) compared to HCs (mean ± SE, ng/L: 285.9 ± 66.9 versus 131.9 ± 22.0, P = 0.046). However, there was no difference in the serum IL-35 levels between the patients with long disease duration (>2 years) and HCs (P = 0.264). The logistical regression analysis, which was performed to exclude the interactions between medical type and IL-35 levels, showed no associations of IL-35 levels with medical types in patients with pSS (P > 0.05) (data are shown in Supplementary Table S1; Supplementary Data are available online at
Correlation between serum IL-35 levels and autoantibody production in patients with pSS
As shown in Fig. 1E, no significant difference was found in serum IL-35 levels between pSS patients with anti-SSA/Ro, anti-SSB/La, and without. Interestingly, the serum IL-35 levels were significantly higher in the RF-positive group compared with the RF-negative group (P = 0.0451) (Fig. 1E).
Correlation between serum IL-35 levels and systemic involvement in pSS patients
In pSS patients, the serum IL-35 levels in the pSS with arthritis or ILD were higher than those without arthritis or ILD, respectively (P = 0.001, P = 0.02, respectively). However, no correlation was found between serum IL-35 levels and other manifestations in patients with pSS, including Raynaud's phenomenon, salivary gland swelling, AITD, AIH, and RTA (Raynaud's phenomenon: P = 0.855, salivary gland swelling: P = 0.99, AITD: P = 0.33, AIH: P = 0.93, RTA: P = 0.628) (Fig. 1F).
Discussion
According to current research, IL-35 is involved in the development of various autoimmune diseases. Our study showed that serum IL-35 levels in patients with pSS were significantly higher than HCs. We could speculate that the endogenous elevation of IL-35 may be involved in the negative feedback immune regulation stimulated by inflammatory factors, which could neutralize excessive inflammatory response, and finally plays a protective role in patients with pSS. Furthermore, we found a significant correlation between serum IL-35 levels and disease activity, including ESR and ESSDAI. These observations provide a clue that the IL-35 can be utilized to determine disease activity of pSS, further suggesting that IL-35 is closely related to the inflammatory state of pSS patients. However, the specific mechanism about how IL-35 functions in pSS still need investigation.
In addition, we found a positive correlation between serum IL-35 levels and serum B cell activation biomarker IgG, suggesting that IL-35 may be a treatment target especially for pSS patients with high Ig. Therefore, serum IL-35 levels can be used to evaluate the disease activity of pSS, further suggesting that IL-35 is closely related to the inflammatory state of pSS patients and may be involved in the pathogenesis of pSS.
Interestingly, the opposite results were obtained by Fogel and others (2017). They detected lower spontaneous serum IL-35 levels in pSS patients compared with HCs. However, the population that they studied was not classified specifically with disease duration. Our study found that serum IL-35 levels were associated with disease duration in patients with pSS indicating that IL-35 may play different roles in different stages of pSS. However, the specific mechanism still needs to be elucidated.
In this study, we, for the first time, reported that the serum IL-35 levels were particularly elevated in the RF-positive patients. However, we did not show the relationship between IL-35 and other antibodies, including anti-SSA/Ro and anti-SSB/La. The reason for that may be several reasons. First, anti-SSA/Ro and anti-SSB/La have been applied to the diagnosis of pSS, but none of these autoantibodies provides sufficient specificity and sensitivity (Kyriakidis and others 2014). Second, our study had limitations, including small population and the lack of study on molecular mechanisms underlying the role of IL-35 in the pathogenesis of pSS. Therefore further studies in a bigger sample size to solve these limitations are warranted. More studies from in vivo experimental models are needed to explore the particular role of IL-35 in the pathogenesis of pSS.
To better apprehend the role of IL-35 in the pathophysiology of pSS, we tried to figure out the correlation between IL-35 and relevant systemic involvement of pSS (eg, arthritis, ILD, and AIH). PSS occurs in association with other extraglandular complications, particularly arthritis (Uhlig and others 1999). In our study, the prevalence of arthritis was 56.0%. This is the first study to report the association of IL-35 with arthritis in pSS. Previous study reported that IL-35 restrained the progression of arthritis in CIA mice (Li and others 2016). However, the mechanism of IL-35 in pSS with arthritis is still not clear. ILD is also a common and severe complication of pSS. The prevalence of ILD in pSS patients is ∼8% (Gardiner 1993). In the present work, we found an increment of IL-35 in pSS patients with arthritis or ILD compared with and those with pSS alone. Although AIH, RTA, salivary gland swelling, AIHD, and Raynaud's phenomenon are also common manifestations in patients with pSS, we did not show the correlation between IL-35 and pSS with above manifestations. These may suggest a complex interaction between IL-35 and systemic involvements in pSS, which still needs to be further investigated.
Conclusions
IL-35 may play some part in the development of pSS and potentially contribute to the development of arthritis or ILD in pSS. In this study, we only reported associations between IL-35 and pSS; further studies are needed to discover the mechanism involved in pSS.
Footnotes
Acknowledgment
This study was supported by the National Natural Science Foundation of China (grant no. 81273248 and 81471542).
Author Disclosure Statement
All authors declared no conflicts of interest.